The differential diagnosis for febrile patients with a rash is extensive. Diseases that present with fever and rash are usually classified according to the morphology of the primary lesion. Rashes can be categorized as maculopapular (centrally and peripherally distributed), petechial, diffusely erythematous with desquamation, vesiculobullouspustular and nodular. Potential causes include viruses, bacteria, spirochetes, rickettsiae, medications and rheumatologic diseases. A thorough history and a careful physical examination are essential to making a correct diagnosis. Although laboratory studies can be useful in confirming the diagnosis, test results often are not available immediately. Because the severity of these illnesses can vary from minor (roseola) to life-threatening (meningococcemia), the family physician must make prompt management decisions regarding empiric therapy. Hospitalization, isolation and antimicrobial therapy often must be considered when a patient presents with fever and a rash.
Evaluating the patient who presents with fever and a rash can be challenging because the differential diagnosis is extensive and includes minor and life-threatening illnesses. In addition, the clinical picture can vary considerably, and the family physician may need to quickly decide about initiating empiric therapy or isolation. This article reviews common diagnoses for fever and a rash and suggests a logical approach to obtaining the correct diagnosis.1–3
History
A detailed history can be quite helpful in identifying the cause of fever and a rash. A history of recent travel, woodland or animal exposure, drug ingestion or contact with ill persons should be noted. The time of year can be a clue to certain diagnoses.2–4
A complete medical history can help to determine whether the patient is at increased risk for specific conditions associated with valvular heart disease, sexually transmitted diseases or immunosuppression from chemotherapy. Immune status is particularly important because many of the diseases that result in fever and a rash present differently in immunocompromised patients.2–4
Details about the rash should include site of onset, rate and direction of spread, presence or absence of pruritus, and temporal relationship of rash and fever.2–5 It is also important to know whether any topical or oral therapies have been attempted.
Physical Examination
A basic understanding of the various types of rashes is essential in making an accurate assessment and determining the severity and acuteness of the patient's illness. Brief descriptions of common primary skin lesions are presented in Table 1.1,6
The physician should identify the primary lesion but also note the presence of secondary lesions. Important features include the distribution, configuration and arrangement of the lesions.2
In addition to evaluating the patient's vital signs and general appearance, the physician should look for the following: signs of toxicity, adenopathy, oral, genital or conjunctival lesions, hepatosplenomegaly, evidence of excoriations or tenderness, and signs of nuchal rigidity or neurologic dysfunction.2,4
TABLE 1 Common Primary Skin Lesions
| Lesion type | Description |
|---|---|
| Macule | Circumscribed area of change in normal skin color, with no skin elevation or depression; may be any size |
| Papule | Solid, raised lesion up to 0.5 cm in greatest diameter |
| Nodule | Similar to papule but located deeper in the dermis or subcutaneous tissue; differentiated from papule by palpability and depth, rather than size |
| Plaque | Elevation of skin occupying a relatively large area in relation to height; often formed by confluence of papules |
| Pustule | Circumscribed elevation of skin containing purulent fluid of variable character (i.e., fluid may be white, yellow, greenish or hemorrhagic) |
| Vesicle | Circumscribed, elevated, fluid-containing lesion less than 0.5 cm in greatest diameter; may be intraepidermal or subepidermal in origin |
| Bulla | Same as vesicle, except lesion is more than 0.5 cm in greatest diameter |
Information from Fitzpatrick TB, et al. Color atlas and synopsis of clinical dermatology: common and serious diseases. 3d ed. New York: McGraw-Hill, Health Professions Division, 1997, and Habif TP. Clinical dermatology: a color guide to diagnosis and therapy. 3d ed. St. Louis: Mosby, 1996.
Laboratory Data
Laboratory data are not usually available during the initial evaluation. The complete blood count with differential, an erythrocyte sedimentation rate, a chemistry panel, liver function tests, and blood and urine cultures may prove useful in identifying organisms or disease processes.1
Aspirates, scrapings and pustular fluid may be obtained for Gram staining and culture. When a herpes simplex virus infection is suspected, a Tzanck test may be performed by unroofing a lesion and taking a scraping of the lesion base. Biopsy samples should be obtained from nonhealing or persistent purpuric lesions. Biopsy of inflammatory dermal nodules and ulcers should also be considered.1
Specific diagnoses that may be confirmed histologically include Rocky Mountain spotted fever, herpetic infections, systemic lupus erythematosus, erythema multiforme, allergic vasculitis, secondary syphilis and deep fungal infections.1,6,7
Although serologic tests are not helpful in the acute setting, they can be used to confirm or support the diagnosis of conditions such as systemic lupus erythematosus, syphilis, rheumatoid arthritis and human immunodeficiency virus infection.1,6,7
Diseases that present with fever and rash are summarized in Table 21,2 and discussed by rash type in the following sections.
Maculopapular Rashes
Maculopapular eruptions are most frequently seen in viral illnesses (Figure 1) and immune-mediated syndromes. These eruptions can have many causes, including drug reactions and bacterial infections. Infectious exanthems are common and are defined as generalized cutaneous eruptions associated with a systemic infection. It is helpful to consider centrally and peripherally distributed eruptions separately because each type has its own differential diagnosis.2
FIGURE 1.
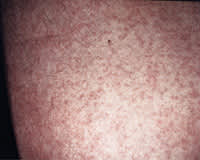
Maculopapular rash in a nonspecific viral exanthem.
CENTRALLY DISTRIBUTED ERUPTIONS
Centrally distributed maculopapular eruptions are more common than peripheral eruptions.2 These eruptions include rashes that begin centrally, first affecting the head and neck, and then progress peripherally.
Viral Exanthems. Viral etiologies of rashes include rubeola, rubella, erythema infectiosum and roseola.4
The exanthem of rubeola begins around the fourth febrile day, with discrete lesions that become confluent as they spread from the hairline downward, sparing the palms and soles. The exanthem typically lasts four to six days. The lesions fade gradually in order of appearance, leaving a residual yellow-tan coloration or faint desquamation. Rubeola is also distinguished by the presence of Koplik's spots in the oral mucosa.1,2
Rubella is similar to rubeola. However, it causes less severe symptoms, and its exanthem characteristically has a shorter duration (two to three days).1,2
Erythema infectiosum, or fifth disease, is caused by human parvovirus B19. This disease primarily affects children between three and 12 years of age, although it can present as a rheumatic syndrome in adults. The prodrome may consist of fever, anorexia, sore throat and abdominal pain. Once the fever resolves, the classic bright-red facial rash (“slapped cheek”) appears. Within several days, the exanthem progresses to a diffuse, lacy, reticular rash that may wax and wane for six to eight weeks (Figure 2). Human parvovirus B19 infection is of particular concern in pregnant women because it has been associated with fetal hydrops and subsequent fetal death.1,4,7,8
FIGURE 2.

Maculopapular rash of erythema infectiosum (fifth disease).
Roseola, or exanthema subitum, is caused by human herpesvirus 6. This disease occurs in children less than three years of age. As in fifth disease, the rash appears after the resolution of several days of high fever. The diffuse maculopapular eruption often spares the face and is of short duration, typically fading within three days.7,8
Lyme Disease and Erythema Migrans. Lyme disease is the most commonly reported vector-borne illness in the United States.7 It is caused by the spirochete Borrelia burgdorferi, which is transmitted by the bite of a tick (Ixodes species). Endemic areas in the United States include the northeastern, mid-Atlantic, north-central and far-western regions.9
Erythema migrans, the pathognomonic rash, develops in about 80 percent of patients with Lyme disease.6 This enlarging, erythematous macular rash begins as a macule or papule at the site of inoculation (Figure 3). Systemic symptoms, including fever, chills, myalgias, headaches and arthralgias, often accompany the rash.1,10
FIGURE 3.

Erythema migrans on upper arm in Lyme disease.
The rash is more common on the proximal extremities, in body creases and on the chest. It enlarges over a period of days to weeks, reaching a maximum diameter of 3 to 68 cm (median diameter: 15 cm).1,10
The primary lesion may show central clearing, central necrosis, induration or vesiculation. Smaller secondary lesions may develop in up to 20 percent of patients with Lyme disease and may indicate early hematogenous spread.10
Borrelia lymphocytoma is a painless bluish-red nodule or plaque that may develop in early Lyme disease. The lesion is usually located on the earlobe, nipple or scrotum.9
Complications of untreated Lyme disease include carditis, neuroborreliosis, arthritis and acrodermatitis chronica atrophicans.9
Drug-Related Eruptions. Drug reactions can present as any dermatologic morphology and show no predilection for age, gender or race. Exanthematous eruptions most commonly occur in association with the administration of penicillins or cephalosporins. The rash usually appears within the first week after the offending drug is started and typically resolves within days after the drug is discontinued. Drug-related reactions can be difficult to distinguish from viral exanthems, but they may be more intensely erythematous and pruritic.1,2,11
PERIPHERAL ERUPTIONS
Erythema Multiforme. The most common peripheral eruptive maculopapular rash, erythema multiforme occurs more frequently in men than in women and most often affects persons between 20 and 30 years of age. The rash, which can be recurrent, shows a predilection for palms, soles, knees and elbows. Although erythema multiforme has a number of known etiologies (Table 3),1,4,6 it is idiopathic in more than 50 percent of affected patients.1,6
TABLE 3 Etiologies of Erythema Multiforme
| Idiopathic (more than 50 percent of cases) | |
| Radiation therapy | |
| Medications | |
| Penicillin | |
| Sulfonamides | |
| Phenytoin (Dilantin) | |
| Barbiturates | |
| Phenylbutazone | |
| Infectious causes | |
| Herpes simplex virus | |
| Epstein-Barr virus | |
| Adenovirus | |
| Coxsackievirus B5 | |
| Vaccinia virus | |
| Mycoplasma species | |
| Chlamydia species | |
| Salmonella typhi | |
| Yersinia species | |
| Mycobacterium tuberculosis | |
| Histoplasma capsulatum | |
| Coccidioides immitis | |
Information from Fitzpatrick TB, et al. Color atlas and synopsis of clinical dermatology: common and serious diseases. 3d ed. New York: McGraw-Hill, Health Professions Division, 1997; Weber DI, Cohen MS, Fine JD. The acutely ill patient with fever and rash. In: Mandell GL, Bennett JE, Dolin R, eds. Mandell, Douglas, and Bennett's Principles and practice of infectious diseases. 5th ed. Philadelphia: Churchill Livingstone, 1999:633–50; and Habif TP. Clinical dermatology: a color guide to diagnosis and therapy. 3d ed. St. Louis: Mosby, 1996.
Erythema multiforme begins as a macular eruption (Figure 4). The dull-red lesions advance from macules to papules, with prominence of characteristic target-shaped lesions. Vesicles and bullae may develop in the center of the papules. In many patients, the mucous membranes of the mouth and lips are involved.1
FIGURE 4.

Erythema multiforme associated with sulfa drug administration.
[ corrected] The illness is classified as minor or major, depending on severity. In erythema multiforme minor, bullae and systemic symptoms are absent. The eruption is typically confined to the extensor surfaces of extremities and only rarely involves the mucous membranes. Recurrent episodes of erythema multiforme minor usually precede an outbreak of herpes simplex by several days. Recurrences may be prevented with chronic acyclovir (Zovirax) therapy.1
Erythema multiforme major most often results from a drug reaction. Mucous membranes are always involved. The eruption tends to become bullous and systemic symptoms, including fever and prostration, are present. Eating may be complicated by cheilitis and stomatitis, and micturition may be difficult because of balanitis and vulvitis. Conjunctivitis may be severe and can lead to keratitis and ulceration. Lesions may also be found in the pharynx, larynx and trachea. Rarely, erythema multiforme major can be life-threatening and can progress to necrotizing tracheobronchitis, meningitis, blindness, sepsis and renal tubular necrosis.1,4,6
Secondary Syphilis. The rash of secondary syphilis can be diffuse, with localized eruptions often occurring on the head, neck, palms and soles. The lesions are typically brownish-red or pink macules and papules, but they may be papulosquamous, pustular or acneiform. The eruption usually occurs two to six months after the primary infection and two to 10 weeks after the primary chancre.12
Patients often present with acute constitutional symptoms, and asymptomatic flat-topped macules and papules (mucous patches) are commonly found on the oral and genital mucosa. Classic condyloma lata may also be found in the perineum.1,6,12
Others. Meningococcemia, Rocky Mountain spotted fever and dengue fever—all potentially life-threatening infections—may initially present with erythematous maculopapular lesions before advancing to a petechial exanthem.3,13
Petechial Eruptions
Petechial rashes warrant immediate evaluation to rule out severe, life-threatening illness. For proper assessment of an acutely ill patient with a petechial rash, the physician must be familiar with the common infectious and noninfectious etiologies. Prompt, accurate diagnosis and early treatment can be life-saving in patients with meningococcemia, rickettsial infections and bacteremia.3,13
MENINGOCOCCEMIA
Meningococcal infections are a worldwide concern. These infections occur sporadically or in epidemics, most commonly in the midwinter months.1 Seeding of Neisseria meningitidis from the nasopharynx may result in acute meningococcal septicemia, meningococcal meningitis or chronic meningococcemia. The risk of meningococcal disease is highest in infants, asplenic patients, alcoholics and patients with a complement deficiency (especially C5 to C8).1
In some patients, the typical prodrome of cough, headache, sore throat, nausea and vomiting may be of short duration. Patients with acute meningococcemia appear ill and usually present with a characteristic petechial rash (Figure 5), a high, spiking fever, tachypnea, tachycardia and mild hypotension. In the early stages of disease, the rash may be maculopapular.14 Signs and symptoms of meningeal irritation may be helpful, given that up to 88 percent1 of patients with meningococcemia develop meningitis.1,13–15
FIGURE 5.

Petechiae in meningococcemia.
Chronic meningococcemia is a rare condition. Patients may present with intermittent rash, fever, arthritis and arthralgias occurring over a period of weeks to several months. In some patients, the chronic form advances to acute meningococcemia.1 The rash may be polymorphous, with maculopapular lesions usually located around a painful joint or pressure point, nodules on the lower extremities and petechiae of variable size.1,4,7,13–15
ROCKY MOUNTAIN SPOTTED FEVER
Rocky Mountain spotted fever is the most common rickettsial disease in the United States.16 It is caused by Rickettsia rickettsii, which is transmitted through a tick bite or contact with tick feces or tissue juices.1
The disease occurs most often in young men between April and September.16 In the United States, the areas with the highest prevalence of Rocky Mountain spotted fever are Oklahoma and the southern Atlantic states.6
The prodrome may include malaise, chills, a feverish feeling, anorexia and irritability. The onset of symptoms may be abrupt, with the predominant features being fever (94 percent), severe headache (86 percent), generalized myalgia (83 percent), shaking rigor, photophobia, prostration and nausea. The diagnosis can be difficult when the onset is gradual and no rash is present, as is the case in up to 20 percent of adults and 5 percent of children with Rocky Mountain spotted fever.16
When rash is present, it develops on approximately the fourth day of illness. Its appearance, combined with the temporal evolution, is characteristic of Rocky Mountain spotted fever. The rash typically begins as pink macules, 2 to 6 mm in diameter, located on the wrists, forearms, ankles, palms and soles. Within six to 18 hours, the rash spreads centrally to involve the arms, thighs, trunk and face. In the ensuing one to three days, the lesions evolve into deep-red papules. Within two to four days after onset of the rash, the lesions become petechiae.1,4,7,13,16,17
OTHER CAUSES
Viral illnesses known to cause petechial rashes include coxsackievirus A9, echovirus 9, Epstein-Barr virus and cytomegalovirus infections, atypical measles and viral hemorrhagic fevers caused by arboviruses and arenaviruses. Coxsackievirus and echovirus infections in children can produce severe illness and, at times, are difficult to distinguish from meningococcemia.4
Included in the differential diagnosis of petechial rash are disseminated gonococcal infections, bacteremia, staphylococcemia and thrombotic thrombocytopenic purpura.
Diffuse Erythema with Desquamation
SCARLET FEVER
Scarlet fever provides the classic example of an erythematous rash with subsequent desquamation. Most common between one and 10 years of age,18 scarlet fever usually follows an acute infection of the tonsils or skin by group A beta-hemolytic streptococci that produce an erythrogenic exotoxin.2 Patients may appear acutely ill and have fever, sore throat, headache, chills, nausea and vomiting.1,18
The rash begins as finely punctate erythema on the superior trunk and face two to three days after the onset of illness. The erythema quickly spreads to the extremities. When present, petechiae in the antecubital and axillary skin folds (Pastia's lines) can be helpful in making the diagnosis.1,2
Initially, the tongue may appear white, with red, swollen papillae (white strawberry tongue), but by the fourth or fifth day, it becomes bright red (red strawberry tongue). The oral mucosa may have punctate erythema or petechiae, and the tonsils may be acutely infected.1
The exanthem varies in intensity. However, it usually fades in four to five days and is followed by diffuse desquamation.1
The infection may be mild, and patients may present with only complaints of desquamation. Rarely, the streptococcal infection may produce a toxic-shock–like picture that results in hypotension and multisystem failure. Many of these patients have a localized tissue infection that progresses to necrotizing fasciitis, which usually warrants immediate surgical intervention.1,2
TOXIC SHOCK SYNDROME AND SCALDED SKIN SYNDROME
Staphylococcus aureus is the organism responsible for classic toxic shock syndrome and scalded skin syndrome. Toxic shock syndrome can present with hypotension, erythema, fever and multisystem dysfunction.3 Most cases of nonmenstrual toxic shock syndrome occur in the postoperative setting.1
Several different staphylococcal exotoxins have been implicated. The syndrome may result from infection, or it may occur because of simple colonization with S. aureus.3 Staphylococcal scalded skin syndrome occurs in infants, young children and adults with immunosuppression or renal impairment.1
The rash is usually diffuse and can present as bullous impetigo, scarlatiniform lesions or diffuse erythema (Figure 6). The mucous membranes are spared in most patients. During the physical examination, the physician should attempt to elicit Nikolsky's sign (shearing of the skin with gentle lateral pressure).1,3,4
FIGURE 6.

Diffuse erythema in toxic shock syndrome.
KAWASAKI'S DISEASE
Kawasaki's disease, or mucocutaneous lymph node syndrome, is an acute febrile illness that affects infants and young children (mean age: 2.6 years). The disease is uncommon after the age of 12 years.6
In patients with Kawasaki's disease, fever begins abruptly, and the temperature is typically higher than 40°C (104°F). The fever lasts five to 30 days (mean duration: 8.5 days) and does not respond to antibiotics and antipyretics.6,8
The rash appears within three days of the onset of fever and can vary in character. Frequently, the rash is scarlatiniform on the trunk and erythematous on the palms and soles, with subsequent distal desquamation. Mucous membrane involvement is common and includes hyperemic bulbar conjunctiva, injected oropharynx, dry, cracked lips and a strawberry tongue.1,6
The physical examination may reveal non-suppurative cervical lymphadenopathy (more than 1.5 cm in diameter). Coronary artery abnormalities develop in 20 to 25 percent of patients with Kawasaki's disease.19 Cardiovascular complications are the major cause of short-term and long-term morbidity and mortality.1,6,8,19
OTHER CAUSES
Ehrlichiosis, a rickettsial-like infection, can occasionally be associated with a clinical picture similar to toxic shock syndrome, including diffuse erythema. Streptococcus viridans bacteremia is another rare cause of generalized erythema. Finally, enteroviral infections, toxic epidermal necrolysis, graft-versus-host reaction, erythroderma and generalized pustular psoriasis (von Zumbusch's psoriasis) may present with diffuse erythema.1,3
Vesiculobullous-Pustular Eruptions
VARICELLA-ZOSTER VIRUS INFECTIONS
Varicella-zoster virus is the most infectious of the human herpesviruses. It is responsible for varicella (chickenpox) and herpes zoster (shingles).20
Varicella. Primary infection with varicella-zoster virus results in chickenpox, a common childhood illness. Its highest incidence is in late winter and spring.2 The disease is typically more severe in adults and immunocompromised patients.1,6
The clinical presentation consists of rash, fever and general malaise.2 A mild prodrome lasting one to two days before appearance of the rash is not uncommon. The rash typically begins on the face, scalp or trunk and then spreads to the extremities.8
The lesions appear as erythematous macules and progress to papules with an edematous base (Figure 7). The papules quickly evolve into vesicles, with each vesicle initially having the appearance of “a dewdrop on a rose petal.”1 The vesicles evolve into pustules, which become umbilicated and subsequently crust over in the ensuing eight to 12 hours. An enanthema may be noted, and vesicles may evolve to shallow erosions, primarily on the palate. On physical examination, lesions in all stages may be present.1
FIGURE 7.

Rash of varicella (chickenpox).
Complications are unusual in immunocompetent patients. In children, the most common complication is secondary bacterial infection of excoriated lesions.7
The central nervous system (CNS) is the most common site of extracutaneous involvement in children. Cerebellar ataxia is the most frequently encountered syndrome. Other possible CNS complications include encephalitis, meningitis, transverse myelitis and, rarely, Reye's syndrome (especially subsequent to aspirin use). Varicella pneumonia and encephalitis can be serious complications in adults. Additional rare complications in children and adults include myocarditis, corneal lesions, nephritis, arthritis, bleeding diatheses, acute glomerulonephritis and hepatitis.1,2,7,21
Herpes Zoster. After the primary infection, the varicella-zoster virus lies dormant in the dorsal root ganglia. Herpes zoster is caused by reactivation of the virus.20 Although shingles can occur at any age, its incidence increases significantly with age and in immunocompromised patients. An estimated 10 to 20 percent of the general U.S. population will have herpes zoster at some time in life.20
The characteristic vesicular rash of herpes zoster usually affects a single dermatome and rarely crosses the midline (Figure 8). The most common locations are the chest (approximately 50 percent of cases) and the face (approximately 20 percent of cases).20 A prodrome of unusual skin sensations may evolve into pain, burning and paresthesias, which precede the rash by two to three days.
FIGURE 8.

Dermatomal distribution of rash in herpes zoster.
The rash begins as an erythematous maculopapular eruption that rapidly evolves to a vesicular rash.21 In about 5 percent of patients, the rash may be accompanied by headache, malaise and fever.1 Drying of the lesions with crust formation generally occurs in seven to 10 days, and the lesions usually resolve in 14 to 21 days.20
Pain is the most debilitating feature of herpes zoster, and postherpetic neuralgia is the most common long-term complication. Post-herpetic neuralgia is uncommon in young patients but may affect as many as 50 percent of patients more than 50 years of age.21
Other potential complications of herpes zoster include secondary infection, meningo-encephalitis, transverse myelitis, pneumonitis, hepatitis, myocarditis, pancreatitis, esophagitis, cystitis, granulomatous arteritis, conjunctivitis and Ramsay Hunt syndrome (herpes zoster involving the facial and auditory nerves). When herpes zoster affects the eye (herpes zoster ophthalmicus), an ophthalmologist should always be consulted.1,20,21
OTHER CAUSES
Staphylococcal bacteremia may present with a widespread pustular eruption. Gonococcemia may also produce a pustular rash, although other lesion types, such as macules, petechiae and papules, are usually present.3
In immunocompromised patients, disseminated herpes simplex virus infection must be considered. Patients with underlying liver disease, renal dysfunction or diabetes are particularly susceptible to infection with Vibrio vulnificus, which is acquired from eating seafood, exposure to sea water or injury when handling crabs. Rickettsia akari, transmitted by a house mite, is the cause of rickettsialpox, a mild disease characterized by a local eschar, a papulovesicular rash and a mild clinical course.1–4,12
Nodular Eruptions
ERYTHEMA NODOSUM
Erythema nodosum is an acute inflammatory and immunologic process involving the panniculus adiposus (the fatty tissue layer underlying the skin).1 A number of etiologies have been identified (Table 4).1,4 This condition is more common in women than in men.
TABLE 4 Etiologies of Erythema Nodosum
| Idiopathic (40 percent of cases) | ||
| Infectious causes | ||
| Beta-hemolytic streptococci | ||
| Yersinia species | ||
| Hepatitis C virus | ||
| Mycobacterium species | ||
| Chlamydia trachomatis | ||
| Coccidioides immitis | ||
| Noninfectious causes | ||
| Medications | ||
| Sulfonamides | ||
| Oral contraceptives | ||
| Systemic lupus erythematosus | ||
| Sarcoidosis | ||
| Ulcerative colitis | ||
| Behçet's syndrome | ||
| Pregnancy | ||
Information from Fitzpatrick TB, et al. Color atlas and synopsis of clinical dermatology: common and serious diseases. 3d ed. New York: McGraw-Hill, Health Professions Division, 1997, and Weber DI, Cohen MS, Fine JD. The acutely ill patient with fever and rash. In: Mandell GL, Bennett JE, Dolin R, eds. Mandell, Douglas, and Bennett's Principles and practice of infectious diseases. 5th ed. Philadelphia: Churchill Livingstone, 1999:633–50.
Presenting features often include fever, malaise and arthralgias. The characteristic nodules are painful and tender. The lesions most often develop on the lower legs, knees and arms (Figure 9). The course of erythema nodosum depends on the specific cause, but spontaneous resolution can be expected within six weeks.1,2
FIGURE 9.

Erythema nodosum.
OTHER CAUSES
In immunocompromised patients, disseminated fungal infections may produce nodular lesions. Disseminated candidiasis may present with diffuse nonerythematous nodules in an immunocompromised patient who has fever and myalgias. Other fungal infections to consider include cryptococcosis, blastomycosis, histoplasmosis, coccidioidomycosis and sporotrichosis.2
