
Am Fam Physician. 1999;59(3):575-582
See related patient information handout on herniated lumbar disc, written by the authors.
Degeneration of the intervertebral disc from a combination of factors can result in herniation, particularly at the L4-5 and L5-S1 levels. The presence of pain, radiculopathy and other symptoms depends on the site and degree of herniation. A detailed history and careful physical examination, supplemented if necessary by magnetic resonance imaging, can differentiate a herniated lumbar disc from low back strain and other possible causes of similar symptoms. Most patients recover within four weeks of symptom onset. Many treatment modalities have been suggested for lumbar disc herniation, but studies often provide conflicting results. Initial screening for serious pathology and monitoring for the development of significant complications (such as neurologic defects, cauda equina syndrome or refractory pain) are essential in the management of lumbar disc herniation.
The intervertebral disc is responsible for the attachment of vertebral bodies to each other, providing flexibility and absorbing and distributing the loads applied to the spinal column. With aging, the disc undergoes significant changes in volume and shape as well as in biochemical composition and biomechanical properties. Lumbar disc herniations are believed to result from anular degeneration that leads to a weakening of the anulus fibrosus, leaving the disc susceptible to anular fissuring and tearing.1
Symptoms of a herniated lumbar disc may often be difficult to distinguish from those of other spinal disorders or simple back strain. To effectively manage this disorder, it is crucial that a complete medical history and physical examination be performed. It is also important to understand the natural history of herniated disc and subsequent radiculopathy, the probability of spontaneous improvement and the contribution of diagnostic imaging studies or referral to an orthopedic specialist. This article discusses a standardized approach to the diagnosis and conservative treatment of a herniated lumbar disc. This approach will lead to more efficient use of diagnostic studies and a reduction in unnecessary referrals and ineffectual surgical procedures.
Etiology of Disc Degeneration
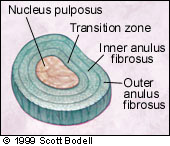
The intervertebral disc is arranged in four concentric layers: (1) an outer anulus fibrosus composed of dense collagen fibril lamellae; (2) a fibrocartilaginous inner anulus fibrosus; (3) a transition zone; and (4) the central nucleus pulposus2 (Figure 1). The frame work of the disc is composed of collagen fibers in the anulus, which provide tensile strength, and proteoglycans in the nucleus, which provide stiffness and resistance to compression.
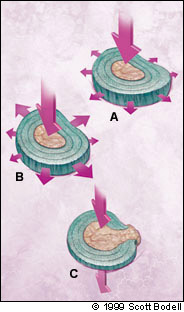
Several factors, including genetic factors and changes in hydration and collagen, are believed to play a role in the development of degenerative disc disease. It is widely accepted that the water-binding capability of the nucleus plays an integral role in the physical properties of the disc. In the healthy disc, the nucleus distributes the applied forces equally throughout the anulus. Decreased hydration of the disc can reduce the cushioning effect, thus transmitting a greater portion of the applied loads to the anulus in an asymmetric distribution,3 which could lead to injury, as illustrated in Figure 2. Increases in the collagen content of the nucleus and in its crystallinity have been reported to be partially responsible for disc degeneration.4
The possibility of genetic effects has been investigated in other spinal disorders, such as scoliosis, spondylolisthesis and ankylosing spondylitis, but few studies have searched for genetic factors in degenerative disc disease. One study5 reported a strong familial predisposition to discogenic low back pain and suggested that the etiology of degenerative disc disease includes both genetic and environmental factors.
Clinical Assessment
MEDICAL HISTORY
Information from the medical history allows the physician to target the physical examination, leading to an accurate diagnosis. The symptoms related to spinal disorders must be differentiated from those of other potentially serious conditions, including metastatic and rheumatologic disorders, fracture and infection. The Agency for Health Care Policy and Research (AHCPR)6 has developed guidelines for the management of acute (less than three months' duration) low back pain. The AHCPR recommendations are based on “red flags” for spinal fracture, cancer or infection (Table 1).
| Possible condition | Findings from the medical history |
|---|---|
| Fracture | Major trauma (motor vehicle accident, fall from height) |
| Minor trauma or strenuous lifting in an older or osteoporotic patient | |
| Tumor or infection | Age > 50 years or < 20 years |
| History of cancer | |
| Constitutional symptoms (fever, chills, unexplained weight loss) | |
| Recent bacterial infection | |
| Intravenous drug use | |
| Immunosuppression (corticosteroid use, transplant recipient, HIV infection) | |
| Pain worse at night or in the supine position | |
| Cauda equina syndrome | Saddle anesthesia |
| Recent onset of bladder dysfunction | |
| Severe or progressive neurologic deficit in lower extremity |
Rheumatologic disorders often begin in the appendicular skeleton before progressing to the spine. Inflammatory arthritides such as ankylosing spondylitis result in generalized pain and stiffness that are worse in the morning and relieved somewhat throughout the day. In general, if a disc herniation is responsible for the back pain, the patient can recall the distinct time of onset and contributing factors, whereas if the pain is of a gradual onset, other degenerative diseases are more probable than disc herniation.
The most common levels for a herniated disc are L4-5 and L5-S1. The onset of symptoms is characterized by a sharp, burning, stabbing pain radiating down the posterior or lateral aspect of the leg, to below the knee. Pain is generally superficial and localized, and is often associated with numbness or tingling. In more advanced cases, motor deficit, diminished reflexes or weakness may occur. Generally, only the relatively uncommon central disc herniation provokes low back pain and saddle pain in the S1 and S2 distributions. A central herniated disc may also compress nerve roots of the cauda equina, resulting in difficult urination, incontinence or impotence. The medical history and physical examination may disclose bowel or bladder dysfunction. In such cases, immediate referral to a specialist is required for emergency surgery to prevent permanent loss of function.
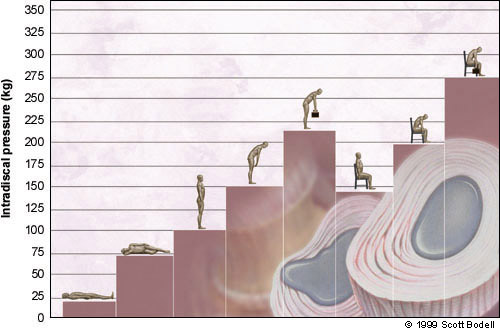
Often the most difficult aspect of evaluating patients with symptoms of a central herniated disc is differentiation between low back strain and herniated disc. Pain caused by low back strain is exacerbated during standing and twisting motions, whereas pain caused by central disc herniation is worse in positions (such as sitting) that produce increased pressure on the anular fibers. Questions about whether the patient's pain became worse while driving to the appointment and sitting in the waiting room may be revealing. The pressure on the intervertebral disc is increased during sitting and bending postures, as opposed to standing or recumbent positions7 (Figure 3). This explains the exacerbation of herniated disc symptoms when the patient is in the sitting position.
PHYSICAL AND NEUROLOGIC EXAMINATION OF THE LUMBAR SPINE
A complete physical and neurologic examination can reveal defects at specific levels. The first assessment in the physical examination is a search for any external manifestations of pain, including an abnormal stance. The patient's posture and gait should be examined for sciatic list, which is indicative of disc herniation. The spinous processes and interspinous ligaments should be palpated for tenderness. Range of motion should be evaluated. Pain during lumbar flexion suggests discogenic pain, while pain on lumbar extension suggests facet disease. Ligamentous or muscular strain can cause pain when the patient bends contralaterally.
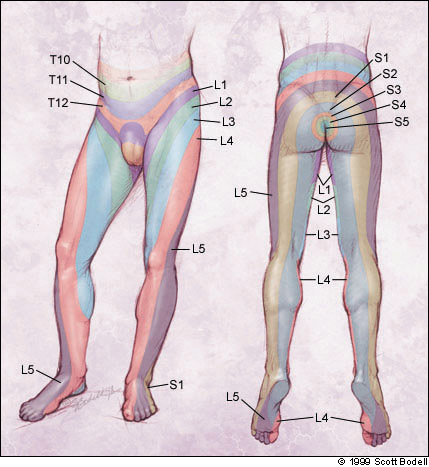
Motor, sensory and reflex function should be assessed to determine the affected nerve root level8 (Figure 4). Muscle strength is graded from zero (no evidence of contractility) to 5 (complete range of motion against gravity, with full resistance). Examination of the lumbar spine by neurologic levels is helpful in locating the source of the patient's symptoms (Table 2).
| Disc level | Location of pain | Motor deficit |
|---|---|---|
| T12-L1 | Pain in inguinal region and medial thigh | None |
| L1-2 | Pain in anterior and medial aspect of upper thigh | Slight weakness in quadriceps; slightly diminished suprapatellar reflex |
| L2-3 | Pain in anterolateral thigh | Weakened quadriceps; diminished patellar or suprapatellar reflex |
| L3-4 | Pain in posterolateral thigh and anterior tibial area | Weakened quadriceps; diminished patellar reflex |
| L4-5 | Pain in dorsum of foot | Extensor weakness of big toe and foot |
| L5-S1 | Pain in lateral aspect of foot | Diminished or absent Achilles reflex |
Specific movements and positions that reproduce the symptoms should be investigated during the examination to help determine the source of the pain. For example, the upper lumbar region (L1, L2 and L3) controls the iliopsoas muscles, which can be evaluated by testing resistance to hip flexion. While seated, the patient should attempt to raise each thigh while the physician's hands are placed on the leg to create resistance. Pain and weakness are indicative of upper lumbar nerve root involvement. The L2, L3 and L4 nerve roots control the quadriceps muscle, which can be evaluated by manually trying to flex the actively extended knee. The L4 nerve root also controls the tibialis anterior muscle, which can be tested by heel walking.
The L5 nerve root controls the extensor hallucis longus, which can be tested with the patient seated and moving both great toes in a dorsiflexed position against resistance. The L5 nerve root also innervates the hip abductors, which are evaluated by use of the Trendelenburg test. This test requires the patient to stand on one leg; the physician stands behind the patient and puts his or her hands on the patient's hips. A positive test is characterized by any drop in the pelvis on the opposite side and suggests either L5 nerve root or hip-joint pathology. Possible cauda equina syndrome can be identified by unexpected laxity of the anal sphincter, perianal or perineal sensory loss, or major motor loss in the lower extremities.
Nerve root tension signs are often used in the evaluation of patients suspected of having a herniated disc. The straight-leg raising test is performed with the patient in the supine position. The physician raises the patient's legs to approximately 90 degrees. Normally, this position results in only minor tightness in the hamstrings. If nerve root compression is present, this test causes severe pain in the back of the affected leg and can reveal a disorder of the L5 or S1 nerve root.
A crossed straight-leg raising test may also suggest nerve root compression. In this test, straight-leg raising of the contralateral limb reproduces more specific but less intense pain on the affected side. In addition, the femoral stretch test can be used to evaluate the reproducibility of pain. In this test, the patient lies in either the prone or the lateral decubitus position. The thigh is extended at the hip, and the knee is flexed. Reproduction of pain suggests upper nerve root (L2, L3 and L4) disorders.
Attention should also be paid to any non-organic physical signs (Waddell signs), which may identify patients with pain of a psychologic or socioeconomic basis.9 These signs include superficial tenderness, positive results on simulation tests (i.e., maneuvers that appear to the patient to be a test but actually are not), distraction tests that attempt to reproduce positive physical findings when the patient is distracted, regional disturbances that do not correspond to a neuroanatomic or dermatomal distribution and overreaction during the examination. Patients who are more likely to demonstrate such nonorganic signs include patients with work-related injury or those involved in litigation related to their injury.
Imaging of the Herniated Disc
The major finding on plain radiographs of patients with a herniated disc is decreased disc height. Radiographs have limited diagnostic value for herniated disc because degenerative changes are age-related and are equally present in asymptomatic and symptomatic persons.10 Neurodiagnostic imaging modalities reveal abnormalities in at least one third of asymptomatic patients.11 For this reason, computed tomography (CT) also has limited diagnostic value for herniated disc.
The gold standard modality for visualizing the herniated disc is magnetic resonance imaging (MRI), which has been reported to be as accurate as CT myelography in the diagnosis of thoracic and lumbar disc herniation.12 T1-weighted sagittal spin-echo images can confirm disc herniation; however, the size of herniation is underestimated because the low signal of the anulus merges with the low signal of the cerebrospinal fluid. Conventional T2 and T2-weighted fast spin-echo images are used in the diagnosis of degenerative disc disease. MRI also has the ability to demonstrate damage to the intervertebral disc, including anular tears and edema in the adjacent end plates. As with CT scans, MRI can reveal bulging and degenerative discs in asymptomatic persons; therefore, any management decisions should be based on the clinical findings corroborated by diagnostic test results.11
MRI has been traditionally used to obtain images in the axial and sagittal planes. Recent advances have brought about oblique images, which provide better views of certain anatomic structures that were not available with conventional methods.13,14 Oblique images are oriented perpendicular to the course of the neural foramen. It has been suggested that oblique MRI be added to the conventional technique to aid in the detection of foraminal impingement.
Nonoperative Treatment
While low back pain and radiculopathy are common causes of disability, the majority of patients experience resolution of their symptoms regardless of the treatment method. In one study15 of 208 patients with radicular pain of either an L5 or an S1 origin, 70 percent had marked reduction in leg pain within four weeks of the onset of symptoms. It is beneficial to provide symptomatic treatment to patients with symptoms of herniated disc during the first six weeks of symptoms.
As a result, the family physician often takes on the role of educator, providing advice on methods of relieving the symptoms of herniated disc. Most patients with low back pain respond well to conservative therapy, including limited bed rest, exercise and, in selected cases, injections. It is the responsibility of the physician to determine the goals and optimal strategy for each patient. The condition should be thoroughly explained to the patient, including the likely natural history and the potential forms of treatment.
The rationale for bed rest relates to the reduction in both mechanical pain and intradiscal pressure in the supine position. The optimal duration of bed rest for patients with herniated discs is debatable, but bed rest is commonly recommended for two to seven days. However, studies suggest that bed rest in excess of two days is not associated with a better outcome16 and that continuing to perform usual activities as tolerated leads to more rapid recovery than bed rest.17 Excessive bed rest can result in deconditioning, bone mineral loss and economic loss.
The benefit of aerobic exercise for relieving radicular pain is controversial. Advocates believe that strengthening of the abdominal and back muscles can relieve symptoms, reduce weight and alleviate depression and anxiety. Exercise and massage techniques are easily taught to the patient and family members. Extension and isometric exercises are performed first and, after sufficient strength and pain relief are achieved, flexion exercises are allowed. Flexion exercises are delayed because flexion motions apply the greatest load to the intervertebral disc.
The McKenzie exercise program is believed to be one of the most beneficial. This program is individualized to the patient's symptoms and emphasizes exercises that minimize or centralize radiating pain.18 However, several studies have reported no significant benefits of exercise programs in terms of functional recovery, range of motion or pain severity.19,20 Exercise programs must be carefully designed to provide the greatest benefit, especially for patients with other conditions that limit strenuous activity. Determining the patient's limitations and the goal for therapy is important.
Some physicians believe trigger point injections can provide extended relief for localized pain sources. An injection of 1 to 2 mL of 1 percent lidocaine (Xylocaine) without epinephrine is usually administered. The use of either ultrasound (phonophoresis) or electricity (iontophoresis) over the injected area may provide additional relief, although the benefits of these methods have not been proved. Epidural steroid injection therapy has been reported to be effective in patients with lumbar disc herniation with radiculopathy.21,22 Others have reported limited value from steroid injections in patients with radiculopathy.23,24
Surgical Indications for Herniated Disc
While most patients with a herniated disc may be effectively treated conservatively, some do not respond to conservative treatment or have symptoms that necessitate referral to a specialist. Any surgical decisions should be firmly based on the clinical symptoms and corroborating results of diagnostic testing. Indications for referral include the following: (1) cauda equina syndrome, (2) progressive neurologic deficit, (3) profound neurologic deficit and (4) severe and disabling pain refractory to four to six weeks of conservative treatment.