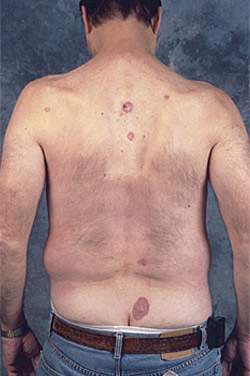
A 54-year-old man presented with multiple erythematous and eroded patches and thin plaques scattered on the trunk. They were demarcated sharply, were minimally scaling, and varied in size from 2 to 12 cm (Figures 1 and 2). The lesions were chronic and progressed slowly over many years. The patient was diagnosed with plaque psoriasis. Treatment with topical steroids for about two years led to no improvement. The patient’s Hodgkin’s disease had been treated more than 40 years ago with radiation therapy to the trunk.
Figure 1.

Figure 2.
Question
Based on the patient’s history, course of the disease, and physical examination, which one of the following is the most likely diagnosis?
A. Basal cell carcinoma.
B. Chronic radiation dermatitis.
C. Bowen’s disease.
D. Extramammary Paget’s disease.
E. Plaque psoriasis.
Discussion
The answer is A: basal cell carcinoma. Superficial basal cell carcinoma is found most commonly on the trunk and extremities. Typically, the tumors are characterized by an erythematous macule, patch, or thin plaque with a fine scale or irregular superficial erosion. The lesions exhibit little tendency to ulcerate or invade, and enlarge slowly. Close examination of the edges of the lesion shows a “rolled” raised border. Sometimes the lesions heal at one place with a white atrophic scar and then spread actively to the neighboring skin. There may be several dozen lesions, some of which may coalesce to form extensive plaques.1,2
This type of basal cell carcinoma occurs most frequently in persons with chronic arsenic exposure3 and as a late sequela of radiation therapy.4 An association between superficial basal cell carcinoma and frequent radiography has been suggested but not proven.
Superficial basal cell carcinoma often is found in younger adults (mean age: 56.8 years) and constitutes 9 to 11 percent of all basal cell carcinomas. The diagnosis usually is made clinically, based on the characteristic appearance of the lesions, and is confirmed with biopsy.
Depending on the patient, and on the size and location of the lesion, superficial basal cell carcinoma may be treated with simple excision, Mohs’ micrographic surgery, or curettage and electrosurgery. The topical application of 5-fluorouracil or imiquimod (Aldara) is effective but is an off-label use and is best used in patients who are not surgical candidates.5
Chronic radiation dermatitis results from exposure to any type of ionizing radiation. It is an end-stage of events that follows the exposure, leading to a combination of skin atrophy, hypo- and hyperpigmentation, and telangiectases.
Bowen’s disease is an intraepidermal squamous cell carcinoma. It may be found on any part of the body as a scaly and crusted patch from a few millimeters to many centimeters in diameter. The lesion is demarcated sharply and the scale often is thick.
The most common site of extramammary Paget’s disease is the vulva, followed in decreasing frequency by the perianal area, penis, scrotum, and groin. The disease begins as an erythematous crusted or keratotic, circumscribed, pruritic patch. It may simulate eczematous dermatitis.
The lesions frequently are mistaken for plaque psoriasis, which usually demonstrates erythematous plaques with thick, often lamellar scale and good initial response to topical steroids. Plaque psoriasis is the most common type of psoriasis.
Selected Differential Diagnosis of Erythematous Scaly Plaques
| Condition | Characteristics |
|---|---|
| Superficial basal cell carcinoma | Focal erosion; tends to ulcerate; “rolled” raised border |
| Chronic radiation dermatitis | Localized squamous cell carcinoma; raised center; pale or erythematous |
| Bowen’s disease | Usually solitary lesion |
| Extramammary Paget’s disease | Typically located on genitalia, perianal area; slowly enlarging and ulcerating pruritic plaque |
| Plaque psoriasis | Well demarcated, erythematous, diffusely scaly with thick adherent scale; erosions and ulcers are uncommon; good response to topical steroids |
