Paraphimosis is a urologic emergency, occurring in uncircumcised males, in which the foreskin becomes trapped behind the corona and forms a tight band of constricting tissue. Often iatrogenically induced, paraphimosis can be prevented by returning the prepuce to cover the glans following penile manipulation. Treatment often begins with reduction of edema, followed by a variety of options, including mechanical compression, pharmacologic therapy, puncture technique and dorsal slit. Prevention and early intervention are key elements in the management of paraphimosis.
Paraphimosis is one of the few urologic emergencies that may be encountered in general practice.1–3 It is a condition in which the foreskin, once pulled back its original position. Paraphimosis only occurs in uncircumcised or partially circumcised males. Paraphimosis must be distinguished from phimosis, a nonemergency condition in which the foreskin cannot be pulled back.
If left untreated, paraphimosis can have severe consequences. Vigilance in returning the foreskin to its natural position following foreskin manipulation is the key to preventing paraphimosis. When paraphimosis is suspected, a urology consultation should be obtained for prompt evaluation and treatment.
Etiology
The cause of paraphimosis is most often iatrogenic; the condition frequently occurs after penile examination, urethral catheterization or cystoscopy. Paraphimosis typically occurs after Foley catheter placement. During the insertion of a urethral catheter, the foreskin is retracted to prepare and drape the glans penis. After insertion of the catheter, the practioner may not return the retracted foreskin to its normal position.
Rare causes of paraphimosis include self-inflicted injury to the penis (such as piercing a penile ring into the glans4) and paraphimosis secondary to penile erections.5
Pathophysiology
When the foreskin becomes trapped behind the corona for a prolonged time, it may form a tight, constricting band of tissue. This circumferential ring of tissue can impair the blood and lymphatic flow to and from the glans and prepuce. As a result of penile ischemia and vascular engorgement, the glans and prepuce may become swollen and edematous. If left untreated, penile gangrene and autoamputation may follow in days or weeks.6
Clinical Presentation
A patient with paraphimosis often presents with penile pain. However, pain may not always be present. The glans appears enlarged and congested, with a collar of swollen foreskin around the coronal sulcus. A tight, constricting band of tissue appears immediately behind the head of the penis (Figure 1). The remainder of the penile shaft is flaccid and unremarkable. Infants and children with paraphimosis may present with obstructive voiding symptoms and, when severe, acute urinary obstruction.7
FIGURE 1.

Paraphimosis.
Evaluation
When evaluating a patient with suspected paraphimosis, a detailed history must be obtained regarding penile manipulation, instrumentation or endoscopic surgery of the bladder or urethra. Any history of self-retraction should also be elicited. The patient must be asked whether he has been circumcised or partially circumcised. Changes in skin texture and color can make this determination difficult based on visual inspection alone.
The physical examination should focus on the penis, urethral catheter (if present) and scrotum. The penis should be inspected for the presence of foreskin, the color of the glans, the degree of constriction around the penile corona and turgor of the prepuce. Absence of foreskin excludes the diagnosis of paraphimosis. A pink or salmon hue to the glans indicates a good blood supply. If the glans or prepuce appears to be black, autonecrosis has begun. Palpation of the glans can provide additional information on the viability of the glans. A normal glans is soft and pliant. If the glans feels firm and inelastic, with black areas present, penile necrosis should be suspected.
Patients with paraphimosis often have an indwelling urethral catheter. Removal of the catheter before manipulating the penis will aid in successful reduction of paraphimosis. However, the reason for the initial placement of the catheter should be obtained first so that, if necessary, it can be replaced following reduction of the paraphimosis.
Scrotal skin should be inspected for color, texture and turgor. Scrotal contents should be palpated for tenderness, hydrocele or tumor.
Treatment
The treatment of paraphimosis involves reducing the penile edema and restoring the prepuce to its original position. There are no prospective, randomized, controlled studies comparing the efficacy of currently available treatment options. Several noninvasive or minimally invasive methods are used to reduce the penile swelling. Because of extreme pain, patients may require a penile nerve block (Figure 2), topical analgesic or oral narcotics before penile manipulation.8 In infants and children, a topical anesthetic such as 2 percent lidocaine gel or 2.5 percent prilocaine and 2.5 percent lidocaine (Emla cream) applied to the skin for several minutes to an hour before penile manipulation is effective.
FIGURE 2.
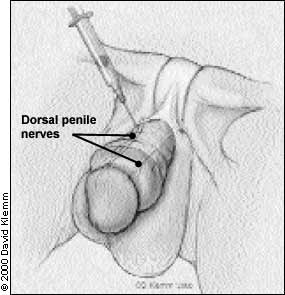
Penile nerve block.
MANUAL REDUCTION
Manual pressure may reduce edema. A gloved hand is circled around the distal penis to apply circumferential pressure and disperse the edema. Ice packs are also useful in reducing swelling of the penis and prepuce.9 The penis is first wrapped in plastic, with ice packs applied intermittently until the swelling subsides. To reduce edema, a compressive elastic dressing is then wrapped circumferentially around the penis from the glans to the base. This dressing should be left in place for five to seven minutes,10 and the penis should be checked periodically to monitor the resolution of swelling. Once the swelling has subsided, the wrap should be removed.
PHARMACOLOGIC THERAPY
Injection of hyaluronidase into the edematous prepuce is effective in resolving edema and allowing the foreskin to be easily reduced.11 Degradation of hyaluronic acid by hyaluronidase enhances diffusion of trapped fluid between the tissue planes to decrease the preputial swelling. Hyaluronidase is well suited for use in infants and children.
Granulated sugar has shown to be effective in the treatment of paraphimosis,12 based on the principle of fluid transfer occuring through osmotic gradient. Granulated sugar is generously spread on the surface of the edematous prepuce and glans. The hypotonic fluid from the edematous prepuce travels down the osmotic gradient into the sugar, reducing the swelling and allowing for manual reduction. Both of the procedures mentioned here should be performed by a physician experienced in these techniques.
MINIMALLY INVASIVE THERAPY
The “puncture” technique is a minimally invasive therapy in which a hypodermic needle is used to directly puncture the edematous prepuce.13,14 Puncture sites permit safe and effective evacuation of the trapped fluid. External drainage of the trapped fluid allows for manual reduction of paraphimosis.
Blood aspiration of the tourniqueted penis may be attempted.15 The base of the penis is temporarily tied off with a rubber tourniquet. An 18-gauge needle is inserted into the penis, and corporal blood is aspirated to reduce penile swelling. These techniques should only be performed by a physician experienced in the procedures.
All of these techniques are geared toward reducing the swelling so that manual reduction can be performed. After the preputial swelling has subsided, paraphimosis is reduced. To reduce the prepuce, the thumbs of both hands are placed on the glans and the fingers wrap behind the prepuce. A gentle but steady and forceful pressure is applied to the glans with the thumbs, and countertraction is applied to the foreskin with the fingers as the prepuce is pulled down (Figure 3). When performed properly, the constricting band of tissue should come down distal to the glans with the prepuce.
FIGURE 3.

Manual reduction of paraphimosis.
SURGICAL THERAPY
If a severely constricting band of tissue precludes all forms of conservative or minimally invasive therapy, an emergency dorsal slit should be performed. This procedure should be performed with the use of a local anesthetic by a physician experienced with the technique.
The penis and prepuce are prepared with a povidone-iodine solution and draped. Two straight hemostats are applied to crush the foreskin at the 12 o'clock position perpendicular to the corona. After two minutes, the prepuce between the hemostats is sharply incised, releasing the constricting band of tissue. The incisions are approximated with 4-0 absorbable suture. Circumcision, a definitive therapy, should be performed at a later date to prevent recurrent episodes, regardless of the method of reduction used.
