Benign paroxysmal positional vertigo, acute vestibular neuronitis, and Ménière’s disease cause most cases of vertigo; however, family physicians must consider other causes including cerebrovascular disease, migraine, psychological disease, perilymphatic fistulas, multiple sclerosis, and intracranial neoplasms. Once it is determined that a patient has vertigo, the next task is to determine whether the patient has a peripheral or central cause of vertigo. Knowing the typical clinical presentations of the various causes of vertigo aids in making this distinction. The history (i.e., timing and duration of symptoms, provoking factors, associated signs and symptoms) and physical examination (especially of the head and neck and neurologic systems, as well as special tests such as the Dix-Hallpike maneuver) provide important clues to the diagnosis. Associated neurologic signs and symptoms, such as nystagmus that does not lessen when the patient focuses, point to central (and often more serious) causes of vertigo, which require further work-up with selected laboratory and radiologic studies such as magnetic resonance imaging.
One of the most common and frustrating complaints patients bring to their family physicians is dizziness. There are four types of dizziness: vertigo, lightheadedness, presyncope, and dysequilibrium.1 The most prevalent type is vertigo (i.e., false sense of motion), which accounts for 54 percent of reports of dizziness in primary care.2 The differential diagnosis of vertigo (Table 11–6 ) includes peripheral vestibular causes (i.e., those originating in the peripheral nervous system), central vestibular causes (i.e., those originating in the central nervous system), and other conditions. Ninety-three percent of primary care patients with vertigo have benign paroxysmal positional vertigo (BPPV), acute vestibular neuronitis, or Ménière’s disease.7 Other causes include drugs (e.g., alcohol, aminoglycosides, anticonvulsants [phenytoin (Dilantin)], anti-depressants, antihypertensives, barbiturates, cocaine, diuretics [furosemide (Lasix)], nitroglycerin, quinine, salicylates, sedatives/hypnotics),8,9 cerebrovascular disease, migraine, acute labyrinthitis, multiple sclerosis, and intracranial neoplasms. Much confusion surrounds the nomenclature of acute vestibular neuronitis because the term “labyrinthitis” often is used interchangeably with it. Labyrinthitis (i.e., inflammation of the labyrinthine organs caused by infection) is distinct from acute vestibular neuronitis (i.e., inflammation of the vestibular nerve), and the terms are not interchangable.1
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendations | Evidence rating | References | Comments |
|---|---|---|---|
| Use the Dix-Hallpike maneuver to diagnose BPPV. | C | 7,10 | The Dix-Hallpike maneuver has a positive predictive value of 83 percent and negative predictive value of 52 percent for the diagnosis of BPPV. |
| Do not use laboratory tests to initially identify the etiology of dizziness. | C | 10 | Laboratory tests identify the etiology of vertigo in less than 1 percent of patients with dizziness. |
| Consider radiologic studies in patients with neurologic signs and symptoms, risk factors for cerebrovascular disease, or progressive unilateral hearing loss. | C | 19 | — |
| Use MRI for diagnosing vertigo when neuroimaging is needed. | C | 26 | MRI is superior to computed tomography for the diagnosis of vertigo because of its superior ability to visualize the posterior fossa. |
BPPV = benign paroxysmal positional vertigo, MRI = magnetic resonance imaging.
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, see page 196 orhttps://www.aafp.org/afpsort.xml.
TABLE 1 Differential Diagnosis of Vertigo
| Cause | Description |
|---|---|
| Peripheral causes | |
| Acute labyrinthitis | Inflammation of the labyrinthine organs caused by viral or bacterial infection |
| Acute vestibular neuronitis (vestibular neuritis)* | Inflammation of the vestibular nerve, usually caused by viral infection |
| Benign positional paroxysmal vertigo (benign positional vertigo) | Transient episodes of vertigo caused by stimulation of vestibular sense organs by canalith; affects middle-age and older patients; affects twice as many women as men |
| Cholesteatoma | Cyst-like lesion filled with keratin debris, most often involving the middle ear and mastoid |
| Herpes zoster oticus (Ramsay Hunt syndrome) | Vesicular eruption affecting the ear; caused by reactivation of the varicellazoster virus |
| Ménière’s disease (Ménière’s syndrome, endolymphatic hydrops) | Recurrent episodes of vertigo, hearing loss, tinnitus, or aural fullness caused by increased volume of endolymph in the semicircular canals |
| Otosclerosis | [ |
| Perilymphatic fistula | Breach between middle and inner ear often caused by trauma or excessive straining |
| Central causes | |
| Cerebellopontine angle tumor | Vestibular schwannoma (i.e., acoustic neuroma) as well as infratentorial ependymoma, brainstem glioma, medulloblastoma, or neurofibromatosis |
| Cerebrovascular disease such as transient ischemic attack or stroke | Arterial occlusion causing cerebral ischemia or infarction, especially if affecting the vertebrobasilar system |
| Migraine | Episodic headaches, usually unilateral, with throbbing accompanied by other symptoms such as nausea, vomiting, photophobia, or phonophobia; may be preceded by aura |
| Multiple sclerosis | Demyelinization of white matter in the central nervous system |
| Other causes | |
| Cervical vertigo | Vertigo triggered by somatosensory input from head and neck movements |
| Drug-induced vertigo | Adverse reaction to medications |
| Psychological | Mood, anxiety, somatization, personality, or alcohol abuse disorders |
* —Acute vestibular neuronitis often is erroneously called acute or viral labyrinthitis.
Because patients with dizziness often have difficulty describing their symptoms, determining the cause can be challenging. An evidence-based approach using knowledge of key historic, physical examination, and radiologic findings for the causes of vertigo can help family physicians establish a diagnosis and consider appropriate treatments in most cases (Figure 1).
Figure 1. Diagnosing Vertigo
Algorithm for an initial approach for diagnosing the cause of vertigo. (MRI = magnetic resonance imaging.)
History
History alone reveals the diagnosis in roughly three out of four patients complaining of dizziness, although the proportion in patients specifically complaining of vertigo is unknown.10 When collecting a patient’s history, the physician first must determine whether the patient truly has vertigo versus another type of dizziness. This can be done by asking, “When you have dizzy spells, do you feel light-headed or do you see the world spin around you?” An affirmative answer to the latter part of this question has been shown to accurately detect patients with true vertigo.11
PERIPHERAL OR CENTRAL CAUSE OF VERTIGO
The next task is to determine whether the patient has a peripheral or central cause of vertigo. Key information from the history that can be used to make this distinction includes the timing and duration of the vertigo (Table 23,6,12); what provokes or aggravates it (Table 31,3,5,12,13); and whether any associated symptoms exist, especially neurologic symptoms and hearing loss (Tables 41,6,12–14 and 59,12,13).10 Characteristics distinguishing peripheral and central causes of vertigo are listed in Table 6.14,15 Rotatory illusions are highly associated with peripheral vestibular disorders, especially when nausea or vomiting accompanies the vertigo.1 Nystagmus in peripheral vertigo usually is horizontal and rotational, lessens or disappears when the patient focuses the gaze, and usually is triggered by some provoking factor. In central vertigo, nystagmus is purely horizontal, vertical, or rotational; does not lessen when the patient focuses the gaze; and persists for a longer period.14 The duration of each episode also has significant diagnostic value; generally, the longer symptoms last, the greater the likelihood that there is a central cause of vertigo.3 In one study,16 the presence of vertigo upon awakening in the morning was suggestive of peripheral vestibular disorders. Peripheral vertigo generally has a more sudden onset than vertigo of central nervous system origin, except for acute cerebrovascular events.3
TABLE 2 Typical Duration of Symptoms for Different Causes of Vertigo
| Duration of episode | Suggested diagnosis |
|---|---|
| A few seconds | Peripheral cause: unilateral loss of vestibular function; late stages of acute vestibular neuronitis; late stages of Ménière’s disease |
| Several seconds to a few minutes | Benign paroxysmal positional vertigo; perilymphatic fistula |
| Several minutes to one hour | Posterior transient ischemic attack; perilymphatic fistula |
| Hours | Ménière’s disease; perilymphatic fistula from trauma or surgery; migraine; acoustic neuroma |
| Days | Early acute vestibular neuronitis*; stroke; migraine; multiple sclerosis |
| Weeks | Psychogenic (constant vertigo lasting weeks without improvement) |
*—Vertigo with early acute vestibular neuritis can last as briefly as two days or as long as one week or more.
TABLE 3 Provoking Factors for Different Causes of Vertigo
| Provoking factor | Suggested diagnosis |
|---|---|
| Changes in head position | Acute labyrinthitis; benign positional paroxysmal vertigo; cerebellopontine angle tumor; multiple sclerosis; perilymphatic fistula |
| Spontaneous episodes (i.e., no consistent provoking factors) | Acute vestibular neuronitis; cerebrovascular disease (stroke or transient ischemic attack); Ménière’s disease; migraine; multiple sclerosis |
| Recent upper respiratory viral illness | Acute vestibular neuronitis |
| Stress | Psychiatric or psychological causes; migraine |
| Immunosuppression (e.g., immunosuppressive medications, advanced age, stress) | Herpes zoster oticus |
| Changes in ear pressure, head trauma, excessive straining, loud noises | Perilymphatic fistula |
TABLE 4 Associated Symptoms for Different Causes of Vertigo
| Symptom | Suggested diagnosis |
|---|---|
| Aural fullness | Acoustic neuroma; Ménière’s disease |
| Ear or mastoid pain | Acoustic neuroma; acute middle ear disease (e.g., otitis media, herpes zoster oticus) |
| Facial weakness | Acoustic neuroma; herpes zoster oticus |
| Focal neurologic findings | Cerebellopontine angle tumor; cerebrovascular disease; multiple sclerosis (especially findings not explained by single neurologic lesion) |
| Headache | Acoustic neuroma; migraine |
| Hearing loss | Ménière’s disease; perilymphatic fistula; acoustic neuroma; cholesteatoma; otosclerosis; transient ischemic attack or stroke involving anterior inferior cerebellar artery; herpes zoster oticus |
| Imbalance | Acute vestibular neuronitis (usually moderate); cerebellopontine angle tumor (usually severe) |
| Nystagmus | Peripheral or central vertigo |
| Phonophobia, photophobia | Migraine |
| Tinnitus | Acute labyrinthitis; acoustic neuroma; Ménière’s disease |
TABLE 5 Causes of Vertigo Associated with Hearing Loss
| Diagnosis | Characteristics of hearing loss |
|---|---|
| Acoustic neuroma | Progressive, unilateral, sensorineural |
| Cholesteatoma | Progressive, unilateral, conductive |
| Herpes zoster oticus (i.e., Ramsay Hunt syndrome) | Subacute to acute onset, unilateral |
| Ménière’s disease | Sensorineural, initially fluctuating, initially affecting lower frequencies; later in course: progressive, affecting higher frequencies |
| Otosclerosis | Progressive, conductive |
| Perilymphatic fistula | Progressive, unilateral |
| Transient ischemic attack or stroke involving anterior inferior cerebellar artery or internal auditory artery | Sudden onset, unilateral |
TABLE 6 Distinguishing Characteristics of Peripheral vs. Central Causes of Vertigo
| Feature | Peripheral vertigo | Central vertigo |
|---|---|---|
| Nystagmus | Combined horizontal and torsional; inhibited by fixation of eyes onto object; fades after a few days; does not change direction with gaze to either side | Purely vertical, horizontal, or torsional; not inhibited by fixation of eyes onto object; may last weeks to months; may change direction with gaze towards fast phase of nystagmus |
| Imbalance | Mild to moderate; able to walk | Severe; unable to stand still or walk |
| Nausea, vomiting | May be severe | Varies |
| Hearing loss, tinnitus | Common | Rare |
| Nonauditory neurologic symptoms | Rare | Common |
| Latency following provocative diagnostic maneuver | Longer (up to 20 seconds) | Shorter (up to 5 seconds) |
SEVERITY
Knowing the severity of vertigo over time also is helpful. For example, in acute vestibular neuronitis, initial symptoms typically are severe but lessen over the next few days. In Ménière’s disease, attacks of vertigo initially increase in severity, then lessen in severity later on. Patients complaining of constant vertigo lasting for weeks may have a psychological cause for their symptoms.
PROVOKING FACTORS
Provoking factors and circumstances around the onset of vertigo may prove useful in narrowing the differential diagnosis to a peripheral vestibular condition. If symptoms occur only with positional changes, such as turning over in bed,17 bending over at the waist and then straightening up, or hyperextending the neck, BPPV is the most likely cause.1 A recent viral upper respiratory infection may precede acute vestibular neuronitis or acute labyrinthitis. Factors that provoke migraine headaches can cause vertigo if the patient experiences this as a symptom associated with migraine.
Vertigo can be caused by perilymphatic fistula (i.e., breach between the inner ear and middle ear).18 Perilymphatic fistula may be caused by trauma from a direct blow, or from activities such as scuba diving (from barotrauma) and heavy weight bearing or excessive straining with bowel movements.3,12 Sneezing or movements that place the affected ear downward also can provoke vertigo in patients with perilymphatic fistulas.19
The presence of Tullio’s phenomenon (i.e., nystagmus and vertigo caused by loud noises or sounds at a particular frequency) suggests a peripheral cause for vertigo.12
Significant psychosocial stress can cause patients to complain of vertigo. Asking about psychological stressors or psychiatric history may be important, especially in patients whose history does not necessarily fit the usual presentation of physical causes of vertigo. For example, a history of anxiety or panic attacks associated with vertigo may point to hyperventilation as a cause.12
ASSOCIATED SYMPTOMS
Hearing loss, pain, nausea, vomiting, or neurologic symptoms can help differentiate the cause of vertigo. Most causes of vertigo with hearing loss are peripheral, the main exception being a cerebrovascular event involving the internal auditory artery or anterior inferior cerebellar artery. Pain accompanying vertigo may occur with acute middle ear disease, invasive disease of the temporal bone, or meningeal irritation.12 Vertigo often is associated with nausea or vomiting in acute vestibular neuronitis and in severe episodes of Ménière’s disease and BPPV.1,20 In central causes of vertigo, nausea and vomiting tend to be less severe.14 Neurologic symptoms such as weakness, dysarthria, vision or hearing changes, paresthesia, altered level of consciousness, ataxia, or other changes in sensory and motor function favor the presence of a central cause of vertigo such as cerebrovascular disease, neoplasm, or multiple sclerosis. Patients with migrainous vertigo may experience other symptoms related to the migraine, including a typical headache (often throbbing, unilateral, sometimes preceded by an aura), nausea, vomiting, photophobia, and phonophobia. Twenty-one to 35 percent of patients with migraine suffer vertigo.21
MEDICAL HISTORY
Other important clues to the diagnosis of vertigo may come from the patient’s medical history, including medications, trauma, or exposure to toxins.18 Age is associated with some underlying conditions that can cause vertigo. For example, older patients, especially those with diabetes or hypertension, are at higher risk of cerebrovascular causes of vertigo.12 Patients should be asked about family history including hereditary conditions such as migraine and risk factors for cerebrovascular disease.
Physical Examination
Physicians should pay particular attention to physical findings of the neurologic, head and neck, and cardiovascular systems.
NEUROLOGIC EXAMINATION
The cranial nerves should be examined for signs of palsies, sensorineural hearing loss, and nystagmus. Vertical nystagmus is 80 percent sensitive for vestibular nuclear or cerebellar vermis lesions.2 Spontaneous horizontal nystagmus with or without rotatory nystagmus is consistent with acute vestibular neuronitis. Patients with peripheral vertigo have impaired balance but are still able to walk, whereas patients with central vertigo have more severe instability and often cannot walk or even stand without falling.14 Although Romberg’s sign is consistent with a vestibular or proprioceptive problem, it is not particularly useful in the diagnosis of vertigo. In one study,22 it was only 19 percent sensitive for peripheral vestibular disorders and did not correlate with more serious causes of dizziness (not limited to vertigo) such as drug-related dizziness, seizure, arrhythmia, or cerebrovascular events.
The Dix-Hallpike maneuver (Figure 2)1,3,19 may be the most helpful test to perform on patients with vertigo. It has a positive predictive value of 83 percent and a negative predictive value of 52 percent for the diagnosis of BPPV.7,10 After the initial test, the intensity of induced symptoms typically wanes with repeated maneuvers in peripheral vertigo but does so less often in central vertigo.15 The combination of a positive Dix-Hallpike maneuver and a history of vertigo or vomiting suggests a peripheral vestibular disorder.22 If the maneuver provokes purely vertical (usually downbeat) or torsional nystagmus without a latent period of at least a few seconds, and does not wane with repeated maneuvers, this suggests a central cause for vertigo such as a posterior fossa tumor or hemorrhage.14,15
Figure 2.
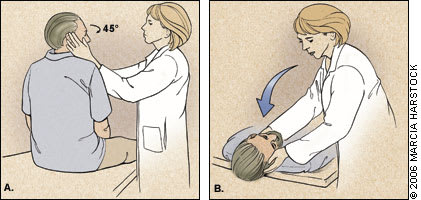
ILLUSTRATION BY MARCIA HARTSOCK
To perform the Dix-Hallpike maneuver, the patient initially sits upright. The examiner should warn the patient that the maneuver may provoke vertigo. The examiner turns the patient’s head 30 to 45 degrees to the side being tested (A). The patient keeps his or her eyes open and focused on the examiner’s eyes or forehead. Then, as the examiner supports the patient’s head, the patient quickly lies supine (within two seconds), allowing the neck to hyperextend slightly and hang off the edge of the examining table 20 to 30 degrees past horizontal (B). After a two- to 20-second latent period, the onset of torsional upbeat or horizontal nystagmus denotes a positive test for benign paroxysmal positional vertigo. The episode can last 20 to 40 seconds. Nystagmus changes direction when the patient sits upright again.
Information from references 1,3, and 19.
Hyperventilation for 30 seconds may assist in ruling out psychogenic causes of vertigo associated with hyperventilation syndrome.22 It rarely can cause true vertigo in patients with perilymphatic fistulas or acoustic neuromas.12
HEAD AND NECK EXAMINATION
The tympanic membranes should be examined for vesicles (i.e., herpes zoster oticus [Ramsay Hunt syndrome]) or cholesteatoma. Hennebert’s sign (i.e., vertigo or nystagmus caused by pushing on the tragus and external auditory meatus of the affected side) indicates the presence of a perilymphatic fistula.12 Pneumatic otoscopy may cause similar findings.3 The Valsalva maneuver (i.e., forced exhalation with nose plugged and mouth closed to increase pressure against the eustachian tube and inner ear) may cause vertigo in patients with perilymphatic fistulae12 or anterior semicircular canal dehiscence12,23; its clinical diagnostic value, however, is limited.22
CARDIOVASCULAR EXAMINATION
Orthostatic changes in systolic blood pressure (e.g., a drop of 20 mm Hg or more) and pulse (e.g., increase of 10 beats per minute) in patients with vertigo upon standing may identify problems with dehydration or autonomic dysfunction.10 Carotid sinus stimulation should not be performed; it has been shown to be not useful diagnostically22 and potentially is dangerous.
Laboratory Evaluation
Laboratory tests such as electrolytes, glucose, blood counts, and thyroid function tests identify the etiology of vertigo in fewer than 1 percent of patients with dizziness.10 They may be appropriate when patients with vertigo exhibit signs or symptoms that suggest the presence of other causative conditions. Audiometry helps establish the diagnosis of Ménière’s disease.20
Radiologic Studies
Physicians should consider neuroimaging studies in patients with vertigo who have neurologic signs and symptoms, risk factors for cerebrovascular disease, or progressive unilateral hearing loss.19 In one study,24 40 percent of patients with dizziness and neurologic signs had relevant abnormalities suggesting central nervous system lesions on magnetic resonance imaging of the head. In patients with isolated vertigo who also were at risk for cerebrovascular disease, 25 percent had caudal cerebellar infarcts.25 In general, magnetic resonance imaging is more appropriate than computed tomography for diagnosing vertigo because of its superiority in visualizing the posterior fossa, where most central nervous system disease that causes vertigo is found.26Magnetic resonance or conventional angiography of the posterior fossa vasculature may be useful in diagnosing vascular causes of vertigo such as vertebrobasilar insufficiency, thrombosis of the labyrinthine artery, anterior or posterior inferior cerebellar artery insufficiency, and subclavian steal syndrome.26
Neuroimaging studies can be used to rule out extensive bacterial infections, neoplasms, or developmental abnormalities if other symptoms suggest one of those diagnoses.26,27 However, they are not indicated in patients who have BPPV,26 usually are not necessary to diagnose acute vestibular neuronitis or Ménière’s disease, and are poor routine screening tests for cerebellopontine angle tumors causing vertigo.27
Conventional radiographs or cross-sectional imaging procedures may aid in the diagnosis of cervical vertigo (i.e., vertigo triggered by somatosensory input from head and neck movements) in patients with a history suggestive of this diagnosis26; however, the existence of this disorder remains controversial, and most patients in whom this diagnosis is considered should have other, more well-established conditions investigated.4
Referral
Not all patients with vertigo need to be referred to a subspecialist. Family physicians should consider referral to the appropriate subspecialist (e.g., otolaryngologist, head and neck surgeon, neurologist, neurosurgeon) if the diagnosis of vertigo is unclear or if the patient has a medical problem requiring further subspecialty care.
