A four-year-old girl presented with progressive weakness in her right arm and leg, and with bowel incontinence. She had a one-year history of intermittent focal seizures that were not controlled with antiepileptic medication. The initial evaluation of her seizures included an unremarkable computed tomography (CT) scan of her head. However, electroencephalography (EEG) showed diffuse, unihemispheric slowing that lasted for two to three minutes. She did not have a history of meningitis or encephalitis
The patient was afebrile, and skin examination findings were normal. A neurologic examination revealed moderately decreased strength in her right limbs. T1-and T2-weighted magnetic resonance imaging (MRI) of the brain (Figures 1and2) was performed.
Figure 1.
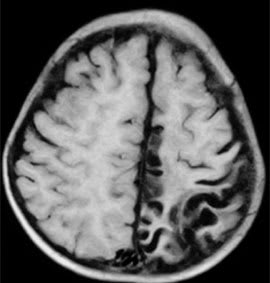
T1-weighted magnetic resonance imaging of the brain.
Figure 2.
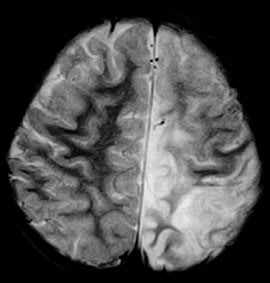
T2-weighted magnetic resonance imaging of the brain.
Question
Based on the patient's history, physical examination, and MRI findings, which one of the following is the most likely diagnosis?
A. Cortical dysplasia.
B. Hemiconvulsion-hemiplegia-epilepsy syndrome.
C. Rasmussen encephalitis.
D. Stroke.
E. Sturge-Weber syndrome.
Discussion
The answer is C: Rasmussen encephalitis. The T1-weighted image of the brain shows left hemiatrophy that is more severe in the occipital and parietal lobes (Figure 1). The T2-weighted image (Figure 2) shows an abnormally hyper-intense signal in the gray and white matter of the left posterior frontal, parietal, and occipital lobes. The MRI findings combined with the patient history of refractory focal seizures and progressive motor weakness are consistent with Rasmussen encephalitis (i.e., Rasmussen syndrome). Hemispherectomy performed five months after presentation confirmed it.
Rasmussen encephalitis is a chronic, likely autoimmune, inflammatory disease, usually affecting one hemisphere. There is no conclusive explanation for why or how it develops, although a cytotoxic T-cell reaction against neurons has been implicated in its pathogenesis.1,2
Although Rasmussen encephalitis can occur in adulthood, it is most common in childhood; the average age of onset is six years. Three disease stages have been described.3,4 Initially, there may be a rather nonspecific prodromal stage with relatively few seizures and, rarely, mild hemiparesis. The median duration of the prodromal stage is seven months. Following this, all patients enter an acute stage with frequent seizures, usually simple partial motor seizures. Neurologic deterioration manifests as progressive hemiparesis; hemianopsia; cognitive deterioration; and aphasia, if the language-dominant hemisphere is affected. This stage usually lasts four to eight months. In one third of patients, the acute stage is the initial manifestation. Finally, the residual stage includes permanent, stable neurologic deficits. Seizures continue, but are less frequent. Hemiparesis and cognitive status are the most useful markers of disease progression.
Antiepileptic drugs do not control seizures. Steroids and other immunotherapies have also proved ineffective. Surgery is the only method to alter disease progression.2
The diagnosis is based on clinical, EEG, and neuro-imaging findings. Three criteria have been proposed for early diagnosis: refractory focal seizures with a predominant motor component, slow focal activity on EEG contralateral to the motor manifestations, and focal contralateral white matter hyperintensity with insular cortical atrophy on MRI.5 Brain biopsy is reserved for patients with an atypical presentation.6 If biopsy is performed, it will show T-cell–dominated encephalitis with activated microglial cells and reactive astrogliosis.7,8 Positron emission tomography, single-photon emission CT, and magnetic resonance spectroscopy may help confirm the unihemispheric nature of Rasmussen encephalitis, but these tests are not specific for the diagnosis.
Cortical dysplasia usually begins in infancy and is associated with focal cortical thickening rather than atrophy. Hemiconvulsion-hemiplegia-epilepsy syndrome involves atrophy of the entire hemisphere, often following an episode of meningitis or encephalitis. Stroke is usually confined to a particular vascular distribution, often involving watershed areas of major vascular channels. The infarcted cortex has gyral swelling in the acute stage followed by atrophic change. Patients with Sturge-Weber syndrome have a port-wine stain. MRI shows tram-track cortical calcification, focal cerebral atrophy, leptomeningeal venous angiomas, and ipsilateral skull thickening.
Summary Table
| Condition | MRI characteristics |
|---|---|
| Cortical dysplasia | Focal cortical thickening, blurring of gray-white matter junction, hyperintensity of subcortical white matter (T2-weighted) |
| Hemiconvulsion-hemiplegia-epilepsy syndrome | Early findings show involvement of the entire hemisphere, which is indicative of diffuse cytotoxic edema; hemispheric atrophy follows |
| Rasmussen encephalitis | Progressive unihemispheric focal cortical atrophy and hyperintensity (T2-weighted) in gray or white matter |
| Stroke | Acute gyral swelling and hyperintensity (T2-weighted) in the infarcted cortex; atrophic findings follow |
| Sturge-Weber syndrome | Tram-track cortical calcification, focal cerebral atrophy, leptomeningeal venous angiomas, ipsilateral skull thickening |
MRI = magnetic resonance imaging.
