
Your practice is where vaccine confidence gets built.
Join an AAFP immunization initiative and get the tools, training and support to strengthen every immunization conversation in your practice. Just 25 practices per program. Apply by Aug. 10. Explore programs.
Respiratory virus vaccines: Clinical guidance and resources

Respiratory virus vaccines remain essential tools for preventing serious complications.
All adults, children and families should stay up to date on recommended vaccines to keep themselves and their loved ones healthy. On this page, you’ll find guidance that provides an overview of respiratory virus vaccine recommendations and counseling techniques.
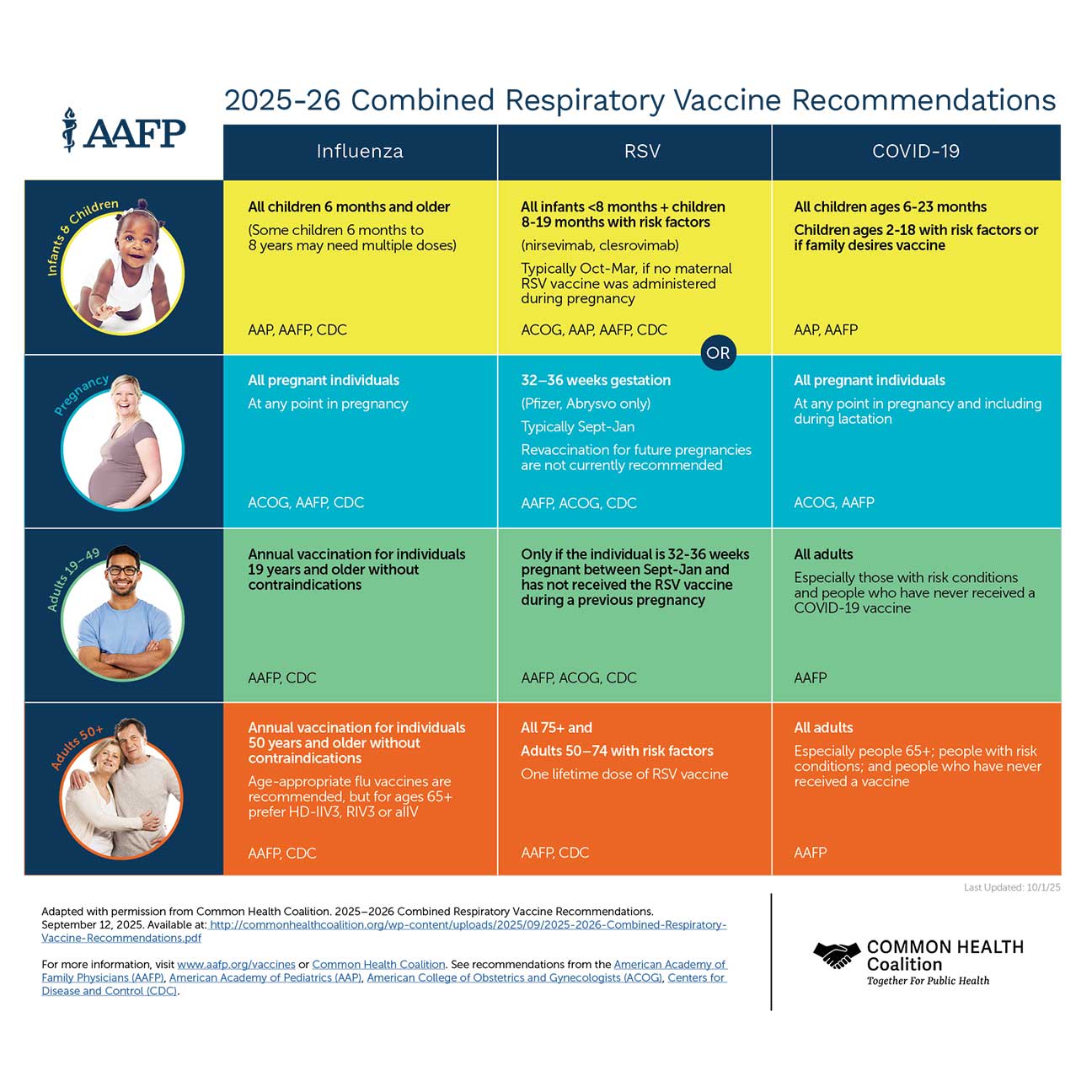
2025 to 2026 combined respiratory vaccine recommendations
Visit our immunization and vaccines page for our full vaccine schedules.
COVID treatment
COVID-19 remains a public health concern affecting patients in every community. The AAFP will continue to provide information on the following COVID-19-related topics to help you in your practice and patient care. Key findings from the CDC’s “Preventing Chronic Disease, Public Health Research, Practice and Policy” found:
Several underlying medical conditions were associated with an increased risk for severe COVID-19 illness in adults.
Obesity, diabetes with complications and anxiety and fear-related disorders had the strongest association with death.
Read the full clinical guidance.
Shared decision-making considerations
Shared decision-making is key to effective COVID-19 treatment conversations. It involves you and your patient working together to make decisions about their treatment plan based on the best available evidence. Benefits of this approach include increasing the patient’s understanding of their condition and available treatment options, improving patient-physician communication, building trust and increasing patient satisfaction. Research has also shown that prioritizing patients’ involvement in clinic visits and encouraging them to take a more active role in decision-making leads to positive health outcomes. A collaborative approach can be particularly useful when treating patients at higher risk of severe COVID-19 outcomes.
Download the AAFP’s conversation guide: Shared decision-making considerations for COVID-19 treatment (PDF).
COVID-19 vaccines
COVID-19 vaccines offer high levels of protection against severe disease, hospitalization and death, especially for people who receive boosters.
Family physicians and other primary care clinicians are trusted sources of health information. As you care for patients of all ages, use these evidence-based resources to strongly recommend COVID-19 vaccination. Download the 2025-26 recommendations (PDF).
Navigating COVID vaccine conversations with patients
Conversation tool: Closing the gaps
Pregnancy
Pregnant women are at increased risk of severe COVID-19 infection, intensive care unit admission and death, as well as adverse pregnancy outcomes. The best protection against potential harm is to receive the COVID-19 vaccine. Patients can safely receive the vaccine at any stage of pregnancy. One dose of the bivalent vaccine (Moderna or Pfizer) is recommended for optimal protection, regardless of whether the patient received any original COVID-19 vaccines.
Coding and payment
The AMA updates COVID-19 vaccine and administration codes. The unique structure of these codes allows for tracking and accommodating multiple COVID-19 vaccines.
Coding and payment guidance
How to code third doses of COVID-19 vaccines: These codes are only to be used for third doses for immunocompromised individuals, which are different than booster shots.
COVID-19 vaccine coverage requirements and preliminary payment guidance: Information on coverage for vaccine administration and related services.
Long COVID
Long COVID—sometimes called long-haul COVID, chronic COVID or post-acute sequelae of SARS-CoV-2 infection (PASC)—is a complex and variable chronic condition that can persist long after the acute phase of COVID-19 infection. Symptoms range from mild to debilitating and often fluctuate over time. These symptoms can affect anyone who has had COVID-19, even if their initial infection was mild or did not cause symptoms. The best way to reduce the risk of developing long COVID is by getting vaccinated against COVID-19. Evidence shows people who are fully vaccinated are less likely to experience severe COVID-19 illness, which, in turn, can decrease their likelihood of developing long COVID.
Family physicians are essential in providing care for patients experiencing long COVID, offering support, coordination and access to resources that address this complex condition.
Symptoms
Documentation of a positive COVID-19 test is not required to diagnose long COVID. Long COVID encompasses a variety of symptoms that may affect multiple organ systems, ranging in severity and duration. Symptoms often fluctuate over time and can significantly impact daily functioning.
Long COVID common symptoms
Fatigue or post-exertional malaise (PEM)
Shortness of breath or difficulty breathing
Cognitive impairment or brain fog
Chest pain or heart palpitations
Joint and muscle pain
Sleep disturbances, headaches and rashes
Impaired ability to perform daily activities
Disability classification
Under guidance from the U.S. Department of Health and Human Services (HHS), long COVID may qualify as a disability under the Americans with Disabilities Act (ADA). This designation ensures patients experiencing significant limitations due to long COVID are eligible for workplace or school accommodations. For additional information, visit HHS’s long COVID disability resources.
Influenza prevention and control
Family physicians and care teams can protect patients from severe illness and health complications by strongly recommending influenza vaccination as soon as it is available each year and providing the vaccine throughout the flu season. Annual flu vaccination is recommended for everyone aged 6 months and older without medical contraindications.
Influenza prevention resources
Respiratory syncytial virus (RSV)
Respiratory syncytial virus (RSV) is a common virus that affects the lungs, making breathing difficult. The virus is common in children under age 2, though people of all ages can contract it. It is more serious for young and premature babies, and older adults with poor health.
RSV resources
Increasing respiratory syncytial virus (RSV) vaccination in adults 60 and older
Get up-to-date guidance to help you identify patients at higher risk for severe RSV and support informed conversations about vaccination. These resources cover recommendations from the Advisory Committee on Immunization Practices, available vaccines, key risk factors and practical strategies for discussing RSV vaccination with adults 60 and older.
Immunization awareness
Patient education
The AAFP patient education website, FamilyDoctor.org, provides many patient-facing resources.