A 42-year-old man presented with sudden-onset chest pain that began the previous day while he ran on a treadmill. The patient felt a sharp pain in the left side of his chest that radiated to his back and worsened with deep inspiration. He also felt a clicking sensation with inspiration. He stopped running when the pain occurred, but did not seek care until the following day. At the time of examination, he was pain-free except with deep inspiration. He denied having a cough, wheezing, fever, recent symptoms of upper respiratory tract infection, shortness of breath, or dyspnea on exertion.
The patient's medical history included spondylosis and degenerative disk disease, and he was taking oxycodone (Oxycontin) and acetaminophen. He was athletic and used chewing tobacco. He had no family history of coronary artery disease.
On physical examination, he appeared to be well, had a temperature of 97.9° F (36.6° C), heart rate of 83 beats per minute, blood pressure of 155/74 mm Hg, respirations of 20 breaths per minute, and oxygen saturation of 99 percent. Cardiovascular auscultation was unremarkable. Auscultation of the lungs was also unremarkable, except for a subtle diminution of breath sounds at the left apex. Palpation of his left fourth and fifth ribs at the costosternal joints produced pain similar to his presenting complaint. He had strong and equal radial pulses. Results of electrocardiography were unremarkable. His posterior-anterior chest radiograph is shown in Figure 1.
Figure 1.

Question
Based on the patient's history, physical examination, and radiographic findings, which one of the following is the most likely diagnosis?
A. Intercostal muscle strain.
B. Pneumothorax.
C. Pulmonary embolism.
D. Stress fracture of the rib.
E. Tietze syndrome.
Discussion
The answer is B: pneumothorax. The incidence of spontaneous pneumothorax is 20,000 per year in the United States.1 Spontaneous pneumothorax may be primary, occuring in patients with no preexisting pulmonary disease; or secondary, occuring with preexisting disease (usually chronic obstructive pulmonary disease). The patient's radiograph confirms the diagnosis, showing displaced visceral pleura between the fourth and fifth ribs, above which there are no pulmonary markings (Figure 2).
Figure 2.
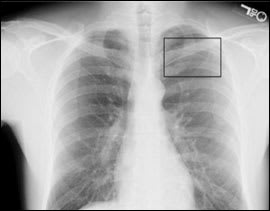
Chest radiograph showing displaced visceral pleura (black box).
Risk factors for primary spontaneous pneumothorax include smoking, ectomorphism, and family history of the condition.1 Symptoms include dyspnea and pleuritic chest pain radiating to the back or scapula. Examination may reveal tachycardia, diminished breath sounds, and diminished chest movement. Some patients have no or few symptoms. Although the patient had no abnormal breath sounds, the clicking may have been from an air leak or movement of the pleura (Hamman sign).2
Treatment is guided by the patient's clinical status and size of the pneumothorax. Unstable patients need immediate needle decompression and chest tube placement. Stable patients with a small pneumothorax (less than 2 to 3 cm) may be treated conservatively; however, a chest tube may be needed if the pneumothorax is larger.1
Definitive treatment is recommended after the second episode of primary spontaneous pneumothorax. Patients who are at a higher risk if the condition recurs (e.g., divers, airplane pilots) should receive definitive treatment after the first episode.1
Intercostal muscle strains are common and often reproducible with palpation or exacerbated by trunk rotation. Reproduction of chest pain by palpation may be misleading because some patients with pain of cardiac etiology report chest wall tenderness.
The clinical presentation of pulmonary embolism is similar to that of pneumothorax. Patients with pulmonary embolism may have identifiable risk factors (e.g., recent trauma, malignancy, prolonged immobilization, clotting disorder). Initial radiography usually is normal.
Stress fractures of the ribs are rare, but may occur in rowers and golfers,3 and in persons with a severe cough.4
Tietze syndrome is a form of costochondritis. The etiology is unknown.5
Summary Table
| Condition | Characteristics | Risk factors |
|---|---|---|
| Intercostal muscle strain | Usually reproducible with palpation or exacerbated by trunk rotation | Physical activity (e.g., in athletes) |
| Primary spontaneous pneumothorax | Pleuritic chest pain with radiation to the back or scapula, dyspnea, diminished breath sounds; patient may have hypoxia, tachycardia, tachypnea, hypotension | Smoking, increased height-to-weight ratio (ectomorphism), family history of spontaneous pneumothorax |
| Pulmonary embolism | Dyspnea, chest pain, hypoxia, tachycardia | Recent trauma or surgery, malignancy, prolonged immobilization, clotting disorder |
| Stress fracture of the rib | Reproducible pain over the affected rib | History of severe cough, participation in sports that require strenuous use of the upper body (e.g., golfing, rowing) |
| Tietze syndrome | Reproducible pain over the costochondral or sternoclavicular joints, with associated swelling | Unknown |
