Pigmented villonodular synovitis is an uncommon disease that remains a diagnostic challenge. Presenting complaints commonly involve one joint, most often the knee or hip. Symptoms of pain and swelling characteristically have an insidious onset and are slowly progressive. The physical examination may be completely normal. Radiographs of the knee may appear normal or may show a periarticular soft tissue density, expansion of the suprapatellar pouch and local osseous changes confined to the patellofemoral articulation. Radiographs of the hip may show erosions in the head and neck of the femur and acetabulum. Magnetic resonance imaging usually demonstrates key diagnostic features, which include joint effusion, elevation of the joint capsule, hyperplastic synovium and low signal intensity resulting from hemosiderin deposition. The diagnosis of pigmented villonodular synovitis is confirmed by biopsy, and the treatment of choice is synovectomy.
Pigmented villonodular synovitis is an uncommon disease characterized by hyperplastic synovium, large effusions and bone erosions. The disease was first described as a distinct entity in 1941.1 Since then, many articles in the orthopedic, radiologic and rheumatologic literature have discussed the radiologic features of this disease. However, few articles have described its clinical presentation.
Pigmented villonodular synovitis remains a diagnostic challenge. On average, the disease is not correctly identified until 4.4 years after presentation.2 The difficulty stems from the insidious onset and nonspecific presentation of the disease, as well as its subtle radiographic findings. In addition, the disease can be difficult to differentiate from conditions such as rheumatoid arthritis, osteoarthritis and other inflammatory and neoplastic processes of the synovial lining.3
The family physician plays a crucial role in the early diagnosis and treatment of pigmented villonodular synovitis. Because patients often present initially with vague complaints, early diagnosis requires knowledge of the common symptoms and radiographic features of the disease.
Definition and Etiology
In the original description of the disease, the term “pigmented villonodular synovitis” was applied to a lesion that occurred in the synovial membrane of joints and tendon sheaths and was characterized by fibrous stroma, hemosiderin deposition, histiocytic infiltrate and giant cells.1 Subsequently, two forms of the disease were identified: a localized subtype characterized by a pedunculated lesion and a subtype with diffuse joint involvement.4
The etiology of pigmented villonodular synovitis remains controversial.4–8 The most widely held theory is that the disease is an inflammatory reaction of the synovium.1,4 However, some evidence exists that it is a benign neoplastic process.7
Epidemiology
The incidence of pigmented villonodular synovitis is 1.8 cases per 1 million people per year, with no environmental, genetic, ethnic or occupational predilection.9 Most studies show equal prevalence in males and females, although some investigations report a slightly greater predilection in males.9 Pigmented villonodular synovitis generally occurs in patients between the ages of 20 and 45 years, but it has been found in patients as young as 11 years and as old as 70 years.10
The vast majority of patients with pigmented villonodular synovitis have monoarticular complaints of pain and swelling. Only a few reports of polyarticular involvement have been published. In both the localized and diffuse subtypes, the knee is the most commonly affected joint (about 80 percent of patients),5 followed by the hip, ankle, small joints of the hands and feet, shoulder and elbow.10 The presentations of the disease in the knee and hip are somewhat different.
Pathology
Grossly, pigmented villonodular synovitis appears as a proliferative synovial process with brownish villonodular fronds in the affected joints (Figures 1 and 2). Histologically, diffuse disease is characterized by a mononuclear stromal cell infiltrate in the synovial membrane (Figure 3). Hemosiderin-laden macrophages give the characteristic brown color (Figure 4). Additional cell populations include foam cells and multinucleated giant cells.
FIGURE 1.
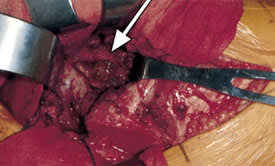
Intraoperative photograph showing characteristic hypertrophic synovium (arrow) and villonodular fronds in pigmented villonodular synovitis.
FIGURE 2.
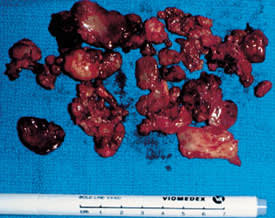
Gross specimen after total synovectomy.
FIGURE 3.
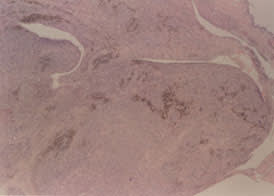
Low-power photomicrograph showing a villous formation with mononuclear stromal cells and populations of hemosiderin-laden macrophages.
FIGURE 4.
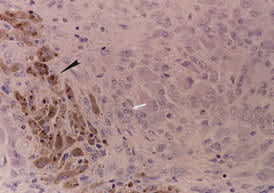
High-power photomicrograph demonstrating mononuclear stromal cell infiltrate (white arrow) and hemosiderin-laden macrophages (black arrow).
Pigmented Villonodular Synovitis of the Knee
Diffuse pigmented villonodular synovitis of the knee can mimic many other conditions. In one study of 25 patients,6 the two most common incorrect working diagnoses were extensor mechanism malalignment (patellofemoral syndrome) and meniscal lesion. The disease was also confused with inflammatory arthritis, ligament instability and other conditions.
Patients with diffuse pigmented villonodular synovitis of the knee complain of the insidious onset and slow progression of symptoms. One third of these patients report previous trauma to the knee.2 Patients also tend to complain of intermittent swelling and stiffness around the joint. Most report diffuse discomfort rather than severe focal pain (such as occurs with a meniscal tear or fracture).6 Hence, the diagnosis of diffuse pigmented villonodular synovitis may be suggested by a clinical history of swelling that has an insidious onset, is not preceded by trauma and is out of proportion to the degree of discomfort.6 Patients do not complain of knee instability; however, they occasionally report a “popping” sensation in the joint.
On physical examination, up to 96 percent of patients have distention of the suprapatellar pouch and a large effusion.6 As many as 40 percent of patients have a diffuse palpable synovial mass.6 Patients also have a slightly decreased ability to flex and extend the joint. Up to 90 percent of patients complain of mild to moderate tenderness, mainly over the medial patellofemoral area.6 In addition, arthrocentesis yields blood-tinged synovial fluid in 44 to 69 percent of patients.6,9
IMAGING STUDIES
In patients with pigmented villonodular synovitis of the knee, plain radiographs often appear normal. However, radiographic findings in diffuse disease can include a periarticular soft tissue density (in up to 80 percent of patients), expansion of the suprapatellar pouch and local osseous changes mainly confined to the patellofemoral articulation11 (Figure 5). The changes at the patellofemoral joint result from abnormal patellar tracking because of the synovial mass lifting and stretching the extensor mechanism, thereby allowing shear forces to act on the articular cartilage. Osteopenia is occasionally found, and degenerative changes may be detected in 30 to 40 percent of patients.11 In general, bone and joint changes are less common in the knee than in the hip, because of the ability of the knee capsule to expand to accommodate the hyperplastic synovium.
FIGURE 5.

Lateral radiograph of the knee showing a large cystic erosion in the inferior pole of the patella (arrows).
In patients with diffuse pigmented villonodular synovitis of the knee, magnetic resonance imaging (MRI) may show a large effusion, low signal intensity on both T1- and T2-weighted images (because of hemosiderin deposition), hyperplastic synovium and occasional bony erosions2,3,12 (Figures 6, 7 and 8).
FIGURE 6.

Axial T2-weighted magnetic resonance image (MRI) of the knee in a patient with pigmented villonodular synovitis. The scan shows a large effusion and villous proliferation arising from the synovial lining (arrow).
FIGURE 7.

Axial T2-weighted MRI scan showing a lesion in the proximal fibula (arrow) that has a low intensity consistent with pigmented villonodular synovitis.
FIGURE 8.

Sagittal T2-weighted MRI scan demonstrating a cystic lesion in the proximal fibula (arrowhead), as well as proliferative synovitis (arrow).
Pigmented Villonodular Synovitis of the Hip
The hip is the second most common location for pigmented villonodular synovitis. Like patients with knee disease, those with hip disease usually present with deep monoarticular pain of variable duration (a few months to a few years). The pain is often alleviated only by rest. Patients may localize the pain to the anterior groin or the lateral aspect of the hip. The pain is frequently intermittent, with completely asymptomatic periods in which patients are able to participate in all activities.
Patients occasionally report episodes of extreme pain, which may represent hemorrhage into the joint space. During these exacerbations, patients may be able to relieve the pain by positioning their hip in a flexed and externally rotated position. This positional relief of pain is typical of a joint effusion or inflammatory process of the synovium, in that the repositioning minimizes pressure within the joint.
Patients may also report decreased active and passive range of motion. A small number of patients (6.9 percent) can recall a specific traumatic event associated with the onset of symptoms,2 although this association may be coincidental.
IMAGING STUDIES
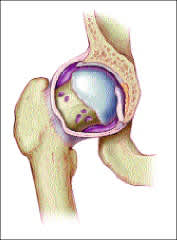
In pigmented villonodular synovitis of the hip, radiographs show bony erosions in the head and neck of the femur and acetabulum in 95 percent of patients.5 These erosions are found early in the course of hip disease and appear as cystlike structures on anteroposterior radiographs (Figure 9). An average of three to four erosions, ranging from a few millimeters to 5 cm in diameter, are typically seen5 (Figure 10). A thin sclerotic rim may also be present and is due to the slow growth of the process.
FIGURE 9.

Anteroposterior radiograph of the pelvis showing a cystic erosion in the right inferior medial femoral neck (black arrow), medial femoral head (arrowhead) and acetabulum (white arrow).
FIGURE 10.
Cystic erosions in the neck of the right femur.
Erosions are much more common in pigmented villonodular synovitis of the hip than the knee, primarily because the tight capsule of the hip joint does not allow the joint to expand to accommodate the hyperplastic synovium. As a result, intracapsular pressure increases, and bone erosion occurs. In the late stages of the disease, the articular joint space decreases, most often superolaterally, in 70 to 75 percent of patients.5
MRI is highly sensitive and specific for the diagnosis of pigmented villonodular synovitis of the hip. Characteristic MRI findings include hip joint effusion, lifting of the joint capsule, low signal intensity on both T1- and T2-weighted images (because of hemosiderin deposition), hyperplastic synovium (that appears as a lobulated synovial mass), bony erosions and preservation of bone density.10,11
On computed tomographic scans, the cystic erosions appear as a decreased signal of the marrow of the femoral head (Figure 11).
FIGURE 11.

Computed tomographic scan of the hip showing multiple erosions in the femoral neck (arrows).
Evaluation
Pigmented villonodular synovitis should be considered in the differential diagnosis of patients from 20 to 45 years of age who have monoarticular symptoms (Table 1). Most patients with this disease have a long history of pain and disability. The presence of non-traumatic effusions of the hip or knee should further raise the index of suspicion.
TABLE 1 Differential Diagnosis of Nontraumatic Monoarticular Hip or Knee Problems*
| Osteoarthritis |
| Inflammatory arthritis |
| Rheumatoid arthritis |
| Psoriatic arthritis |
| Systemic lupus erythematosus |
| Septic arthritis |
| Synovial chondromatosis |
| Pigmented villonodular synovitis |
| Benign or malignant bone tumor |
| Avascular necrosis (hip only) |
*—In patients 20 to 45 years of age.
Plain radiographs are the first studies that should be performed. In many patients, radiographs will be normal or show only subtle findings. Patients with nontraumatic knee effusions should then undergo arthrocentesis. The finding of blood-tinged fluid is highly suggestive, although not pathognomonic, of pigmented villonodular synovitis. MRI should be performed to further suggest the diagnosis and define the extent of the disease process.
In patients with hip lesions, an effusion usually cannot be identified by palpation. Thus, MRI is usually performed to search for hip effusion and hypertrophic synovium before arthrocentesis is considered or attempted.
Technetium-99m etidronate bone scanning may show diffuse mild uptake when bone erosions are present. However, the study may reveal no findings when the disease is confined to the synovium. Thus, a normal bone scan does not exclude the diagnosis of pigmented villonodular synovitis.
Treatment
The diagnosis of pigmented villonodular synovitis is confirmed by biopsy of the synovium. The treatment of choice is synovectomy. Associated bony lesions should be carefully curettaged, and bone grafting should be performed as necessary.
Diffuse pigmented villonodular synovitis has a high rate of local recurrence (up to 45 percent in one review4). The role of radiation therapy in the management of refractory disease is not clear. In one retrospective series,13 13 of 14 patients with recurrent or extensive diffuse disease treated with radiation therapy were disease-free at a mean follow-up period of 69 months. Eleven patients were characterized as having good or excellent limb function, and three patients had fair function. Radiotherapy can be considered in patients with previous adequate resection of disease who experience local relapse and in patients with a large amount of disease in whom complete resection is not possible.13
Synovectomy may not relieve all symptoms in patients with significant destructive changes in the joint. In these situations, arthrodesis or total joint replacement should be considered. A series of 11 patients with active diffuse pigmented villonodular synovitis of the knee treated with synovectomy and total knee arthroplasty showed a local control rate of approximately 70 percent and good to excellent joint function at a mean follow-up period of 10.8 years.14
