A “burner” is a common nerve injury resulting from trauma to the neck and shoulder, usually during sports participation. The injury is most often caused by traction or compression of the upper trunk of the brachial plexus or the fifth or sixth cervical nerve roots. Burners are typically transient, but they can cause prolonged weakness resulting in time loss from athletic participation. Furthermore, they often recur. Treatment consists of restoring range of motion, improving strength and providing protective equipment. Return to sports participation depends primarily on reestablishment of pain-free motion and full recovery of strength and functional status.
A “burner,” also called a “stinger,” is a nerve injury resulting from trauma to the neck and shoulder. Its primary symptom is burning pain radiating down one upper extremity. The pain is sometimes accompanied by numbness, paresthesias or weakness. Burners occur most commonly in football players, but they have also been reported in wrestlers, gymnasts and hockey players.1
A burner signifies peripheral nerve dysfunction or injury. In most cases, it is a brachial plexopathy involving the upper trunk. However, cervical nerve root lesions have also been described.2–6 A burner is generally a brief, self-limited injury, but recovery can take weeks to months in severe cases. The injury often becomes a recurrent problem and occasionally leads to a chronic syndrome.7
Although burners are common injuries, their true incidence is unknown. This void is largely due to underreporting by athletes. A survey of college football players found that 65 percent of players had at least one burner in their college careers, but 70 percent of these athletes did not report the injury to anyone.1
Pathophysiology
Burners are typically either grade 1 or 2 peripheral nerve injuries. A grade 1 injury is neurapraxia, which is a disruption of nerve function involving demyelinization.8,9 Axonal integrity is preserved, and remyelinization occurs within three weeks. A grade 2 injury is axonotmesis, which entails actual axonal damage and Wallerian degeneration.9 A grade 3 injury is neurotmesis, which is permanent nerve damage. Fortunately, grade 3 injuries are rare in sports and are not characteristic of burners.8,9
Three mechanisms of burners have been described. The first is traction injury to the brachial plexus (Figure 1, part A). Traction injury occurs when the shoulder is depressed and the neck is forced into lateral flexion away from the involved side; as a result, the brachial plexus is stretched.1,2,10 The second mechanism involves a direct blow to the supraclavicular fossa; this causes a percussive injury to the upper trunk5,6 (Figure 1, part B). The third mechanism is nerve compression by a combination of neck hyperextension and ipsilateral lateral flexion10 (Figure 1, part C). One investigator observed that the most persistent and severe symptoms from burners occurred with neck hyperextension and ipsilateral rotation.11
FIGURE 1.
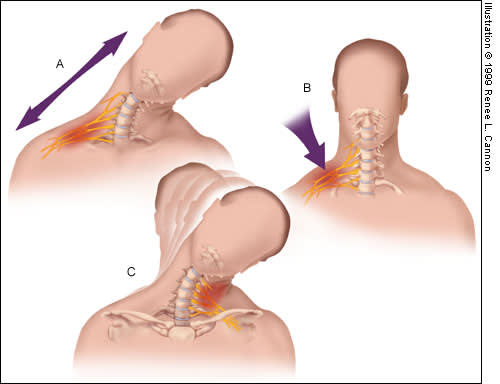
Mechanisms of “burners.” (A) Traction to the brachial plexus from ipsilateral shoulder depression and contralateral lateral neck flexion. (B) Direct blow to the supraclavicular fossa at Erb's point. (C) Compression of the cervical roots or brachial plexus from ipsilateral lateral flexion and hyperextension.
The role of abnormalities of the cervical neuroforamina, canal and discs is controversial. Studies indicate that cervical stenosis and disc abnormalities are frequently found in asymptomatic patients and in patients with compressive burners.7,12–14 However, the definition of cervical stenosis used in those studies has recently been questioned.15,16 A causative role for these abnormalities awaits further study.
History and Physical Examination
Burners occur most commonly with tackling in football. Thus, they are most often incurred by linebackers and defensive backs. Immediately after contact, the injured player classically feels burning pain in the supraclavicular area. The pain radiates down the arm, generally in a circumferential, nondermatomal pattern. The player might also note numbness, paresthesias or weakness in the extremity. Frequently, the discomfort resolves spontaneously in one to two minutes.2
A detailed description of immediate and residual symptoms should be obtained from the athlete suspected of having a burner. Information about pain quality, intensity, location, radiation and duration is helpful. The player should also be asked about numbness, paresthesias and weakness. The athlete and observers can describe the exact mechanism of injury. Because burners frequently recur, information on previous burners and their treatment is also meaningful.
The physical examination begins with inspection. On the field, the patient may shake the upper extremity or hold it against the body to reduce discomfort.2 Atrophy or asymmetry in the neck, shoulder or upper extremity suggests a previous injury or a predisposition to injury. Shoulder depression and atrophy of the deltoid and supraspinatus muscles commonly develop after burners.6
Palpation localizes tenderness and spasm, which are not specific for burners. Provided cervical stability has been established, range of motion in the neck and the shoulder should be evaluated. Sensation and muscle stretch reflexes should also be assessed. Spurling's test (Figure 2) and percussion of the supraclavicular fossa for tenderness or Tinel's sign may be positive.
FIGURE 2.
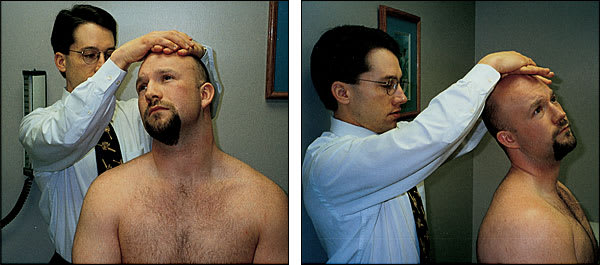
Spurling's test: anterior view (left) and lateral view (right). The examiner passively hyperextends and laterally flexes the patient's neck toward the involved side. The test is positive if axial loading by the examiner's hands reproduces symptoms.
Strength assessment warrants special comment. Muscles and their innervation are listed in Table 1. In burners, motor deficits usually involve muscles innervated by the fifth or sixth cervical nerve roots, the fibers of which travel through the upper trunk of the brachial plexus.8,10 Each of the areas listed in Table 1 should be tested manually.17–19
TABLE 1 Evaluation of Motor Function in Burners and Other Brachial Plexus Injuries
| Muscle | Innervation | Clinical test |
|---|---|---|
| Deltoid | Axillary (C5, C6) | Shoulder abduction |
| Supraspinatus | Suprascapular (C5, C6) | “Full can” abduction* |
| Infraspinatus | Suprascapular (C5, C6) | External rotation |
| Biceps brachii | Musculocutaneous (C5, C6) | Elbow flexion |
| Pronator teres | Median (C6, C7) | Forearm pronation |
| Triceps brachii | Radial (C7, C8) | Elbow extension |
| Abductor digiti minimi | Ulnar (C8, T1) | Fifth digit abduction |
*—“Full can” shoulder abduction is performed with the shoulder abducted 90 degrees, the arm in the plane of the scapula and the thumb directed upward, as if the patient could hold a full can of liquid without spilling. The examiner then resists abduction from this position.18,19
Although weakness may resolve within a few minutes of the injury, it can also develop hours or days later, and it may persist.1,2 Thus, frequent reexamination of patients with burners is extremely important. Furthermore, the baseline strength of some athletes is so great that manual muscle testing may not detect subtle deficits.20
At initial presentation, it is critical to rule out serious injuries, such as cervical fracture, cervical dislocation or spinal cord contusion, before further evaluation is conducted. Until proved otherwise, bilateral symptoms, cervical vertebral tenderness or lower extremity findings indicate cervical fracture or spinal cord injury. The differential diagnosis also includes clavicle fracture, shoulder dislocation and acromioclavicular separation.1 When symptoms become chronic, thoracic outlet syndrome should be considered.
Diagnostic Tests
Adjunctive testing can be valuable in selected patients. Electrodiagnostic studies can confirm the diagnosis, localize the lesion and help assess the severity of the injury. Because of the cost of testing and the delay between injury and the onset of electromyographic (EMG) changes, EMG should be reserved for patients with symptoms that last at least three weeks.2,8 Electrodiagnostic studies do not always differentiate lesions of cervical roots from those in the upper trunk.2 In addition, weakness can be prolonged more than a few minutes in the absence of axonal injury (as indicated by normal EMG findings).21
Imaging is indicated in selected patients to rule out the rare occurrence of bony involvement. Radiography of the cervical spine should be performed in patients with severe neck pain, limited range of motion, weakness or recurrent injury.8,22 The radiographs should include anteroposterior, lateral and oblique views, as well as views obtained with the neck in flexion and in extension.8 Magnetic resonance imaging or computed tomography can delineate abnormalities in patients with possible involvement of the spinal cord or nerve roots. Findings from these studies should be correlated with the athlete's precise clinical presentation, because abnormalities such as foraminal narrowing can be asymptomatic.14
Management
The management of burners includes addressing predisposing factors, correcting strength deficits and enhancing protective equipment.
Flexibility and strength of the neck, shoulder and upper extremity are important, because stiffness and weakness are predisposing factors for a burner as well as consequences of this injury.2,8,23 Maintenance of a chest-out posture is also advocated. This strategy opens foramina maximally, reduces the effect of the weight of the head on nerve roots and augments the thoracic outlet, thereby decreasing pressure on the brachial plexus by the scalene muscles.23
Techniques to improve flexibility, strength and posture are part of the general approach to injuries and are recommended for patients with a burner.24,25 The first goal is to restore pain-free mobility. Strengthening is then addressed with concentric and eccentric loading at various speeds and in different directions. Sport-specific therapy follows and should be continued at least through the athletic season.20 Finally, return to athletic participation requires evaluation of the athlete's playing style. Correction of suboptimal technique should minimize the risk of reinjury.1,20 Physical therapists and athletic trainers can be invaluable in helping the physician manage the player's recovery.
The use of protective equipment is also advised (Figure 3). In football players, shoulder pads that ride high, have air floatation pads or are raised by supplemental pads called “lifters” can reduce the incidence of burners.5,6 These equipment modifications can improve shoulder pad fit, reduce direct pressure on the neck and augment shock absorption.11,23 A study of five asymptomatic football players demonstrated statistically significant limitation of cervical extension using a neck roll, a Cowboy Collar or a custom orthosis, compared with shoulder pads alone.26 The custom orthosis had the greatest effect. The Cowboy Collar and the neck roll produced similar degrees of limitation. Another study found that a padded Orthoplast orthosis improved burner symptoms in three of five football players over one season.6
FIGURE 3.
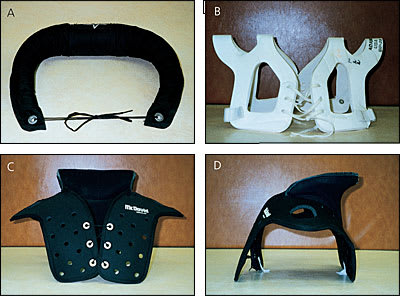
Examples of protective equipment for football players who have sustained burners. (A) A neck roll, which attaches to the shoulder pads. (B) A lifter, which is worn underneath shoulder pads. (C) Anterior view of a Cowboy Collar, which is also worn underneath shoulder pads. (D) Lateral view of a Cowboy Collar.
It is reasonable to try any of these protective devices. The neck roll is relatively inexpensive. For consistent limitation of excessive motion, the device should fit snugly below the helmet and remain in place. A custom orthosis costs more than a neck roll, but it has the advantage of individualized fit. Although limitation of excessive cervical motion is the goal, straps binding the helmet to the shoulder pads are generally considered unsafe and inappropriate.2,8
Follow-up and Return to Play
The importance of reexamination cannot be overemphasized. The patient with a burner should be evaluated at the time of injury and after the practice or game. The patient should be reexamined during the next week, again one week later and afterward as needed until symptoms resolve, motion of the neck and shoulder becomes full and pain-free, and strength returns to normal.2,8,10,16,21,24,27,28 Careful attention to slight differences between the involved and uninvolved sides is essential.
The purposes of EMG in patients with burners are to confirm the diagnosis and provide prognostic information. EMG abnormalities can persist for months or even years after motor deficits have resolved. Therefore, repeating the EMG is not recommended in deciding when or if an athlete is able to return to play.2,8,21,24
The patient must remain asymptomatic during practices in order to continue sport participation. Finally, psychologic support may be beneficial for the patient who feels apprehensive about athletic competition after a neurologic injury has resolved.20
Prognosis
Burners recur frequently. One study of college football players found that 87 percent had a recurrence.1 Another study found that of 36 athletes with neck injuries causing time loss from sports participation (most symptoms were consistent with burners), 15 (42 percent) experienced subsequent neck injuries.29
The risk of permanent nerve injury from recurrent burners has not been determined. In light of the high incidence of burners, this risk appears to be low. However, burners can clearly lead to a chronic syndrome that limits athletic participation.7
Prevention
The preparticipation examination provides an opportunity to screen for athletes at risk for burners. It is important to ask about previous burners.1 Limitations in flexibility and strength should be sought manually. Abnormalities detected by the history and physical examination should be addressed with a therapeutic plan to improve range of motion, strength and playing technique. Athletes who have already had a burner or who are identified as being at risk for this injury should consider using special protective equipment.23
Screening radiography is not done routinely. However, a study of college football players who had already sustained neck injuries found an increased risk of reinjury when neck abnormalities were detected on radiographs or physical examination.29 Until a cost-benefit analysis has been performed, screening radiography is not recommended for the general contact-sport population.
