
The new board recertification process has garnered mixed reviews from family physicians. Find out how it will impact you.
Fam Pract Manag. 2005;12(1):42-48

When Mitchell Lewis, MD, of Marathon, Fla., finished his third board recertification exam in July 2003, he thought the arduous part was behind him, at least for another seven years. But as he left the room, Lewis was handed an envelope, which contained his introduction to the new maintenance of certification requirements created by the American Board of Family Practice (ABFP).*
“After completing the last question on the exam, I felt the typical train-ran-me-over blues when a smiling proctor handed me a big envelope,” Lewis said. “I opened it on the elevator, on the way up to my overpriced hotel room, and found out that the ABFP hadn’t had enough fun with me yet.”
Lewis is among the first wave of family physicians who must comply with the new requirements, and he isn’t alone in responding with angst.
In October, following much testimony critical of the new process, the American Academy of Family Physicians (AAFP) Congress of Delegates voted to “urge” the ABFP to suspend components of the program until further testing and improvements could be completed. But in November, the ABFP announced it is moving forward.
“We listened very carefully at the Congress of Delegates, but we’ve decided not to suspend maintenance of certification,” said Thomas E. Norris, MD, president of the ABFP board of directors and professor of family medicine and vice dean at the University of Washington in Seattle. “We think communication is improving, and we think we have most of the technical problems fixed. If we were to suspend maintenance of certification, we would be sending the wrong message to the public.”
KEY POINTS
Family physicians must begin the ABFP’s new maintenance of certification program following their next recertification exam.
The new requirements include six Web-based “self-assessment modules” every seven years and completion of a quality improvement project.
While some family physicians believe the new requirements are onerous, some have found them educational.
The AAFP has expressed support for the concept of maintenance of certification, but it has expressed several concerns about the initial design and implementation of the ABFP program.
Why is the ABFP doing this?
The concept of maintenance of certification is in many ways nothing new to family physicians. Thirty-five years ago, the ABFP became the first specialty board to require recertification and continuing medical education of its diplomates. In contrast, the American Board of Internal Medicine did not begin requiring recertification until 1990.
The ABFP is one of 24 specialty boards belonging to the American Board of Medical Specialties (ABMS), which recently directed its boards to move from a process of recertification (e.g., through a cognitive exam administered every seven years) to maintenance of certification, which stresses lifelong learning and ongoing improvement. The move was made in response to public concerns about health care safety and quality, as well as concerns within the profession that medical decisions were not based consistently on current evidence.
While the ABFP could not ignore the ABMS directive to implement maintenance of certification, some believe it has gone further than was required, creating a process that is burdensome and of questionable value.
“I am not opposed to the concept of maintenance of certification,” said Richard Feldman, MD, immediate past president of the Indiana Academy of Family Physicians, and a vocal critic of the new process. “The problem is what the ABFP developed. It’s extraordinarily complex, and it has alienated good, responsible, mainstream family physicians.”
“I have heard from FPs across the country, and I am convinced that we are going to lose a significant number of diplomates because of MOC – maybe 25 to 30 percent,” he said. “If the Board doesn’t retool this, and do it quickly, my fear is that this will fragment our specialty. This situation is urgent.”
Already, positions seem polarized. Family physician Christopher Koman, MD, of Pittsburgh, recertified in 2003 and recently completed his first “self-assessment module,” one of the new requirements. To Koman, the program is “just another layer of nonsensical bureaucracy on an already taxed physician. Succinctly, it is onerous, not well-thoughtout, lacking rank and file input, and was half baked at the time it was forced upon me. I found problems with it and resented having to pay to be a beta tester.”
On the flip side are family physicians such as Robert Nielson, MD, of Saratoga Springs, N.Y. He too recertified in 2003 and has taken his first self-assessment module. “I actually enjoyed it,” he said. “I thought it was well written and very easy to complete. I even printed one of their hypertension help cards, laminated it and keep it in the office as a reference. I don’t have any complaints at all.”
The new requirements
All board-certified family physicians will begin the ABFP’s maintenance of certification program after their next recertification exam, with all groups reaching compliance by 2010. The initial group of more than 11,000 physicians who took the board exam in 2003 should have completed the first requirement (a self-assessment module) by Dec. 31, 2004. At press time, however, roughly 5,500 physicians had started the process and only half of them had actually completed the first module, according to the ABFP.
While the program is set up to charge late fees, the ABFP is considering a one-time forgiveness. “This is new, and a lot of people got confused when the Academy’s Congress asked that we suspend it,” said Norris. “We want to be fair and give people an opportunity to do this without punishing them.”
The new requirements are “just an evolutionary step from the old requirements,” he said.
Part one: Evidence of professional standing This requirement is essentially unchanged and involves possession of a full, unrestricted and active medical license. The American Board of Internal Medicine is experimenting with two alternatives – peer review and patient satisfaction surveys – which have been somewhat controversial. However, the ABFP is currently only studying these options and has no immediate plans to implement them, said Norris.
Part two: Life-long learning and self-assessment During each seven-year recertification cycle, family physicians will now need to complete six Internet-based, self-assessment modules to improve their knowledge of common medical problems. (See the example.) The first two modules address diabetes and hypertension, and new topics will be added each year. The ABFP will be developing specifications for the self-assessment modules so that other organizations, including the AAFP, can develop their own modules.
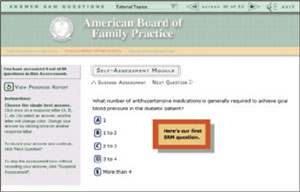
During their next recertification cycle, family physicians will be required to complete six Internet-based, self-assessment modules, such as the hypertension module shown here.
The 60-question modules come with 15 CME credits and are open-book tests. They can even be completed in groups, sometimes referred to as “SAM parties.” Physicians do not have to complete the modules at one sitting; modules can be paused and resumed. To pass, physicians must obtain a score of 80 percent or better on each section. “The pass rate is set at a level of mastery, and we anticipate that a high percentage of physicians will not achieve the desired level of competency the first time they answer the self-assessment module questions,” said Norris.
Physicians who don’t pass can review their missed answers, click on hyperlinks to read related articles from the literature and retake the test as many times as necessary. “The goal is not to get a high score or to get past the test,” said Norris. “The goal is to gain the knowledge, and the test is simply a tool to do this. After you have worked through this process and gotten to the level of mastery, you can move on.”
After each self-assessment module, physicians will need to complete an online patient simulation using what’s called a computer-based assessment system. (See the example.)
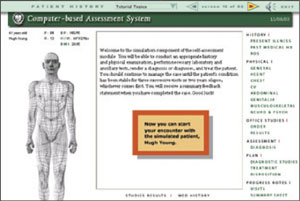
The ABFP’s simulated, computerized patient is intended to help physicians assess how well they manage patients with diabetes, hypertension and other common conditions.
“It’s designed to take the disease process that the physician has just achieved mastery level on and apply it to a simulated, computerized patient,” said Norris. “In real life, if you see a diabetic patient, do their laboratory studies and put them on medication, you have to wait a month or so to see how the medication worked and how the lab tests changed. The computer lets us compress time. It is just a tool to allow you to simulate the conditions that you might see in your practice, similar to what an airline pilot might use to simulate an emergency landing.”
Once the simulated patient has achieved a steady state, the system records the module as completed in the physician’s file.
The final requirement of part two is completion of 300 hours of approved continuing medical education, which is unchanged. Time spent in parts two and four will count toward the CME requirement.
Part three: Cognitive expertise This component requires successful completion of the closed-book recertification exam, as was required in the past. However, there are a few changes. First, as of 2005, the exam will be entirely computerized. To apply to take the exam, physicians must log on to the ABFP Web site (https://www.theabfm.org/cert/ite.aspx) and complete an online application.
In addition, the exam is now being offered on multiple dates in July and again in early December and at more sites than in the past. “For most people, there is now a site within two hours of their office, so they don’t have to stay overnight to take the examination,” said Norris.
The ABFP has also changed the content of the examination. Rather than defining the content in terms of other specialties, the ABFP is surveying family physicians and “changing the fundamental blueprint to be more reflective of our actual practices,” said Norris.
Part four: Evaluation and enhancement of practice performance This component will be introduced in 2005 and will replace the traditional clinical office records review. It will require physicians to select patient records and report their contents as in the past process. However, the new process will be Internet based and, instead of focusing on record keeping, will focus on improving quality of care. Physicians’ data will be compared against data collected from their peers to highlight areas of improvement.
Based on the chart review results, physicians will need to formulate a quality improvement project and reassess their performance at a later date to see whether their practice has improved in the targeted area. For example, a physician might decide to do a quality improvement project to improve the rate of annual foot checks for patients with diabetes. “The solution may be simply for the nurse to set out the monofilament tester at every visit with a diabetic patient so it’s sitting in front of the physician as a reminder,” said Norris. “In six months, they might go back and find that they’re now testing 60 percent of their patients instead of 40 percent. That’s the improvement in practice that we’re after.”
The AAFP has created a quality-improvement program called Measuring, Evaluating and Translating Research Into Care (METRIC), which will help family physicians comply with part four of the new requirements. The METRIC program is scheduled to launch a diabetes module this month and a coronary artery disease module in July. For more information, visit https://www.aafp.org/cme/cme-topic/performance-improvement.html.
Common criticisms
While all specialty boards must comply with the ABMS mandate for maintenance of certification, the programs they have created are not identical. For example, the American Board of Internal Medicine (ABIM) is requiring its diplomates to obtain 25 patient and 10 peer assessments, take a closed-book exam and complete five self-evaluation modules over a 10-year recertification cycle. The ABIM estimates that the entire process will take 75 to 100 hours every 10 years, whereas the ABFP’s self-assessment modules alone are estimated to take approximately 90 hours every seven years. The American Board of Obstetricians and Gynecologists is taking a much simpler approach, providing its diplomates with three options: 1) a cognitive exam every six years, 2) an oral exam every six years or 3) yearly reading assignments and tests. The American Board of Radiology is requiring two self-assessment modules per year, or 20 over the 10-year recertification cycle.
The ABFP believes its program is challenging but still in keeping with what other boards are requiring and what the ABMS mandated. “I’ve been privileged to have a seat at the table and see what other specialty boards are doing,” Norris said. “There are a lot of physicians in other specialties who feel just like our AAFP members, that their boards are going too fast and shouldn’t be doing this, but the reality is that most boards are moving in this direction.”
Among family physicians, criticism of the new process has centered almost unanimously on the self-assessment modules, which the Congress of Delegates tried unsuccessfully to have suspended. “The computer-based modules are extremely complex and problematic in a number of ways, including their educational value,” said Feldman. “They are esoteric, not relevant to practice and full of minutiae that you have to look up using Web links to various medical journals.”
While Feldman believes the self-assessment modules “may need to be scrapped,” he applauds part four of the new requirements, the part that focuses on quality improvement. “That’s where patient improvement is going to come,” he said, “not in answering 60 esoteric questions.”
In August, the Texas Academy of Family Physicians polled its members who had begun the new process. Of 119 respondents, 53 had started a self-assessment module. When asked, “Do you feel the questions were relevant to the practice of medicine?” 47 percent said yes – and 47 percent said no. (To view the survey results, go to http://www.tafp.org/survey/abfpsurveyresults.htm.)
Said Norris, “We’re hearing from physicians that the modules are a useful, educational exercise in an area where they take care of patients every day.”
The ABFP admits that the modules have had some technical problems, but over 20 major improvements have been made. “We have heard from our diplomates, AAFP’s members, about problems they’ve had,” said Norris. “It’s like any new piece of software. Even though we tested it quite thoroughly, we found a number of things that didn’t work quite right. But we have made a huge number of improvements, and it will continue to improve.”
Still, the computerized nature of the new process is a concern for some diplomates. “Everyone is going to need to get an e-mail account so that you can register for the examination and receive your results,” said Norris.
The ABFP originally designed the maintenance of certifications to be computerized for reasons of efficiency and convenience. Nielson, who recently invested in a new computer with a large, flat screen monitor and cable Internet access, liked the Web-based aspect of the self-assessment module because it allowed him a convenient way to earn CME. “You can do the module when you want and where you want. I did the hypertension module at home when my kids weren’t around or late at night when they were asleep,” he said. “It was very convenient.”
Physicians who have slow connections to the Internet have said the modules are difficult to access. “We’re working very hard to come up with functional alternatives for those folks,” Norris said. For example, users may now complete the self-assessment test and review the references on paper, and go online only to send in the results.
There has also been some debate as to how long the modules actually take to complete. Although the ABFP estimates that each module requires roughly 15 hours (assuming physicians are using a high-speed Internet connection), Feldman and others have called that “a woeful underestimate.” The Texas Academy’s survey found wide variation: Users said they spent between three hours and more than 31 hours completing the modules.
Critics have also questioned whether the new process is valid and whether it will actually improve patient care. “I’m afraid the tail is wagging the dog here,” said Koman. “I ask anyone to show me one study that demonstrates the maintenance of certification process will improve family physician competence, quality of care, morbidity, mortality rates, malpractice risk, patient satisfaction, et cetera. Pick one.”
Koman argues that the cost to the profession is too great. “Physicians at my hospital have expressed their desire to drop ABFP certification because of the additional cost, time and hassle associated with maintenance of certification,” he said. “What does this do to our profession? In my opinion, any time you disincentivize physicians from their work, that’s a bad thing.”
The Texas Academy’s survey asked whether respondents planned to continue pursuing maintenance of certification with the ABFP. Sixty-six percent of respondents said “yes,” 16 percent said “no” and 18 percent offered no response.
THE NEW REQUIREMENTS VS. THE OLD
The new maintenance of certification requirements for family physician are divided into four major components, which must be completed during each recertification cycle. The program will cost family physicians $1,150 to $1,500 every seven years.
| Old requirements | New requirements |
| Part 1: Evidence of Professional Standing | |
| Possession of a currently valid, full and unrestricted medical license. | Possession of a currently valid, full and unrestricted medical license. In the future, a process of peer review or patient satisfaction surveys may be added. |
| Part 2: Lifelong Learning and Self-Assessment | |
| Completion of six online self-assessment modules; 15 CME credits each. Completion of six online patient simulations using the Computer-Based Assessment System (CBAS). | |
| Completion of 300 hours of continuing medical education. | Completion of 300 hours of continuing medical education. (Parts 2 and 4 will count toward this requirement.) |
| Part 3 Cognitive Expertise | |
| Successful completion of the ABFP cognitive examination. | Successful completion of the ABFP cognitive examination; exam will be computerized beginning in 2005. |
| Part 4: Evaluation and Enhancement of Practice Performance | |
| Completion of the Office Record Review process (2 charts). | Completion of the Performance in Practice Module, which consists of a record review (10 charts), development of a quality improvement plan and review of results. This component will begin in 2005. |
The AAFP’s role
The ABFP and the AAFP are separate organizations with separate goals and accountabilities. While the AAFP was not involved in creating the maintenance of certification program, it does play a role in educating members about the new process and in developing programs to help family physicians comply with the new requirements.
“We also have a role in making sure that what happens to our members is fair and equitable and the right thing to do,” said Michael Fleming, MD, past president of the AAFP and chair of its board of directors.
Toward that end, the AAFP board of directors signed a Memorandum of Understanding with the ABFP in March 2004. It outlined, among other things, the AAFP’s support of the concept of maintenance of certification. This was perceived negatively by some family physicians. “To our membership and to the medical world, there was very much the perception of inaction and partnership with the ABFP,” said Feldman.
But in reality, Fleming said, “This issue had us greatly concerned, and we felt as though we needed to lay down some ground rules in order to discuss it productively. That’s why the memorandum of understanding came about.”
In October 2004, for the third year in a row, the AAFP Congress of Delegates took up the subject of maintenance of certification. It passed two resolutions asking its board of directors to take the following actions:
1. Urge the ABFP to suspend the maintenance of certification self-assessment modules until technical and clinical problems are adequately resolved, develop a better beta-testing mechanism to gather and disseminate evidence of the program’s effectiveness, and develop an alternative mechanism for those members who have unreliable access to the Internet.
2. Collaborate with the ABFP to educate members on the process and importance of maintenance of certification.
“It was a very strong message to our AAFP leadership and to the leadership of the ABFP that family physicians want some meaningful change in this process,” said Feldman.
The AAFP board of directors met in mid-November and drafted an official letter to the ABFP outlining the Congress’ concerns and offering five recommendations:
1. Make the self-assessment modules optional in 2004 and 2005 for the purpose of beta testing. “We felt that there needed to be ongoing content review, as some questions appear to be outside the practices of most family physicians and some appear to contain outdated recommendations,” said Fleming.
2. Require a self-assessment module every other year rather than every year. “We noted that this was the case with our colleagues who are certified by the American Board of Internal Medicine,” said Fleming.
3. Provide the option of a paper version of the self-assessment module for several years prior to making the transition to an Internet-only format. “Again, we noted that this was the case with our colleagues at the ABIM, who can take their self-assessment module at the American College of Physicians’ annual meeting, where it’s done on paper.”
4. Modify the self-assessment modules so that, when users review their wrong answers, they are provided with the reference from the literature and a summary of why their answer was wrong and why the correct answer is in fact correct. “We think that is a much better learning tool than just being told you’re wrong,” said Fleming.
5. Address the technical challenges experienced by family physicians prior to moving from beta testing to full implementation. “This includes providing better live support, particularly after-hours technical support,” said Fleming.
But before the AAFP had presented its recommendations, the ABFP sent a letter to all diplomates stating that, while it would continue improving the new program, it saw no reason to suspend it.
“We are disappointed that the ABFP did not wait to receive our letter before they spoke to their diplomates,” said Fleming. “We had hope that by sending our letter we could open conversations based on our recommendations, but their letter appears to close that door. Nevertheless, we will continue to initiate conversations.” AAFP leaders are scheduled to meet with the ABFP on Jan. 20.
Norris noted that the purpose of the ABFP’s letter was to update diplomates who were confused about whether the AAFP’s action had changed the requirements. He added that, while the ABFP is not willing to make the self-assessment modules optional, it has already addressed or is addressing many of the AAFP’s concerns. For example, it is instituting an annual content review, minimizing the use of computers and continuing to make technical improvements in the modules. Norris added, “The exact number of modules required in each recertification cycle is under review. At this time, we are requiring six, but this could change.”
Fleming, who recertified in 2003 and has completed his first self-assessment module, says he understands members’ frustrations. “The board of the AAFP is frustrated as well,” he said. “We are offering these suggestions in good faith based on what our Congress of Delegates passed, and we want there to continue to be good, open discussion between us and the ABFP. As the memorandum of understanding states, we do agree with the concept of lifelong learning and maintenance of certification, but we think that before this is rolled out for everyone, we need to have it right. It needs to be as good as it can be.”