Almost 160 million persons live in areas of the United States that exceed federal health-based air pollution standards. The two air pollutants that most commonly exceed standards are ozone and particulate matter. Ozone and particulate matter can harm anyone if levels are sufficiently elevated, but health risk from air pollution is greatest among vulnerable populations. Both ozone and particulate matter can cause pulmonary inflammation, decreased lung function, and exacerbation of asthma and chronic obstructive pulmonary disease. Particulate matter is also strongly associated with increased cardiovascular morbidity and mortality. Children, older adults, and other vulnerable persons may be sensitive to lower levels of air pollution. Persons who are aware of local air pollution levels, reported daily by the U.S. Environmental Protection Agency as the Air Quality Index, can take action to reduce exposure. These actions include simple measures to limit exertion and time spent outdoors when air pollution levels are highest, and to reduce the infiltration of outdoor air pollutants into indoor spaces.
Despite steady improvements in air quality in recent decades, 2007 data indicate that more than one half of all persons in the United States live in areas where levels of outdoor air pollution exceed health-based standards.1 Air pollution levels tend to be highest in urban areas, but rural areas may also be affected. The U.S. Environmental Protection Agency (EPA) and other regulatory agencies focus on reducing air pollution at its many sources. Physicians and patients can use the EPA's daily Air Quality Index (AQI) to take action to mitigate related health risks.
Despite the lack of evidence of improvement in outcomes from prospective studies, consensus guidelines recommend that physicians help patients use AQI information to reduce personal exposure to air pollutants and subsequent health effects. Vulnerable patients include children and older adults, as well as persons with asthma, chronic obstructive pulmonary disease (COPD), or heart disease.2 Improvements in air quality have led to measurable improvements in life expectancy in the United States.3 The American Academy of Family Physicians supports continued measures to reduce air pollution because of its adverse health effects.4
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendation | Evidence rating | References |
|---|---|---|
| All persons living in areas in which air pollutants exceed health-based standards should be aware of the AQI. | C | 2 |
| Monitoring of the daily AQI is recommended for at-risk persons, including those with asthma, chronic obstructive pulmonary disease, or heart disease; children; and older adults. | C | 2, 3, 5, 8 |
| Physicians should advise high-risk patients to reduce exposure to outdoor air pollution when levels are high by spending less time outdoors and avoiding prolonged outdoor exertion. | C | 2, 3, 5, 8 |
note: Recommendations based on consensus guidelines.
AQI = Air Quality Index.
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.xml.
Major Air Pollutants: Ozone and Particulate Matter
The federal Clean Air Act requires the EPA to set National Ambient Air Quality Standards (NAAQS) for pollutants to protect the health of all persons in the United States, including vulnerable populations. The EPA standards cover six major air pollutants, also known as “criteria” pollutants: ozone, particulate matter (PM), carbon monoxide, nitrogen oxides (NOx), sulfur dioxide, and lead. This article focuses on ozone and PM, the most widespread and serious threats to health.
More than 1,000 monitoring stations across the United States measure ambient concentrations of criteria air pollutants. Locations that fail to meet one or more standards are designated “nonattainment” areas. Table 1 summarizes the standards, sources of pollutants, at-risk groups, and numbers of persons in the United States living in nonattainment areas for ozone and PM.1,3,5,6 Figure 1 shows current U.S. nonattainment areas for one or more NAAQS.7 Physicians and patients can determine if their local area meets the standards by going to http://airnow.gov. The EPA also provides an online training course, “Ozone and Your Patients' Health,” at http://www.epa.gov/03healthtraining/index.html.
Table 1. Characteristics of Ozone and PM Air Pollution
| Pollutant | NAAQS (averaging time) | Sources | Potential health effects | Susceptible groups | Main regions affected | U.S. population in nonattainment areas† |
|---|---|---|---|---|---|---|
| Ozone | 0.075 ppm (eight-hour) |
|
|
|
| 132 million |
| 0.12 ppm (one-hour*) | ||||||
| PM2.5 | 15.0 mcg per m3 (annual) |
|
|
|
| 88 million |
| 35.0 mcg per m3 (24-hour) | ||||||
| PM10 | 150 mcg per m3 (24-hour) |
|
|
|
| 26 million |
CHF = congestive heart failure; COPD = chronic obstructive pulmonary disease; MI = myocardial infarction; NAAQS = National Ambient Air Quality Standards; NOx= nitrogen oxides; PM = particulate matter; ppm = parts per million; VOC = volatile organic compound.
*— Applies only in limited areas.
†— A nonattainment area is a location that fails to meet one or more NAAQS.
Figure 1. Counties Designated as Nonattainment Areas for Clean Air Act's NAAQS*
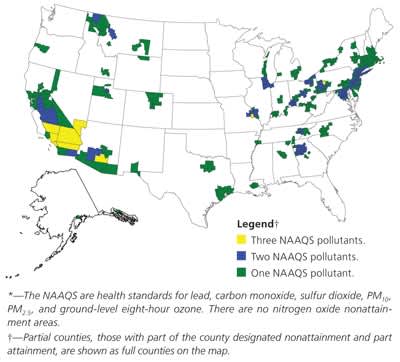
U.S. counties designated as nonattainment areas for failing to meet one or more National Ambient Air Quality Standards (NAAQS). (PM = particulate matter.)
Adapted from U.S. Environmental Protection Agency. Green book. http://www.epa.gov/air/oaqps/greenbk/mapnpoll.html. Accessed October 14, 2009.
The Air Quality Index
Air concentrations of criteria pollutants at most locations show substantial short-term variation, mainly because of changing weather conditions. The EPA offers daily information about air quality, including forecasts, in the form of the AQI. The AQI provides the public with concise information about local air quality, potential health effects, and actions persons can take to protect their health when air pollutants reach unhealthy levels. Pollutant concentrations are reported on a normalized, color-coded scale of 0 to 500 to convey the levels of air pollutant and related health concerns (Table 2).2 The AQI value of the day is the highest individual pollutant AQI value. An AQI value of 100 generally corresponds to the NAAQS for the pollutant. Values greater than 100 are considered unhealthy, first for vulnerable groups and then, as values get higher, for everyone. Values rarely exceed 300 in the United States. The AQI is widely publicized, usually in weather reports, using radio, newspapers, television, the Internet, and many state and local telephone hotlines.
For a given AQI, pollutant-specific cautionary statements identify groups at risk and recommend actions to reduce or avoid exposure to prevent health effects (Table 2).2 The demonstrated health effects of these air pollutants are drawn from a wide range of epidemiologic studies and placebo-controlled exposure studies, and provide a sound basis for recommending risk reduction by avoiding or reducing exposure.5,8–10
Table 2. EPA Cautionary Statements for Ozone and Particle Matter
EPA = U.S. Enviornmental Protection Angency.
Adapted from Environmental Protection Agency. Air Quality Index (AQI): a guide to air quality and your health. 2009. http://airnow.gov/index.cfm?action=aqibasics.aqi. Accessed January 26, 2009.
Reducing Risk from Air Pollution
When ozone concentrations are elevated, patients can reduce their exposure by spending less time outdoors and limiting their level of exertion in outdoor activities. Although outdoor air pollutants infiltrate homes and other buildings, indoor levels are generally lower than outdoor levels. The difference between indoor and outdoor levels varies with the type of pollutant and other factors, such as ventilation rates. Indoor ozone levels are typically 10 to 80 percent of outdoor levels.11 Actions that effectively reduce indoor ozone levels include closing windows and using air conditioning in recirculation mode. Indoor/outdoor ratios of ozone are typically less than 1:10 in buildings with central air conditioning.12 The EPA recommends limiting exertion indoors as well as outdoors when PM is elevated outdoors, because indoor particle levels may be elevated when outdoor levels are high.2 For PM, the relationship between indoor and outdoor levels is also more complex than for ozone because of common indoor sources, such as smoking, cooking, and wood burning.9
Reduction in physical exertion lowers pulmonary ventilation, thus reducing absorption or deposition of air pollutants in the respiratory tract. Breathing through the nose, at rest or at lower levels of exertion, reduces the amount of pollutants reaching the lungs. One study showed a fivefold increase in total deposition of small particles in the lungs during moderate exercise compared with at rest.13
For each person, the benefits of avoiding exposure to air pollution must be weighed against the potential harms of reducing physical activity. Factors to be considered include susceptibility to adverse effects of air pollution; personal and health-related importance of outdoor physical activity; and available opportunities to modify the time, location, duration, or intensity of physical activity. Exercising in the early morning, when air pollution levels are lower, may be a viable option.
Controlled exposure studies have shown wide variability in response to the same level of a given air pollutant, even among healthy persons.14 Similar to that of other triggers, the significance of air pollutants in asthma exacerbations varies widely from person to person. The observed increases in morbidity and mortality associated with acute and long-term increases in PM may disproportionately affect older adults and persons with preexisting heart disease.15,16 Daily AQI reports may give patients the information they need to determine individual susceptibility to levels of specific pollutants, but this has not been formally tested.
Patient Groups at Increased Risk
ASTHMA AND COPD
The National Heart, Lung and Blood Institute evidence-based guidelines for the management of asthma and COPD recommends that physicians advise patients to monitor air quality and to avoid, to the extent possible, exertion or exercise outdoors when levels of air pollution are high.8,17 Epidemiologic and controlled exposure studies have shown that anyone may experience symptoms and compromised lung function from exposure to ozone and PM.18–20 Persons with asthma and COPD are especially vulnerable, because air pollution can trigger exacerbations.5,19,21,22 When levels of these pollutants exceed the NAAQS (AQI value of more than 100), patients with asthma or COPD should limit prolonged outdoor exertion. Even when air pollutants are at moderate levels (AQI value of 51 to 100), some unusually sensitive persons may benefit from reducing exposure.19
Ozone is of particular concern for patients with lung disease. This strong oxidizing compound injures lung tissue and promotes airway inflammation. Ultraviolet light from the sun drives the photochemical reactions that produce ozone from NOx and volatile organic compounds (VOCs). Therefore, ozone levels tend to be highest in the summer, with a broad peak from late morning to early evening. Ozone is usually generated in urban areas that have high concentrations of NOx and VOCs, but it can be transported hundreds of miles downwind where levels may peak later in the evening or at night.10 Patients who are sensitive to ozone should learn the local pattern of ozone concentrations and avoid exposure when levels are highest. In communities that have persistently high ozone levels, adjusting the schedules of organized group athletic activities may be beneficial.
No specific medical treatment has proven effectiveness against air pollution–induced asthma or COPD exacerbations. In a small trial, treatment with inhaled budesonide (Rhinocort) for four weeks reduced ozone-induced inflammation, but did not protect against decreased lung function.23 Supplementation with dietary antioxidants appeared to reduce ozone effects on lung function in healthy adults24 and children with asthma,25 but further study is required. In contrast to allergic asthma triggers, no clinical tests are available for individual sensitivity to air pollutants.
CARDIOVASCULAR DISEASE
Growing evidence suggests that persons with heart disease are susceptible to cardiovascular effects of air pollution, especially PM. Fine particles, or PM2.5 (aerodynamic diameter of 2.5 μm or less), have been most strongly associated with increased cardiovascular morbidity and mortality, including myocardial infarction, arrhythmia, exacerbation of congestive heart failure, and stroke.9 The American Heart Association Scientific Statement on Air Pollution and Cardiovascular Disease supports the use of the AQI to help reduce exposure in persons with heart disease.16
CHILDREN
Children are considered to be more susceptible to air pollution than adults because of their higher relative ventilation rates and more time spent outdoors.26 Young children are also less likely to perceive and report respiratory symptoms.27 Caregivers should be aware of the possible effects of air pollution in all children, but especially those with asthma.19 Exposure to ozone and PM has been associated with increased medication use and hospitalizations among children.28,29
OLDER ADULTS
Studies have suggested that the increased risk of all-cause, cardiac, and pulmonary mortality from PM may be greatest in older adults.30,31 However, the extent to which increased vulnerability to air pollution among older adults may be caused by cardiovascular and pulmonary comorbidities is unknown.32
