
Am Fam Physician. 2007;75(11):1705-1706
Author disclosure: Nothing to disclose.
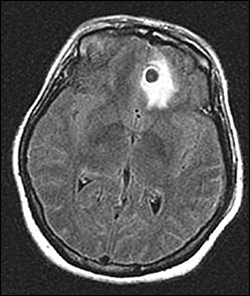
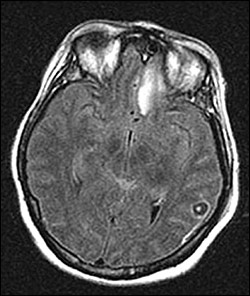
A 35-year-old woman presented to the emergency department in status epilepticus with new-onset seizures. She was immediately intubated for airway protection. Her temperature was 98.4° F (36.9° C); respiratory rate, 22 breaths per minute; pulse, 102 beats per minute; and blood pressure, 127/82 mm Hg. Results of her physical examination were otherwise unremarkable. Her white blood cell count was 17,200 per mm3 (17.2 × 109 per L) with normal differential. Electrolyte, glucose, creatinine, liver enzyme, and hemoglobin levels were normal. Serum pregnancy test and toxicology screens were negative. Computed tomography (CT) without contrast of her head showed a 1.2-cm, well-defined hypodensity with surrounding edema in the left frontal lobe and 1.0-cm hypodensities in the left parietal and right frontoparietal lobes. Magnetic resonance imaging (MRI) of the brain was then performed (Figures 1 and 2).
Question
Discussion
The answer is D: neurocysticercosis. The MRI images show ring-enhancing cystic lesions in the left frontal and parietal lobes, each containing a small mural nodule on a pedicle representing the scolex of the tapeworm, Taenia solium. A large area of edema is visible around one of the degenerating cysts (Figure 1). These findings are pathognomonic for neurocysticercosis, a common parasitic CNS disease.1
Two distinct clinical entities result from T. solium infection. Taeniasis, or adult tapeworm intestinal infection, is caused by ingestion of raw or undercooked pork containing larval cysts (i.e., cysticerci). These develop into adult tapeworms in the small intestine and release proglottids containing eggs that are then passed in feces. Cysticercosis occurs when a host ingests food or water contaminated with T. solium eggs or by autoinoculation in persons harboring the adult tapeworm. Once ingested, the eggs hatch into larvae that burrow through the wall of the small intestine, disseminating hematogenously to other tissues. There they develop into encapsulated, fluid-filled larval cysts.
The clinical manifestations of neurocysticercosis depend on the number and location of the cysts and the host's immune response to the parasite. Symptoms occur because of mass effect or result from an intense local inflammatory reaction when cysticerci degenerate.2 Patients may have seizures, headache, nausea, vomiting, behavior disturbances, and memory impairment. Focal neurologic deficits, hydrocephalus, encephalitis, cerebral edema, fever, and meningism also may occur. Inflammation around degenerating cysticerci in the eye can cause uveitis, retinitis, retinal detachment, or vasculitis. Ocular involvement must be excluded in all patients before initiating therapy because therapy causes cyst degeneration, possibly resulting in visual impairment.
Diagnosis of neurocysticercosis is made by identifying a cystic lesion with a mural nodule on CT or MRI, by identifying the parasite histologically on a biopsy, or by directly visualizing subretinal parasites on funduscopic examination.3 The presence of cysticercal antigens in the cerebrospinal fluid (CSF) or antibodies in serum or CSF may support the diagnosis.3 Stool testing may be negative and is not one of the diagnostic criteria.1
Treatment is based on the presenting symptoms and size, viability, and location of the cysts. Anticonvulsants are used for seizures, and albendazole (Albenza) or praziquantel (Biltricide) may be given with corticosteroids to hasten cyst resolution and reduce inf lammation. Surgery is used for hydrocephalus and ophthalmic cysticercosis.3
Radiographically, cerebral abscesses and toxoplasmosis appear as single or multiple ring-enhancing circumscribed lesions with surrounding vasogenic edema. Brain abscesses are often at the gray-white junction or in the middle cerebral artery distribution.4 Toxoplasmosis has a predilection for the basal ganglia and corticomedullary junction and occurs primarily in immunocompromised persons with immature or impaired T-cell immunity.5 Primary CNS lymphoma appears as a single or multifocal lesion localized to the periventricular white matter or corpus callosum and appears isodense to hyperdense on CT scan but isointense to hypointense on MRI.6 Brain metastases most often appear at the gray-white junction or watershed zones as multiple, homogenously enhanced or ring-enhancing lesions with a large amount of surrounding vasogenic edema.7
| Condition | Characteristics |
|---|---|
| Cerebral abscesses | Single or multiple ring-enhancing lesions; often at gray-white junction or middle cerebral artery distribution when associated with bacteremia |
| Cerebral metastases | Multiple homogenously enhanced or ring-enhancing lesions at gray-white junction or watershed zones; associated vasogenic edema |
| Cerebral toxoplasmosis | Single or multiple ring-enhancing lesions in basal ganglia or corticomedullary junction; immunocompromise; positive Toxoplasma titers |
| Neurocysticercosis | Ring-enhancing lesion, mural nodule on pedicle |
| Primary central nervous system lymphoma | Single or multifocal lesions localized to periventricular white matter or corpus callosum; ring enhancement uncommon; may have necrosis, calcification, and cystic appearance |