Flexible sigmoidoscopy remains a common tool used for the periodic screening of colorectal cancer. Most organizations recommend screening at three- to five-year intervals beginning at age 50 for persons with average risk. Extensive training in endoscopic maneuvering, colorectal anatomy and pathologic recognition is required. Most physicians report comfort performing the procedure unsupervised after 10 to 25 precepted sessions. The procedure involves the insertion of the sigmoidoscope through the anus and distal rectum and advancement of the scope tip to an average depth of 48 to 55 cm in the sigmoid colon. Once the sigmoidoscope has been appropriately advanced, the scope is slowly withdrawn, allowing for the inspection of colon mucosa during withdrawal. Polyps less than 5 mm in diameter should be biopsied. Polyps 5 to 10 mm or greater can be assumed to be adenomatous, and follow-up colonoscopy for complete polypectomy is required. Diverticulosis, hemorrhoids, nonspecific colitis and pseudomembranes may also be encountered during inspection. Use of preprocedural benzodiazepines can be helpful in reducing patient discomfort.
The most promising strategy for reducing the burden of colorectal cancer is periodic screening. Flexible sigmoidoscopy has been widely recommended at intervals of three to five years because of its sensitivity for detecting early cancers and adenomas. This examination is believed to be a cost-effective intervention for family physicians.
In most series, the average depth of insertion of the long flexible sigmoidoscope ranged between 48 and 55 cm. It is thought that about 60 percent of all colorectal cancers are within reach of the sigmoidoscope. The three- to five-year screening interval recommendation is based, in part, on estimates that seven to 10 years are required for an adenoma to progress to malignancy. Most organizations recommend initiating sigmoidoscopy screening at age 50 for persons of average risk.
An important limitation to the effectiveness of screening for colorectal cancer is the ability of patients and physicians to comply with testing. Flexible fiberoptic sigmoidoscopy is considered by many patients to be uncomfortable, embarrassing and expensive, and patients may be reluctant to agree to the testing. Studies of populations that are repeatedly advised to undergo sigmoidoscopy have found that only 10 to 30 percent of persons agree to the procedure. Physician motivation is important in encouraging patient compliance for undergoing the procedure. Physicians report that the lengthy procedure time and the extensive training needed to master the technique limit their use of the sigmoidoscope. Once a physician becomes experienced in endoscopic techniques, however, sigmoidoscopy procedures can be performed routinely in fewer than 10 minutes.
Methods and Materials
PATIENT PREPARATION
Confirm that the patient performed the recommended enemas and bowel preparation. The patient should remove clothing from below the waistline and should be seated on the examination table with a disposable sheet draped over the legs. Place an absorbent sheet beneath the patient on the table.
EQUIPMENT
Nonsterile Tray
Place the following items on a nonsterile drape on a Mayo stand:
Two or three nonsterile gloves (some physicians double-glove the right hand and remove the outer glove after the rectal examination and anoscopy)
1 inch of 4 × 4 gauze
1 inch of water-soluble (K-Y) jelly dispensed on one corner of the drape
1 inch of 5 percent lidocaine ointment dispensed on one corner of the drape
An emesis basin filled with water for suction at the end of the procedure Ive's anoscope
Endoscopy Cart
Water bottle filled and connected to the light source
Suction unit plugged into the wall outlet and connected to the scope
Light source plugged into the wall outlet and sigmoidoscope connected to the light source.
The operation of the sigmoidoscope should be checked before the procedure: air should be bubbled into the basin of water, and some of the water suctioned through.
Biopsy forceps should be available (if in sterile packaging, do not open until the forceps are needed).
Procedure Description
1. The patient is placed in the left lateral decubitus position. A rectal examination is performed with the gloved finger, examining the prostate in the male patient and confirming anal patency. The gloved examining finger can be lubricated with 2 percent lidocaine jelly (Xylocaine) or 5 percent lidocaine ointment to provide topical anesthesia of the anal canal for anoscope and sigmoidoscope insertion.
2. The lubricated slotted Ive's anoscope is lubricated with water-soluble (K-Y) jelly or additional lidocaine jelly and inserted into the anal canal. The three hemorrhoid pads (right posterior, right anterior and left lateral) should be inspected individually, necessitating insertion of the scope three times, to examine for anal canal pathology.
3. The distal portion of the flexible sigmoid oscope is lubricated with water-soluble jelly, but the jelly is kept off the most distal tip to avoid smearing the lens and distorting the image. The scope is inserted into the rectum, either by direct insertion into the anus or by pushing the scope tip into the anus by flexing the index finger behind the scope.
4. Once the scope is in the rectum (7 to 15 cm inserted), air is insufflated, fluid that may be present is suctioned, and the lumen is located by moving the tip of the scope. While some examiners have the nurse or assistant insert the scope, better control of the scope tip is achieved if the right hand inserts the scope and rotates the tip to the right and left. The examiner's left thumb moves the scope tip up and down by moving the inner knob on the scope head.
5. The scope is inserted only while the lumen is visualized. Attempt to insert the scope as quickly as possible, thereby limiting patient discomfort. Special insertion techniques, such as torquing (twisting the scope in the right hand), dithering (rapid, short back-and-forth motions to advance the scope), accordionization (pulling back on angled portions of colon wall with the scope tip, allowing the scope tip then to advance with the colon folded—like an accordion— onto the scope) and hooking and straightening (Figure 1) may be required to negotiate the many turns in the sigmoid. The colon mucosa is inspected as the scope is with drawn, and biopsies are obtained only if needed.
FIGURE 1.
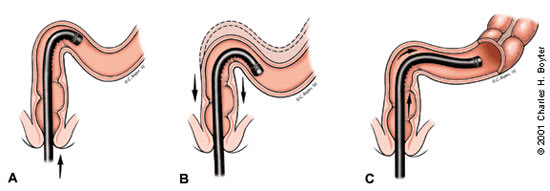
Hooking and straightening technique used to pass through a tortuous sigmoid colon. (A) The scope is inserted to the angled sigmoid. (B) The scope tip is turned to a sharp angle, and the sigmoid is hooked as the scope is withdrawn. (C) The sigmoid is straightened as the scope is withdrawn. The scope can then be inserted through to the descending colon.
6. Once the scope tip is withdrawn to the rectum (10 to 15 cm inserted), the scope tip is retroverted to examine the distal rectal vault. This area is not visualized well by the for ward-directed scope as it is inserted or with drawn. Retroversion is achieved by maximally deflecting the inner knob with the left thumb while simultaneously inserting the scope with the right hand. This maneuver should pro duce an image of the black scope as it enters the rectum from the anal canal.
7. Air is withdrawn from the rectum before removing the scope. The scope is immediately immersed in a basin of water, and the suction channel is flushed to prevent clogging of this channel by stool that may have entered the channel during the procedure. The anus is wiped clear with gauze, and the patient is offered the opportunity to go to the bathroom. Once the patient is dressed, he or she can be moved to a chair for postprocedure counseling while the scope is cleaned and disinfected.
Anatomy and Pathology Recognition During Sigmoidoscopy
1. As the scope is inserted into the rectum, a red-out may develop if the scope tip is pushed up against the colon wall. The scope tip can be slowly withdrawn and air inserted until the lumen appears. The normal rectal mucosa demonstrates a nonfriable vascular network. Proctitis produces an erythematous, friable mucosa, often with bleeding. Preprocedure enemas given to clear the colon may produce some patchy or streaky erythema, which should not be confused with proctitis.
2. The semilunar valves of Houston generally appear as sharp edges protruding into the lumen, with dark shadows noted behind. These valves protrude from different sides of the rectum and are more easily seen with air in sufflation or when the scope is withdrawn on exiting the colon. The physician should examine for pathology behind the valves. Ulcerative colitis usually produces erythema, friability and mucosal bleeding, which may extend from the anus upward throughout the colon.
3. As the scope enters the sigmoid, redundant folds (with a loss of vascularity) obliterate the lumen. Air insufflation is necessary to identify the lumen. Extensive turning of the scope tip, torquing, accordionization or dithering techniques may be needed to negotiate the marked sigmoid turns. The examiner should avoid bowing out the sigmoid, which happens when the midscope is inserted into a sigmoid loop but the scope tip fails to advance (Figure 2).
FIGURE 2.
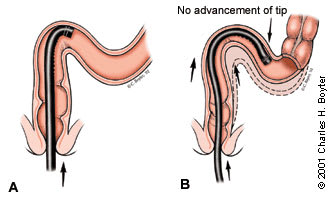
Paradoxic insertion. (A) The scope is bowing out the sigmoid colon, which has a mobile mesenteric attachment. (B) Paradoxic insertion describes the insertion of the tube without advancement of the scope tip. Paradoxic insertion can be very uncomfortable for the patient.
4. The descending colon appears as a long tube ringed with concentric haustrae. The vascularity of the descending colon appears as a random reticular pattern. Diverticular openings may be seen here, appearing as dark circles in the colon wall. Polyps may appear as a mound in the mucosa (sessile) or on a long stalk (pedunculated). Because mucus adherent to the colon wall can be mistaken for a sessile polyp, bulges in the wall can be tapped with the scope tip to see if they wipe off. Colon cancers can often be recognized by the irregular growth or mucosal pattern, or by bleeding or narrowing of the lumen.
5. The splenic flexure sometimes can be reached with the 60-cm sigmoidoscope. The splenic flexure can appear as a dead end and, if the turn is negotiated, the triangular shape to the transverse colon may be visualized. Crohn's disease can produce mucosal cobblestoning, friability, and “skip areas,” with normal mucosa separating areas of erythematous or diseased colon.
6. The last area to be visualized as the scope is withdrawn is the rectal vault. Because the lateral portions of the distal rectum are not well visualized by the forward-directed scope, the scope tip can be retroverted. The scope is seen entering the rectum from the anal canal, and the upper extent of internal hemorrhoids can be identified.
Follow-Up
- Diminutive polyps (less than 5 mm in diameter) cannot be classified by visual inspection. All polyps smaller than 5 mm should be sampled for biopsy. If the polyp is hyperplastic, no further treatment is necessary, because hyperplastic polyps are not associated with polyps in the proximal (right) colon. If the polyp is adenomatous (tubular, villous, etc.), a full colonoscopy should be performed to look for synchronous proximal polyps.
- Larger polyps (larger than 5 to 10 mm in diameter) generally are adenomatous and do not require a biopsy at sigmoidoscopy because they should be completely removed. Polypectomy is performed during colonoscopy to facilitate the search for any additional polyps.
- If a suspected cancer is encountered (an irregular, obstructing, friable or bleeding mass), it may be sampled for biopsy, but vigorous bleeding of the lesion may ensue. Prompt referral is suggested.
- Diverticulosis is believed to result from the colon's exposure to excessive intraluminal pressure. Patients with diverticulosis can be offered stool-bulking agents to soften the stools and reduce stool transit time. Patients with diverticulosis are often told to avoid nuts and seeds in their diet to prevent an undigested seed from clogging a diverticular opening, although there is little evidence suggesting this.
- Hemorrhoids are commonly encountered during sigmoidoscopy. Surgical or ablative therapies can be considered, but the hemorrhoids often shrink with administration of stool-bulking agents and efforts to promote soft stools.
- Nonspecific colitis is a frequent finding with many causes. While multiple biopsies are recommended, they often cannot identify the etiology of the colitis or distinguish Crohn's disease from ulcerative colitis. Referral can be made, although some physicians may consider empiric treatment with salicylate-based anti-inflammatory medications or hydrocortisone enemas.
- Pseudomembranes may be encountered in a patient with diarrhea. A recent history of antibiotic use should be sought, and endoscopic brushings or stool samples for Clostridium difficile can confirm the diagnosis. Treatment with vancomycin (Vancocin) or metronidazole (Flagyl) may be considered.
Procedure Pitfalls/Complications
- The Image Frequently Appears as a Red-Out. When the scope tip is up against the colon wall, the image becomes blurred into a red-out. Whenever a red-out is encountered, additional air can be insufflated, and the scope tip should be withdrawn until the lumen is relocated.
- The Patient Complains of Severe Pain During the Examination. Discomfort during the examination results from several factors, including the insertion technique. Over inflation of the colon with air can cause discomfort, sweating and a vagal response. Lengthy procedure times also produce discomfort. Physicians should strive to limit the insertion time to five minutes, with more time used to examine the colon on withdrawal of the scope. Premedication with diazepam (Valium) or triazolam (Halcion) can be considered for anxious patients, and the patient's back can be rubbed by the nurse or assistant during the most uncomfortable parts of the examination.
- The Scope Tip Does Not Seem to Advance When Inserted. The sigmoid portion of the colon can be bowed out with scope insertion, often with no advancement of the scope tip. This sigmoid bowing, however, can produce significant discomfort. When insertion of the scope fails to advance the tip, consider twisting or torquing the scope to effectively provide more rigidity to the flexible distal portion of the scope to facilitate insertion.
- The Slide-By Technique to Pass Through the Sigmoid Involves Some Risk. The slide-by technique inserts the scope by pushing the scope tip along the colon wall. This technique involves some risk. By pressing the scope against the colon wall, tears and bleeding can occur in the mesentery supporting the colon. Perforations may be more common when the slide-by technique is used. Many experts strongly recommend insertion of the scope only when the lumen can be visualized.
- Retroversion of the Scope Tip at the End of the Procedure Seems Unnecessary. Retroverting the scope tip allows for visualization of the lateral portions of the distal rectum. Because this area is not well visualized by the forward-directed scope, small polyps or cancers can fail to be detected unless retroversion is performed.
- A Diverticular Opening Is Large Enough to Allow for Insertion of the Scope Tip. Occasionally, diverticular openings are so large that they can be mistaken for the colon lumen. Because diverticula have very thin walls, entering a diverticula can easily lead to a perforation. Acute diverticulitis can produce an erythematous, swollen or bleeding diverticular opening. Sliding the scope past an acutely inflamed diverticular opening can result in significant complications. If such an opening is encountered, the scope should be immediately withdrawn.
- Inflammatory Bowel Disease Cannot Be Definitively Diagnosed Visually. Colitis can result from many causes including infection, autoimmune disorders and medications. The diagnosis may not be apparent from the visual appearance of the colon, and biopsies can help to identify the cause of colitis. Biopsies, however, may not be able to differentiate Crohn's disease form ulcerative colitis.
- The Patient Requests That the Endoscopy Be Terminated Early in the Procedure. Scope insertion should not continue against the patient's wishes. Legal concerns over the disregard for the patient's rights make it imperative that physicians not advance the scope over the objections of the patient.
Physician Training
Physicians can benefit from a comprehensive course on sigmoidoscopy, such as the one offered by the American Academy of Family Physicians. Physicians need to be well versed in pathology recognition, and many good atlases can be consulted for this. Physicians can practice the manual skills of scope manipulation on models. Great debate exists over the minimum number of procedures needed for competency. Gastroenterology organizations have suggested procedure numbers of 25 to 100 before privileges are granted. Many physicians have demonstrated good skills after just 10 procedures. Physicians should strive to have as many supervised procedures as they need to be comfortable with scope insertion and pathology recognition. Most physicians achieve comfort after 10 to 25 procedures. Unsupervised procedures should not be performed unless the physician has had some precepted experience.
This article is adapted with permission from Zuber TJ. Office Procedures. Baltimore: Lippincott Williams & Wilkins, 1999.
