
Adults 19 and older immunization schedules
The most current vaccine recommendations for adults based on age group and medical indications.
The CDC's 2025 immunization schedules, which are not endorsed by the AAFP, can be found here.
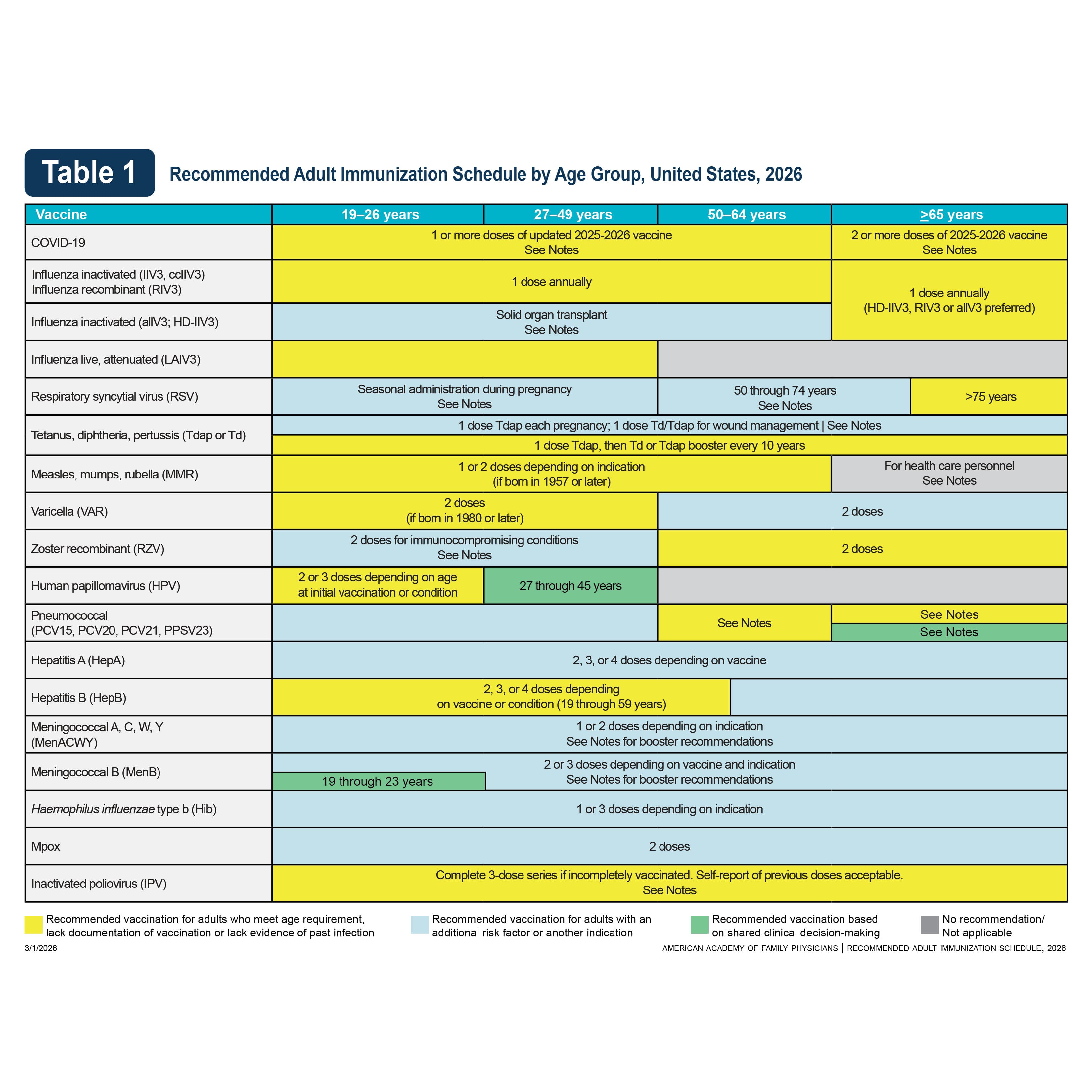
Schedule based on age group
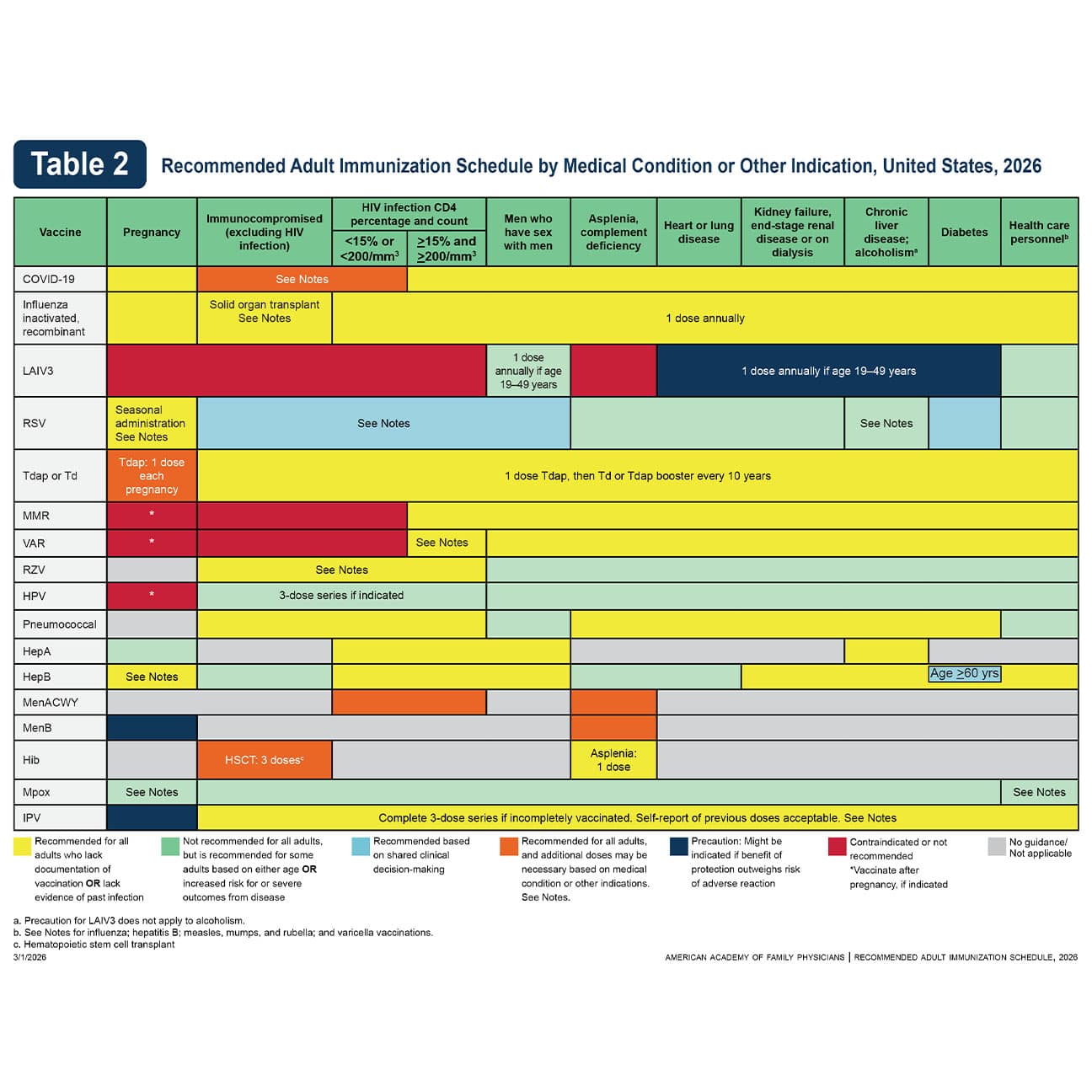
Schedule based on medical condition or other indication
Notes
- For calculating intervals between doses, 4 weeks = 28 days. Intervals of ≥4 months are determined by calendar months.
- Within a number range (e.g., 12–18), a dash (–) should be read as “through.”
- Vaccine doses administered ≤4 days before the minimum age or interval are considered valid. Doses of any vaccine administered ≥5 days earlier than the minimum age or minimum interval should not be counted as valid and should be repeated. The repeat dose should be spaced after the invalid dose by the recommended minimum interval.
- Information on travel vaccination requirements and recommendations is available at www.cdc.gov/travel.
- For information about vaccination in the setting of a vaccine–preventable disease outbreak, contact your state or local health department.
- The National Vaccine Injury Compensation Program (VICP) is a no-fault alternative to the traditional legal system for resolving vaccine injury claims. All vaccines included in the adult immunization schedule except PPSV23, RSV, RZV, mpox and COVID–19 vaccines are covered by the VICP. COVID-19 vaccines that are authorized or approved by the FDA are covered by the Countermeasures Injury Compensation Program (CICP). For more information, see National Vaccine Injury Compensation Program or www. hrsa.gov/cicp.
Routine vaccination
Age 19 to 64 years
- Unvaccinated
- 1 dose Spikevax or mNexspike or Comirnaty or Nuvaxovid
- Previously vaccinated before 2025-26 vaccine with:
- 1 or more doses Spikevax or Comirnaty: 1 dose Spikevax or Nuvaxovid or Comirnaty at least8 weeks after the most recent dose or 1 dose mNexspike at least 12 weeks after the most recent dose.
- 1 dose Nuvaxovid: 1 dose Nuvaxovid 3–8 weeks after most recent dose. If more than 8 weeks after most recent dose, administer 1 dose Spikevax or Nuvaxovid or Comirnaty or 1 dose mNexspike at least 12 weeks after the most recent dose.
- 2 or more doses Nuvaxovid: 1 dose Spikevax or Nuvaxovid or Comirnaty at least 8 weeks after the most recent dose or 1 dose mNexspike at least 12 weeks after the most recent dose.
- 1 or more doses Janssen: 1 dose Spikevax or mNexspike or Nuvaxovid or Comirnaty.
Age 65 years and older
- Unvaccinated: Follow recommendations above for unvaccinated persons ages 19 to 64 years and administer dose 2 of Spikevax or mNexspike or Nuvaxovid or Comirnaty 6 months later (minimum interval: 2 months).
- Previously vaccinated before 2025-26 vaccine: follow recommendations above for previously vaccinated persons ages 19 to 64 years and administer dose 2 of Spikevax or mNexspike or Nuvaxovid or Comirnaty 6 months later (minimum interval: 2 months).
Special situations
Persons who are moderately or severely immunocompromised:
Use vaccine from the same manufacturer for all doses in the initial vaccination series.
- Unvaccinated:
- 4 doses (3-dose initial series Spikevax or mNexspike at 0, 4 weeks, and at least 4 weeks after dose 2, followed by 1 dose Spikevax or mNexspike or Nuvaxovid or Comirnaty 6 months later [minimum interval: 2 months]); May administer additional doses.*
- 4 doses (3-dose initial series Comirnaty at 0, 3 weeks, and at least 4 weeks after dose 2, followed by 1 dose of Spikevax or mNexspike or Nuvaxovid or Comirnaty 6 months later [minimum interval: 2 months]); May administer additional doses.*
- 3 doses (2-dose initial series Nuvaxovid at 0, 3 weeks, followed by 1 dose Spikevax or mNexspike or Nuvaxovid or Comirnaty 6 months later [minimum interval: 2 months]); May administer additional doses.*
- Incomplete initial vaccination series before 2025–26 vaccine
- Previous vaccination with Spikevax
- 1 dose Spikevax: completeinitial series with 2 doses of Spikevax at least 4 weeks apart (administer dose 1 4 weeks after most recent dose), followed by 1 dose Spikevax or mNexspike or Nuvaxovid or Comirnaty 6 months later (minimum interval: 2 months). May administer additional doses.*
- 2 doses Spikevax: complete initial series with 1 dose Spikevax at least 4 weeks after most recent dose, followed by 1 dose Spikevax or mNexspike or Nuvaxovid or Comirnaty 6 months later (minimum interval: 2 months). May administer additional doses.*
- Previous vaccination with Comirnaty
- 1 dose Comirnaty: complete initial series with 2 doses of Comirnaty at least 4 weeks apart (administer dose 1 3 weeks after most recent dose), followed by 1 dose of Spikevax or mNexspike or Nuvaxovid or Comirnaty 6 months later (minimum interval: 2 months). May administer additional doses.*
- 2 doses Comirnaty: complete initial series with 1 dose of Comirnaty at least 4 weeks after most recent dose, followed by 1 dose of Spikevax or mNexspike or Nuvaxovid or Comirnaty 6 months later (minimum interval: 2 months). May administer additional doses.*
- Previous vaccination with Nuvaxovid
- 1 dose Nuvaxovid: complete initial series with 1 dose of Nuvaxovid at least 3 weeks after most recent dose, followed by 1 dose of Spikevax or mNexspike or Nuvaxovid or Comirnaty 6 months later (minimum interval: 2 months). May administer additional doses.*
- Completed the initial vaccination series before 2025–26 vaccine with:
- 3 or more doses Spikevax or 3 or more doses Comirnaty: 2 doses of Spikevax or mNexspike or Nuvaxovid or Comirnaty 6 months apart (minimum interval: 2 months). Administer dose 1 at least 8 weeks after the most recent dose. May administer additional doses.*
- 2 or more doses Nuvaxovid: 2 doses of Spikevax or mNexspike or Nuvaxovid or Comirnaty 6 months apart (minimum interval: 2 months). Administer dose 1 at least 8 weeks after the most recent dose. May administer additional doses.*
- Previous vaccination with Spikevax
*Additional doses of COVID-19 vaccine for moderately or severely immunocompromised: based on shared clinical decision-making and administered at least 2 months after the most recent dose.
Special situations
- Anatomical or functional asplenia (including sickle cell disease): 1 dose if previously did not receive Hib vaccine.
- Elective splenectomy: 1 dose preferably at least 14 days before splenectomy.
- Hematopoietic stem cell transplant (HSCT): 3-dose series 4 weeks apart starting 6–12 months after successful transplant, regardless of Hib vaccination history.
Routine vaccination
Any person who is not fully vaccinated and requests vaccination (identification of risk factor not required): 2-dose series HepA (Havrix 6–12 months apart or Vaqta 6–18 months apart [minimum interval: 6 months]) or 3-dose series HepA-HepB (Twinrix at 0, 1, 6 months [minimum intervals: dose 1 to dose 2: 4 weeks / dose 2 to dose 3: 5 months])
Special situations
- Any person who is not fully vaccinated and who is at risk for hepatitis A virus infection or severe disease from hepatitis A virus infection: complete 2-dose series HepA or 3-dose series HepA-HepB as above. Risk factors include:
- Chronic liver disease, including persons with hepatitis C, cirrhosis, fatty liver disease, alcoholic liver disease, autoimmune hepatitis, alanine aminotransferase (ALT) or aspartate aminotransferase (AST) level greater than twice the upper limit of normal.
- HIV infection
- Men who have sex with men
- Injection or non-injection drug use
- Persons experiencing homelessness
- Work with hepatitis A virus in research laboratory or with nonhuman primates with hepatitis A virus infection
- Travel in countries with high or intermediate endemic hepatitis A (HepA-HepB [Twinrix] may be administered on an accelerated schedule of 3 doses at 0, 7 and 21–30 days, followed by a booster dose at 12 months).
- Close, personal contact with international adoptee (e.g., household or regular babysitting) in first 60 days after arrival from country with high or intermediate endemic hepatitis A: dose 1 as soon as adoption is planned; preferably at least 2 weeks before adoptee’s arrival.
- Pregnancy if at risk for infection or severe outcome from infection during pregnancy.
- Settings for exposure, including health care settings targeting services to injection or noninjection drug users or group homes and nonresidential day care facilities for developmentally disabled persons (individual risk factor screening not required)
Routine vaccination
- Age 19 through 59 years: complete a 2- or 3- or 4-dose series
- 2-dose series only applies when 2 doses of Heplisav-B are used at least 4 weeks apart
- 3-dose series Engerix-B, or Recombivax HB at 0, 1, 6 months (minimum intervals: dose 1 to dose 2: 4 weeks / dose 2 to dose 3: 8 weeks / dose 1 to dose 3: 16 weeks)
- 3-dose series HepA-HepB (Twinrix) at 0, 1, 6 months (minimum intervals: dose 1 to dose 2: 4 weeks; dose 2 to dose 3: 5 months)
- 4-dose series HepA-HepB (Twinrix) accelerated schedule of 3 doses at 0, 7, and 21–30 days, followed by a booster dose at 12 months
Note: A voluntary nationwide recall was initiated in November 2024 for the Hep B vaccine PreHevbrio.
- Age 60 or older with known risk factors for hepatitis B virus infection should receive a HepB vaccine series.
- Any adult age 60 years of age or older who requests HepB vaccination should receive a HepB vaccine series.
- Risk factors for hepatitis B virus infection include:
- Chronic liver disease including persons with hepatitis C, cirrhosis, fatty liver disease, alcoholic liver disease, autoimmune hepatitis, alanine aminotransferase (ALT) or aspartate aminotransferase (AST) level greater than twice the upper limit of normal.
- HIV infection
- Sexual exposure risk (e.g., sex partners of hepatitis B surface antigen [HBsAg]-positive persons; sexually active persons not in mutually monogamous relationships; persons seeking evaluation or treatment for a sexually transmitted infection; men who have sex with men)
- Current or recent injection drug use
- Percutaneous or mucosal risk for exposure to blood (e.g., household contacts of HBsAg positive persons; residents and staff of facilities for developmentally disabled persons; health care and public safety personnel with reasonably anticipated risk for exposure to blood or blood-contaminated body fluids; persons on maintenance dialysis, including in-center or home hemodialysis and peritoneal dialysis persons who are predialysis; patients with diabetes*)
- Incarceration
- Travel in countries with high or intermediate endemic hepatitis B
- Risk factors for hepatitis B virus infection include:
*Age 60 years or older with diabetes: Based on shared clinical decision-making, 2-, 3- or 4-dose series as above.
Special situations
- Patients on dialysis: complete a 3- or 4-dose series
- 3-dose series Recombivax HB at 0, 1, 6 months (Note: Use Dialysis Formulation 1 mL = 40 mcg)
- 4-dose series Engerix-B at 0, 1, 2 and 6 months (Note: Use 2 mL dose instead of the normal adult dose of 1 mL)
- Age 20 years or older with an immunocompromising condition: complete a 2- or 3- or 4-dose series.
- 2-doses series Heplisav-B at 0, 1 months
- 3-dose series Recombivax HB at 0,1, 6 months (Note: Use Dialysis Formulation 1 mL = 40 mcg)
- 4-dose series Engerix-B at 0,1, 2, and 6 months (Note: Use 2 mL dose instead of the normal adult dose of 1 mL)
Routine vaccination
All persons up through age 26 years: 2- or 3-dose series depending on age at initial vaccination or condition.
- Age 9–14 years at initial vaccination and received 1 dose or 2 doses less than 5 months apart: 1 additional dose
- Age 9–14 years at initial vaccination and received 2 doses at least 5 months apart: HPV vaccination series complete, no additional dose needed
- Age 15 years or older at initial vaccination: 3-dose series at 0, 1–2 months, 6 months (minimum intervals: dose 1 to dose 2: 4 weeks / dose 2 to dose 3: 12 weeks / dose 1 to dose 3: 5 months; repeat dose if administered too soon)
No additional dose recommended when any HPV vaccine series of any valency has been completed using the recommended dosing intervals.
Shared clinical decision-making
Adults age 27-45 years: Based on shared clinical decision-making, complete a 2-dose series (if initiated age 9-14 years) or 3-dose series (if initiated ≥15 years)
Special situations
- Age ranges recommended above for routine and catch-up vaccination or shared clinical decision-making also apply in special situations.
- Immunocompromising conditions, including HIV infection: Complete 3-dose series, even for those who initiate vaccination at age 9 through 14 years.
- Pregnancy: Pregnancy testing is not needed before vaccination. HPV vaccination is not recommended until after pregnancy; no intervention needed if inadvertently vaccinated while pregnant.
Routine vaccination
- Age 19 years or older: 1 dose any influenza vaccine appropriate for age and health status annually.
- Solid organ transplant recipients ages 19 through 64 years receiving immunosuppressive medications: HD-IIV3 and aIIV3 are acceptable options. No preference over other age-appropriate IIV3 or RIV3.
- Age 65 years or older: Any one of HD-IIV3, RIV3, or aIIV3 is preferred. If none of these three vaccines is available, then any other age-appropriate influenza vaccine should be used.
FluMist (LAIV3) for self-or caregiver-administration was approved by the FDA September 2024. Individuals can order FluMist for delivery to eligible recipients. Screening for eligibility is performed by central pharmacy or primary care clinician, based on screening criteria.
FluMist has been approved for self-administration for persons aged ≥18 years or administration by a caregiver who is ≥18 years for recipients aged 2 through 17 years. FluMist (LAIV3) will continue to be available for administration by health care professionals as previously recommended. No changes are made to recommendations regarding appropriate population, contraindications or precautions.
Special situations
Close contacts (e.g., caregivers, healthcare workers) of severely immunosuppressed persons who require a protected environment: These persons should not receive LAIV3. If LAIV3 is given, they should avoid contact with/caring for such immunosuppressed persons for 7 days after vaccination.
Note: Persons with an egg allergy can receive any influenza vaccine (egg based and non-egg based) appropriate for age and health status.
Routine vaccination
- No evidence of immunity to measles, mumps, or rubella: 1 dose
- Evidence of immunity: Born before 1957 (except for health care personnel, see below), documentation of receipt of MMR vaccine, laboratory evidence of immunity or disease (diagnosis of disease without laboratory confirmation is not evidence of immunity)
Special situations
- Pregnancy with no evidence of immunity to rubella: MMR contraindicated during pregnancy; after pregnancy (before discharge from health care facility), 1 dose
- Nonpregnant persons of childbearing age with no evidence of immunity to rubella: 1 dose
- HIV infection with CD4 percentages ≥15% and CD4 count ≥200 cells/mm3 for at least 6 months and no evidence of immunity to measles, mumps, or rubella: 2-dose series at least 4 weeks apart; MMR contraindicated for HIV infection with CD4 percentage <15% or CD4 count <200 cells/mm3
- Severe immunocompromising conditions: MMR contraindicated
- Students in postsecondary educational institutions, international travelers, and household or close, personal contacts of immunocompromised persons with no evidence of immunity to measles, mumps, or rubella: 2-dose series at least 4 weeks apart if previously did not receive any doses of MMR or 1 dose if previously received 1 dose MMR
- Health care personnel:
- Born before 1957 with no evidence of immunity to measles, mumps, or rubella: Consider 2-dose series at least 4 weeks apart for protection against measles or mumps or 1 dose for protection against rubella.
- Born in 1957 or later with no evidence of immunity to measles, mumps, or rubella: Complete 2-dose series at least 4 weeks apart for protection against measles or mumps or at least 1 dose for protection against rubella.
Special situations for MenACWY
- Anatomical or functional asplenia (including sickle cell disease), HIV infection, persistent complement component deficiency, complement inhibitor (e.g., eculizumab, ravulizumab) use: 2-dose series Menveo or MenQuadfi at least 8 weeks apart and revaccinate every 5 years if risk remains
- Travel in countries with hyperendemic or epidemic meningococcal disease, or microbiologists routinely exposed to Neisseria meningitidis: 1 dose Menveo or MenQuadfi and revaccinate every 5 years if risk remains
- First-year college students who live in residential housing (if not previously vaccinated at age 16 years or older) or military recruits: 1 dose Menveo or MenQuadfi
Shared clinical decision-making for MenB
- Adolescents and young adults age 16–23 years (age 16–18 years preferred)* not at increased risk for meningococcal disease: based on shared clinical decision–making
- Bexsero or Trumenba (use same brand for all doses): 2-dose series at least 6 months apart (if dose 2 is administered earlier than 6 months, administer dose 3 at least 4 months after dose 2)
*To optimize rapid protection (e.g., for students starting college in less than 6 months), a 3-dose series (0, 1–2, 6 months) may be administered.
Special situations for MenB
- Anatomical or functional asplenia (including sickle cell disease), persistent complement component deficiency, complement inhibitor (e.g., eculizumab, ravulizumab) use, or microbiologists routinely exposed to Neisseria meningitidis
- Bexsero or Trumenba (use same brand for all doses including booster doses): 3-dose primary series at 0, 1–2, 6 months (if dose 2 was administered at least 6 months after dose 1, dose 3 not needed; if dose 3 is administered earlier than 4 months after dose 2, a 4th dose should be administered at least 4 months after dose 3).
- Booster doses: 1 booster dose one year after primary series and every 2-3 years if risk remains
- Pregnancy: Delay MenB until after pregnancy unless at increased risk and vaccination benefits outweigh potential risks.
Note: MenB vaccines may be administered simultaneously with MenACWY vaccines if indicated, but at a different anatomic site, if feasible. Adults may receive a single dose of Penbraya (MenACWY–TT/MenB–FHbp) OR Penmenvy (MenACWY-CRM/MenB-4C) as an alternative to separate administration of MenACWY and MenB when both vaccines would be given on the same clinic day. MenB-containing meningococcal vaccine products from different manufacturers are not interchangeable. Use the same type of MenB-containing vaccine for all doses including booster doses.
- For adults not at increased risk:
- If Penbraya is used for dose 1, then MenB-FHbp (Trumenba) should be administered for dose 2 MenB.
- If Penmenvy is used for dose 1, then MenB-4C (Bexsero) should be administered for dose 2 MenB.
- For adults at increased risk:
- Penbraya or Penmenvy may be used for additional MenACWY and MenB doses (including booster doses) if both vaccines would be given on the same clinic day and if separated by at least 6 months from previous dose.
Penbraya and Penmenvy are not interchangeable. Use the same type of MenB-containing vaccine for all doses including booster doses.
- If previously vaccinated with Trumenba or Penbraya, use Trumenba or Penbraya for subsequent doses.
- If previously vaccinated with Bexsero or Penmenvy, use Bexsero or Penmenvy for subsequent doses.
Special situations
- Any person at risk for mpox infection: 2-dose series, 28 days apart.
- Persons who are gay, bisexual or other MSM; transgender; or nonbinary people who in the past 6 months have had:
- A new diagnosis of at least 1 sexually transmitted disease
- More than 1 sex partner
- Sex at a commercial sex venue.
- Sex in association with a large public event in a geographic area where mpox transmission is occurring.
- Persons who are sexual contacts of the persons described above
- Persons who anticipate experiencing any of the situations described above
- Persons deemed at risk by public health authorities in mpox outbreak settings
- Persons who are gay, bisexual or other MSM; transgender; or nonbinary people who in the past 6 months have had:
- Health care personnel: Vaccination to protect against occupational risk in healthcare settings is not routinely recommended.
Routine vaccination
Age 50 years or older who have:
- Not previously received a PCV13, PCV15, PCV20, or PCV21 or whose previous vaccination history is unknown: 1 dose PCV15 or 1 dose PCV20 or 1 dose PCV21.
- If PCV15 is used: administer 1 dose PPSV23 1 year after the PCV15 dose (may use minimum interval of 8 weeks for adults with an immunocompromising condition,* cochlear implant, or cerebrospinal fluid leak).
- If PPSV23 is not available: 1 dose PCV20 or 1 dose PCV21 may be given 1 year later (only if 1 dose of PPSV23 is indicated).
- If PCV20 or PCV21 is used: a dose of PPSV23 isn’t indicated; pneumococcal vaccinations are complete.
- If PCV15 is used: administer 1 dose PPSV23 1 year after the PCV15 dose (may use minimum interval of 8 weeks for adults with an immunocompromising condition,* cochlear implant, or cerebrospinal fluid leak).
Shared clinical decision-making
Based on shared clinical decision-making, adults age 65 years or older who have previously received both PCV13 (received at any age) and PPSV23 (received at age 65 years or older) may receive 1 dose PCV20 or 1 dose PCV21 (or no additional pneumococcal vaccine).
Special situations
- Age 19–49 years with certain underlying medical conditions or other risk factors** who have:
- Not previously received a PCV13, PCV15, PCV20, or PCV21 or whose previous vaccination history is unknown: 1 dose PCV15 or 1 dose PCV20 or 1 dose PCV21. If PCV15 is used, administer 1 dose PPSV23 at least 1 year after the PCV15 dose (may use minimum interval of 8 weeks for adults with an immunocompromising condition,* cochlear implant, or cerebrospinal fluid leak).
- Previously received only PCV7: follow the recommendation above.
- Previously received only PCV13: 1 dose PCV20 or 1 dose PCV21 at least 1 year after the last PCV13 dose
- Previously received only PPSV23: 1 dose PCV15 or 1 dose PCV20 or 1 dose PCV21, at least 1 year after the last PPSV23 dose. If PCV15 is used, no additional PPSV23 doses are recommended.
- Previously received PCV13 and 1 dose of PPSV23: 1 dose PCV20 or 1 dose PCV21 at least 5 years after the last pneumococcal vaccine dose.
- Adults aged 19 years and older who have received PCV20 or PCV21: no additional pneumococcal vaccine dose recommended.
- Pregnancy: No recommendation for PCV or PPSV23 due to limited data.
- PPSV23 not available: Adults aged 19 years or older who received PCV15 but have not yet completed PPSV23 series, can complete the series with either 1 dose of PCV20 or 1 dose of PCV21 if they no longer have access to PPSV23.
*Note: Immunocompromising conditions include chronic renal failure, nephrotic syndrome, immunodeficiencies, iatrogenic immunosuppression, generalized malignancy, HIV infection, Hodgkin disease, leukemia, lymphoma, multiple myeloma, solid organ transplant, congenital or acquired asplenia or sickle cell disease or other hemoglobinopathies.
**Note: Underlying medical conditions or other risk factors include alcoholism, chronic heart/liver/lung disease, chronic renal failure, cigarette smoking, cochlear implant, congenital or acquired asplenia, CSF leak, diabetes mellitus, generalized malignancy, HIV infection, Hodgkin disease, immunodeficiencies, iatrogenic immunosuppression, leukemia, lymphoma, multiple myeloma, nephrotic syndrome, solid organ transplant, or sickle cell disease or other hemoglobinopathies.
Routine vaccination
Adults known or suspected to be unvaccinated or incompletely vaccinated: Administer remaining doses (1, 2, or 3 IPV doses) to complete a 3-dose primary series.* Unless there are specific reasons to believe they were not vaccinated, most adults who were born and raised in the United States can assume they were vaccinated against polio as children.
Special situations
Adults at increased risk of exposure to poliovirus who completed primary series*: may administer one lifetime IPV booster
*Note: Complete primary series consists of at least 3 doses of IPV or trivalent oral poliovirus vaccine (tOPV) in any combination. For detailed information, see: www.cdc.gov/vaccines/vpd/polio/hcp/recommendations.html
Routine vaccination
Pregnant persons of any age:
- Pregnant at 32 weeks 0 days through 36 weeks and 6 days gestation from September through January in most of the continental United States*: 1 dose Abrysvo. Administer RSV vaccine regardless of previous RSV infection.
- Either maternal RSV vaccination with Abrysvo or infant immunization with nirsevimab or clesrovimab (RSV monoclonal antibodies) are recommended to prevent severe respiratory syncytial virus disease in infants.
- All other pregnant persons: RSV vaccine not recommended
- Subsequent pregnancies: Additional doses not recommended. No data are available to inform whether additional doses are needed in subsequent pregnancies. If vaccine was not provided during the current pregnancy, the infant should receive nirsevimab or clesrovimab
*Note: Providers in jurisdictions with RSV seasonality that differs from most of the continental United States (e.g., Alaska, jurisdictions with tropical climate) should follow guidance from public health authorities on timing of administration. Refer to the 2026 Child and Adolescent Immunization Schedule for considerations regarding RSV monoclonal antibody administration to infants.
Age 75 years or older
- Unvaccinated: 1 dose (Arexvy or Abrysvo or mResvia). Additional doses not recommended.
- Previously vaccinated: additional doses not recommended. No data are available to inform whether additional doses are needed.
Special situations
Age 50–74 years:
- Unvaccinated and at increased risk of severe RSV disease**: 1 dose (Arexvy or Abrysvo or mResvia). Additional doses not recommended.
- Previously vaccinated: Additional doses not recommended. No data are available to inform whether additional doses are needed.
Persons 50 years and older can get RSV vaccine at any time but it is best to administer in late summer and early fall before RSV spreads in communities—ideally August through October in most of continental United States.
**Note: People can self-attest to the presence of a risk factor. The following medical and other conditions increase the risk of severe RSV disease:
- Chronic cardiovascular disease (e.g., heart failure, coronary artery disease, congenital heart disease). Excludes isolated hypertension.
- Chronic lung or respiratory disease (e.g., chronic obstructive pulmonary disease, emphysema, asthma, interstitial lung disease, cystic fibrosis).
- End-stage renal disease or dependence on hemodialysis or other renal replacement therapy
- Diabetes mellitus complicated by chronic kidney disease, neuropathy, retinopathy, or other end-organ damage
- Diabetes mellitus requiring treatment with insulin or sodium–glucose cotransporter 2 (SGLT2) inhibitor
- Neurologic or neuromuscular conditions causing impaired airway clearance or respiratory muscle weakness (e.g., post-stroke dysphagia, amyotrophic lateral sclerosis, muscular dystrophy). Excludes history of stroke without impaired airway clearance.
- Chronic liver disease e.g., cirrhosis
- Chronic hematologic conditions (e.g., sickle cell disease, thalassemia)
- Severe obesity (body mass index ≥ 40 kg/m2)
- Moderate or severe immune compromise
- Residence in a nursing home
- Other chronic medical conditions or risk factors that a health care provider determines would increase the risk of severe disease due to viral respiratory infection (e.g., frailty, concern for presence of undiagnosed chronic medical conditions, residence in a remote or rural community where escalation of medical care is challenging).
Routine vaccination
- Completed primary series and received at least 1 dose Tdap at age 10 years or older: Td or Tdap every 10 years thereafter
- Completed primary series and did NOT receive Tdap at age 10 years or older: 1 dose Tdap, then Td or Tdap every 10 years thereafter
- Unvaccinated or incomplete primary vaccination series for tetanus, diphtheria, or pertussis: Administer remaining doses (1, 2, or 3 doses) to complete 3-dose primary series. 1 dose Tdap followed by 1 dose Td or Tdap at least 4 weeks later, and a third dose of Td or Tdap 6–12 months later (Tdap is preferred as first dose and can be substituted for any Td dose), then Td or Tdap every 10 years thereafter.
Special situations
- Pregnancy: 1 dose Tdap during each pregnancy, preferably in early part of gestational weeks 27–36.
- Wound management: Persons with 3 or more doses of tetanus-toxoid-containing vaccine: For clean and minor wounds, administer Tdap or Td if more than 10 years since last dose of tetanus-toxoid-containing vaccine; for all other wounds, administer Tdap or Td if more than 5 years since last dose of tetanus-toxoid-containing vaccine. Tdap is preferred for persons who have not previously received Tdap or whose Tdap history is unknown. If a tetanus-toxoid-containing vaccine is indicated for a pregnant woman, use Tdap. For detailed information, see www.cdc.gov/mmwr/volumes/69/wr/mm6903a5.htm
Routine vaccination
- No evidence of immunity to varicella: 2-dose series 4–8 weeks apart if previously did not receive varicella-containing vaccine (VAR or MMRV [measles-mumps-rubella-varicella vaccine] for children); if previously received 1 dose varicella-containing vaccine, 1 dose at least 4 weeks after first dose.
- Evidence of immunity: U.S.-born before 1980 (except for pregnant persons and health care personnel [see below]), documentation of 2 doses varicella-containing vaccine at least 4 weeks apart, diagnosis or verification of history of varicella or herpes zoster by a health care provider, laboratory evidence of immunity or disease.
Special situations
- Pregnancy with no evidence of immunity to varicella: VAR contraindicated during pregnancy; after pregnancy (before discharge from health care facility), 1 dose if previously received 1 dose varicella-containing vaccine or dose 1 of 2-dose series (dose 2: 4–8 weeks later) if previously did not receive any varicella-containing vaccine, regardless of whether U.S.-born before 1980.
- Health care personnel with no evidence of immunity to varicella: 1 dose if previously received 1 dose varicella-containing vaccine; 2-dose series 4–8 weeks apart if previously did not receive any varicella-containing vaccine, regardless of whether U.S.-born before 1980.
- HIV infection with CD4 percentages ≥15% and CD4 count ≥200 cells/mm3 with no evidence of immunity: Vaccination may be considered (2 doses 3 months apart); VAR contraindicated for HIV infection with CD4 percentage <15% or CD4 count <200 cells/mm3.
- Severe immunocompromising conditions: VAR contraindicated.
Routine vaccination
Age 50 years or older*: 2-dose series recombinant zoster vaccine (RZV, Shingrix) 2–6 months apart (minimum interval: 4 weeks; repeat dose if administered too soon), regardless of previous herpes zoster or history of zoster vaccine live (ZVL, Zostavax) vaccination.
*Note: Serologic evidence of prior varicella is not necessary for zoster vaccination. However, if serologic evidence of varicella susceptibility becomes available, providers should follow ACIP guidelines for varicella vaccination first. RZV is not indicated for the prevention of varicella, and there are limited data on the use of RZV in persons without a history of varicella or varicella vaccination.
Special situations
- Pregnancy: There is currently no ACIP recommendation for RZV use in pregnancy. Consider delaying RZV until after pregnancy.
- Immunocompromising conditions (including persons with HIV regardless of CD4 count)**: 2-dose series recombinant zoster vaccine (RZV, Shingrix) 2–6 months apart (minimum interval: 4 weeks; repeat dose if administered too soon). For detailed information, see https://www.cdc.gov/shingles/hcp/vaccine-considerations/immunocompromised-adults.html
**Note: If there is no documented history of varicella, varicella vaccination, or herpes zoster, providers should refer to the clinical considerations for use of RZV in immunocompromised adults aged ≥19 years and the ACIP varicella vaccine recommendations for further guidance: www.cdc.gov/mmwr/volumes/71/wr/mm7103a2.htm
Appendix: Contraindications and precautions
When a contraindication is present, a vaccine should not be administered. Vaccination providers should check FDA-approved prescribing information for the most complete and updated information, including contraindications, warnings and precautions.
| Contraindicated or not recommended | Precautions |
| Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a component of an mRNA COVID-19 vaccine. See package inserts and FDA EUA fact sheets for a full list of vaccine ingredients. mRNA COVID-19 vaccines contain polyethylene glycol (PEG). |
|
| Contraindicated or not recommended | Precautions |
| Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a component of a Novavax COVID-19 vaccine. See package inserts and FDA EUA fact sheets for a full list of vaccine ingredients. |
|
| Contraindicated or not recommended | Precautions |
|
|
| Contraindicated or not recommended | Precautions |
|
Severe allergic reaction (e.g., anaphylaxis) to any ccIIV of any valency, or to any component of ccIIV3
|
|
| Contraindicated or not recommended | Precautions |
|
Severe allergic reaction (e.g., anaphylaxis) to any RIV of any valency, or to any component of RIV3 |
|
| Contraindicated or not recommended | Precautions |
|
|
| Contraindicated or not recommended | Precautions |
|
Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a vaccine component
|
Moderate or severe acute illness with or without fever |
| Contraindicated or not recommended | Precautions |
|
Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a vaccine component including neomycin |
Moderate or severe acute illness with or without fever |
| Contraindicated or not recommended | Precautions |
|
Moderate or severe acute illness with or without fever |
| Contraindicated or not recommended | Precautions |
|
Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a vaccine component including neomycin and yeast |
Moderate or severe acute illness with or without fever |
| Contraindicated or not recommended | Precautions |
|
Moderate or severe acute illness with or without fever |
| Contraindicated or not recommended | Precautions |
|
|
| Contraindicated or not recommended | Precautions |
|
Moderate or severe acute illness with or without fever |
| Contraindicated or not recommended | Precautions |
|
Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a vaccine component |
|
| Contraindicated or not recommended | Precautions |
|
Moderate or severe acute illness with or without fever |
| Contraindicated or not recommended | Precautions |
|
Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a vaccine component. |
Moderate or severe acute illness with or without fever |
| Contraindicated or not recommended | Precautions |
|
Moderate or severe acute illness with or without fever |
| Contraindicated or not recommended | Precautions |
|
Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a vaccine component |
Moderate or severe acute illness with or without fever |
| Contraindicated or not recommended | Precautions |
|
Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a vaccine component |
|
| Contraindicated or not recommended | Precautions |
|
Severe allergic reaction (e.g., anaphylaxis) to a vaccine component |
Moderate or severe acute illness with or without fever |
| Contraindicated or not recommended | Precautions |
|
|
| Contraindicated or not recommended | Precautions |
|
|
| Contraindicated or not recommended | Precautions |
|
|