Cysticercosis (i.e., tapeworm infection) is an increasingly common medical problem in the United States, especially in the Southwest and other areas of heavy emigration from endemic areas or in populations with significant travel to these areas. The larval stage of the pork tapeworm, Taenia solium, causes the clinical syndrome of cysticercosis, with humans as dead-end hosts after ingestion of T. solium eggs. Its clinical effects vary depending on site of larval lodging, larval burden, and host reaction. These effects include seizures, headaches, focal neurologic symptoms, visual disturbances, and localized skeletal muscle nodules and pain. Cysticercosis should be considered in any patient from an endemic area presenting with these symptoms. Treatment varies with the clinical presentation. Parenchymal neurocysticercosis generally is treated with albendazole in conjunction with steroids to limit edema and with antiepileptic medications for seizure control. Ocular and extraocular muscle cysticercosis generally requires surgical intervention. Skeletal muscle cysts are surgically removed only if painful. Because cysts can lodge in multiple locations, all patients with cysticercosis should have an ophthalmologic examination to rule out ocular involvement, and all patients with extraneurologic cysticercosis should have computed tomography or magnetic resonance imaging of the brain to rule out neurocysticercosis.
Cysticercosis (i.e., tapeworm infection) is the most common parasitic disease worldwide, with an estimated prevalence greater than 50 million persons infected.1–3 It is endemic in Mexico, Central and South America, and parts of Africa, Asia, and India.4,5 Neurocysticercosis, the neurologic manifestation of cysticercosis, is the most prevalent infection of the brain worldwide,6–8 and more than 1,000 new cases are diagnosed in the United States each year.2,9 Neurocysticercosis is one of the leading causes of adult-onset seizures worldwide10–13 and was found to be the etiologic agent in 10 percent of new-onset seizure patients in one Los Angeles, Calif., emergency department.13,14
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendation | Evidence rating | References | Comments |
|---|---|---|---|
| Dilated eye examination is warranted for detection of ophthalmic lesions, and treatment is generally surgical. | C | 16 | Vision loss is a possible risk of undetected ocular cysts treated with antihelminthic medications. |
| Nonenhancing and enhancing cystic parenchymal neurocysticercosis should be treated with seven to 14 days of albendazole (Albenza). | B | 10, 13, 27, 28 | Treatment seems to decrease rate of seizures, even with degenerating cysts. |
| Calcified or heavy-infection (50 or more cysts) neurocysticercosis does not warrant antihelminthic therapy. | C | 13 | Calcified cysts are already dead, and massive infections could create uncontrollable cerebral edema if treated with antihelminthic medications. |
| For neurocysticercosis with seizures, steroids should be used concomitantly with antihelminthic therapy. | B | 2, 28 | Steroids decrease perilesional edema and seizures. |
| Carbamazepine (Tegretol) is effective in the symptomatic treatment of seizures in neurocysticercosis. | B | 2, 4, 7, 9 | Antiepileptics decrease the rate of seizures. |
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, see page 14 or https://www.aafp.org/afpsort.xml.
Epidemiology
The life cycle of the pork tapeworm, Taenia solium, begins at the larval stage in pigs (Figure 1). Human tapeworm infection occurs when T. solium cysts are ingested from undercooked pork. The larvae attach to the human gut and grow into adult tapeworms. The adult tapeworm then sheds proglottids (i.e., bundles of tapeworm eggs) into human feces that can contaminate the pig food supply. Eggs ingested by pigs develop into the larval stage, travel through the intestinal wall, enter the bloodstream, lodge in various pig tissues, and develop into cysts.4,7,15
Figure 1.
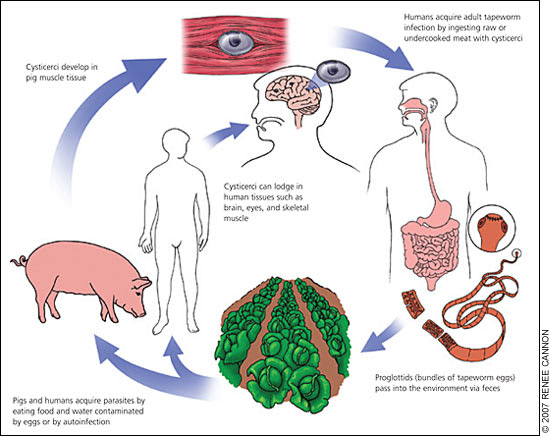
Life cycle of Taenia solium larvae.
When humans ingest eggs, through fecal-oral transmission or possibly through auto-infection, they become dead-end hosts of the larval stage of the parasite and develop cysticercosis similar to pigs.1,2,16 Fecal-oral contamination usually occurs via infected food handlers who do not appropriately wash their hands before working, or by fruit and vegetables fertilized with contaminated human waste. Autoinfection involves the retrograde transmission of proglottids from the intestines into the stomach with subsequent release of T. solium eggs into the human gut. Ingestion of encysted pork does not directly cause cysticercosis; rather, it produces an intestinal infection of the adult tapeworm and a carrier state for the T. solium eggs that, when ingested by humans, produce the clinical syndrome of cysticercosis. Even populations who do not eat pork (e.g., vegetarians) can develop cysticercosis.2,7
Clinical Features
The clinical features of cysticercosis depend on the location of the cysts and overall cyst burden.2–4 Cysts can lodge in the brain and spinal column, eyes, skeletal muscle, and subcutaneous tissues.7,9,16 Brain and eye cysts cause the most morbidity, with the brain being the most common location for cysts (60 to 90 percent of all cases) and the eye being the least common (1 to 3 percent).2,7
The total number of cysts can range from a solitary lesion to several hundred.5,8 The initial host reaction is often avoided through the encystment of the larvae, a process that includes enlisting defense mechanisms against destruction by the host.1,4 This phase may last for years and is often clinically silent except when cyst location or size causes signs or symptoms. Most cysts are unable to maintain these protective barriers indefinitely, and degenerating cysts release larval antigens that produce a vigorous host response and cause the clinically apparent syndrome through inflammatory mediators and surrounding edema.2,4,15 After the acute inflammatory phase, the encysted larvae generally die, complete the degeneration phase, and often calcify.13,15 Calcified cysts can produce symptoms by way of less clearly defined mechanisms.8,15
Parenchymal neurocysticercosis, the infection of brain parenchyma, is a common cause of focal and generalized seizures, but it less commonly presents as headache, parkinsonism, or other neurologic abnormality.5,17,18 Heavy cyst burden in neural tissue can cause encephalopathy with fever, headache, nausea and vomiting, altered mental status, and seizures. Cysts also can occur in the subarachnoid or ventricular spaces, sometimes growing large enough to cause meningeal signs and symptoms, obstructive hydrocephalus, or cranial nerve palsies caused by nerve entrapment.7,8,19 Less commonly, cysts located in the spinal column can cause radicular pain or paresthesias indistinguishable from other spinal pathologies.1,2,7,9
Cysticercosis also can occur at sites distant from the central nervous system. Ocular manifestations can be found in the subretinal space or vitreous humor and can threaten vision through inflammation of degenerating cysts or through retinal detachment.1,7,9,16 Cysts can settle into extraocular muscles, producing limitations on the range of eye movements that can mimic cranial nerve palsies.1,7,8,20 Skeletal muscle or subcutaneous cysticercosis can cause localized pain and nodules.7
Diagnosis
Diagnosis of cysticercosis in a nonendemic region such as the United States requires a high index of suspicion in the appropriate clinical setting. Travel to or emigration from an endemic area should raise suspicion, but exact timing may not be helpful because of T. solium's propensity for a prolonged and variable period of clinically silent infection.7,13 Specific criteria (Table 121 ) have been proposed for the diagnosis of cysticercosis.22
Table 1 Criteria for Diagnosis of Cysticercosis
| Level of criteria | Findings |
|---|---|
| Absolute | Pathologic demonstration of the parasite; cystic lesion with scolex found on computed tomography scan or magnetic resonance imaging; direct visualization on funduscopy |
| Major | Lesions highly suggestive of neurocysticercosis on neuroimaging; positive serum enzyme-linked immunoblot for cysticercal antibodies; resolution of cysts after antiparasitic therapy; spontaneous resolution of a small solitary enhancing lesion |
| Minor | Lesions compatible with neurocysticercosis on neuroimaging; clinical manifestations suggestive of neurocysticercosis; positive cerebrospinal fluid enzyme-linked immunosorbent assay for anticysticercal antibodies or cysticercal antigens; cysticercosis outside of the central nervous system |
| Epidemiologic | Household contact with Taenia solium infection; persons coming from or living in an area where cysticercosis is endemic; history of frequent travel to disease-endemic areas* |
note:Definitive diagnosis is one absolute criterion or two major criteria plus one minor criterion and one epidemiologic criterion; probable diagnosis is one major criterion plus two minor criteria, or one major criterion plus one minor criterion and one epidemiologic criterion, or one minor criterion plus three epidemiologic criteria.
*— Cysticercosis is endemic in Mexico, Central and South America, the Indian subcontinent, sub-Saharan Africa, and China.
Adapted with permission from Del Brutto OH, Wadia NH, Dumas M, Cruz M, Tsang VC, Schantz PM. Proposal of diagnostic criteria for human cysticercosis and neurocysticercosis. J Neurol Sci 1996;142:2.
After the history and physical examination, a computed tomography (CT) scan with or without intravenous contrast media is generally the first step in the diagnosis of suspected neurocysticercosis (Figure 2).1,4 Brain CT with or without contrast media demonstrating a solitary contrast-enhancing lesion less than 20 mm in diameter and producing no midline shift is highly sensitive for neurocysticercosis.23 The scolex, or sucking parts of the larva, also may be visible; this is pathognomonic for neurocysticercosis.
Figure 2.

Computed tomography scan of a solitary parenchymal neurocysticercosis cyst (arrow).
Number, size, and location of cysts, as well as staging of the cysts' life cycle, can be determined and may impact treatment decisions. Cystic, nonenhancing lesions point to viable, nondegenerating cysts. Cystic, enhancing lesions indicate degenerating cysts with some surrounding inflammation. Finally, calcified cysts are evidence of old cysts that have already died.13,15 Care must be taken to consider other causes (e.g., tuberculosis, other parasitic diseases, metastatic or primary brain cancer, brain abscess) when a lesion is found on CT.9,23
Magnetic resonance imaging also is a useful tool for diagnosing neurocysticercosis (Figure 3) and may be better than CT at detecting spinal, brainstem, or intraventricular lesions.4,9,17 Its use should be considered when CT is non-diagnostic.4 CT and ultrasonography are sensitive for the detection of ocular or extraocular muscle cysticercosis.20,24
Figure 3.
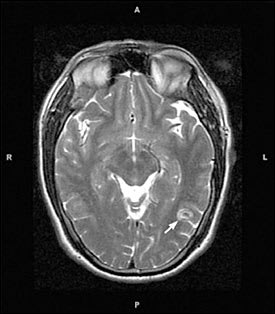
Magnetic resonance image of a solitary parenchymal neurocysticercosis cyst (arrow).
Serology is available for detection of cysticercal antibodies through an enzyme-linked immunoblot assay or enzyme-linked immunosorbent assay of the serum or cerebrospinal fluid; these have a sensitivity of 65 to 98 percent and a specificity of 67 to 100 percent, depending on the specific test used, cyst burden, location, and phase of the infection.2,7,22,25 When available, enzyme-linked immunoblot assay of the serum has the greatest sensitivity and specificity and as major diagnostic criteria is the test of choice. Enzyme-linked immunosorbent assay of the cerebral spinal fluid is less sensitive and specific but still meets minor diagnostic criteria.7 Antibodies can persist after cysts die; therefore, serology should always be reviewed in light of the presenting clinical picture and imaging studies obtained.7
Biopsy of the brain, skin, or muscle can provide a definitive diagnosis in an otherwise ambiguous clinical situation and may be the diagnostic method of choice for ocular, extraocular muscle, or painful muscular/subcutaneous cysts.2,7,16 Biopsy of lesions distal to the central nervous system provides further evidence of neurocysticercosis when brain imaging is nondiagnostic and brain biopsy is not desired or feasible.22
Dilated ophthalmologic examination is sensitive for the detection of ocular cysts and is necessary for anyone diagnosed with cysticercosis to rule out ocular involvement. Likewise, diagnosis of any nonneurologic cysticercosis (e.g., in the muscle or skin) warrants a history, physical examination, and imaging studies to rule out neurologic involvement.
Treatment
Diagnosis of cysticercosis does not automatically lead to therapy with a single, universally applied treatment regimen. The treatment decision-making process can be complex, and therapeutic options include medications, surgery, or watchful waiting. The treatment decision must take into account multiple factors, including symptoms and the location, number, stage, and size of cysts. Discussion of treatment options is difficult because of the number of caveats that must be considered, which also makes evidence-based recommendations difficult to develop except in the most common clinical scenarios (i.e., single or multiple parenchymal neurocysticercosis cysts). Consultation with an infectious diseases subspecialist is almost always warranted, especially with sub-arachnoid or intraventricular disease and with massive cyst infection (i.e., 50 or more cysts).
Soft tissue and muscular cysticercosis treatment depends on location of the cysts. Isolated skeletal muscle or subcutaneous cysticercosis requires no specific treatment unless it is painful, and then simple excision may be required. Small case series suggest that antiparasitic therapy with albendazole (Albenza) or praziquantel (Biltricide), generally in conjunction with steroids, is effective in the treatment of extraocular muscle involvement.20,24 However, surgical excision is an option, and an ophthalmologic consultation is warranted.
Surgical removal of the cyst is considered the treatment of choice for intraocular cysts, although evidence mainly comes from case reports and small case series demonstrating superiority of surgery over antihelminthic therapy.16 It has been suggested that antihelminthic medication be avoided because of the inflammation that may be induced and the resulting threat to vision.16
Treatment of subarachnoid and intraventricular neurocysticercosis is somewhat more complicated and risky. A recent trial suggests that high-dose albendazole (30 mg per kg per day) increases clearance of subarachnoid and intraventricular cysts compared with usual dosing (15 mg per kg per day).26 Intraventricular cysts have generally been excised, but a small case series describes the use of albendazole and steroids as a successful alternative to surgery.6 The risk of inflammation caused by treatment, and its attendant morbidity, would make neurosurgical and infectious diseases consultation advisable before initiation of therapy. Regardless of the treatments chosen, a ventriculoperitoneal shunt should be placed in all patients with evidence of significant obstructive hydrocephalus.1,3
Treatment of parenchymal neurocysticercosis is the most well-studied clinical scenario among all types of cysticercosis, but this treatment has remained controversial because of the heterogeneity of the disease, the presumed natural history of nearly universal spontaneous degradation of the cysts, and overall poor quality of studies of the treatment. Results of studies related to parenchymal neurocysticercosis are inconsistent; however, a recent meta-analysis of the highest-quality studies demonstrates reduced seizures and increased resolution of lesions on imaging for nonenhancing and enhancing lesions in the brain parenchyma with cysticidal drug therapy.10
If antiparasitic therapy is used for parenchymal neurocysticercosis, a seven-day course of albendazole seems to be equally effective as a 14- or 28-day course and is probably more effective than praziquantel.10,13,27,28 Infections with more than a few lesions may require longer courses of antiparasitic medication.10 Massive infections generally are not treated with antihelminthic medications because of the risk of an overwhelming inflammatory response from degenerating cysts.13 Watchful waiting is indicated for calcified cysts because they are already dead.
Using steroids to treat cerebral edema, usually in the form of dexamethasone or prednisolone, has demonstrated a more consistent therapeutic benefit for neurocysticercosis patients with seizures.2,28 Steroids should always be used before or on initiation of antihelminthic medications to blunt the inflammatory reaction that may result in increased seizures.28 Mannitol (Osmitrol) also is an option to reduce cerebral edema as an adjunct to steroids.1
Antiepileptic medications in standard dosages, most commonly phenytoin (Dilantin) and carbamazepine (Tegretol), are key for symptom control.2,4,7,9 Length of use is not well defined, but the antiepileptic should probably be continued for at least one year and then tapered or continued based on symptoms.9 Some patients require long-term antiepileptic therapy.
Future Directions
Further study is required to fully clarify the optimal treatment regimens for cysticercosis, even for the most common presentations of the disease. Future strategies may focus on prevention of the spread of T. solium. A report from the Centers for Disease Control and Prevention Working Group on Parasitic Diseases classified cysticercosis as a potentially eradicable disease.29 Efforts may include decreasing pork tapeworm carriers and thus reducing T. solium egg shedding through more intense meat inspection and preparation, eliminating exposure of pigs to human feces, and developing a vaccine against T. solium. Recent studies have demonstrated the potential utility of various vaccines for use in pigs, but widespread use is not yet a reality.30,31
