A 35-year-old man presented with a nonpruritic rash on his upper extremities and abdomen that had persisted for two years. The rash began on his right hand and left elbow, then spread to his abdomen. The patient had facial swelling and flushing, as well as numbness around lesions that formed on his forearms (Figure 1). He had previously been treated for an allergic reaction, but the rash remained. The patient had emigrated 12 years ago from Mexico. He was not taking medication and had no pets. The review of systems was unremarkable.
Figure 1.

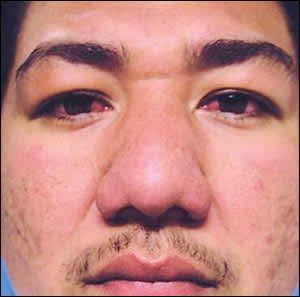
On physical examination, an erythematous plaque was present on his face, along with mild edema of his eyelids, cheeks, and forehead (Figure 2). The conjunctivae were injected bilaterally. The examination also revealed erythematous, hypoesthetic, annular plaques on his right dorsal hand; papules on his dorsal forearms; and hypopigmented patches on his abdomen.
Figure 2.
Question
Based on the patient's history and physical examination, which one of the following is the most likely diagnosis?
A. Cutaneous tuberculosis.
B. Hansen disease (leprosy).
C. Leishmaniasis.
D. Sarcoidosis.
E. Tertiary syphilis.
Discussion
The answer is B: Hansen disease (leprosy). The two primary types of Hansen disease are tuberculoid and lepromatous leprosy. The organism grows best on cooler regions of the body, such as the nose, earlobes, and digits. This patient has tuberculoid leprosy. Skin biopsy showed a superficial and a deeper granulomatous infiltrate, with numerous vacuolated histiocytes and focal perineural granulomas.
Hansen disease is a slowly progressive, infectious disease caused by Mycobacterium leprae. In the United States, 96 cases of the disease were reported in 2002.1 The most common presentations are erythematous or hypopigmented plaques that may be numb. Loss of sweat glands and hair follicles can occur near lesions. Peripheral neuropathy and nerve enlargement are common.2 The classic features of thickened earlobes, loss of lateral eyebrow hair, and leonine facies occur only in patients with lepromatous leprosy. Risk factors for Hansen disease include low socioeconomic status, tropical living environment, immigrant status, and infected family members. Immunocompromise is also a risk factor, particularly with human immunodeficiency virus. Hansen disease is thought to spread mainly through droplet transmission from the nose and mouth. Early diagnosis and treatment can significantly reduce transmission and morbidity. Diagnosis is made through biopsy of suspected lesions, although it is important to obtain tissue from the entire dermis. Diagnosis and treatment information is available at http://www.hrsa.gov/hansens/clinicalcenter.htm.
Cutaneous tuberculosis is a rare manifestation of tuberculosis infection. The most common form of cutaneous tuberculosis is lupus vulgaris, followed by scrofuloderma, tuberculosis verrucosa cutis, tuberculous gumma, and tuberculids.3 Subcutaneous abscesses can lead to breakdown of skin or lymphadenitis, which liquefy and cause a watery or caseous discharge. Diagnosis is made with acid-fast staining and culture, which guides treatment decisions.
Leishmaniasis is caused by protozoan parasites spread through the sand fly. Skin manifestations include localized cutaneous leishmaniasis characterized by painless ulcers; leishmaniasis recidivans that leads to ulcerations, scarring, and new ulcerations; and diffuse cutaneous leishmaniasis characterized by nodules and plaques, especially on cooler regions of the body, as with leprosy.4 Leishmaniasis can be diagnosed with polymerase chain reaction testing.
Sarcoidosis is a disease of unknown etiology involving granulomatous formation in different organs. As much as 20 percent of persons with sarcoidosis have cutaneous reactions, which can include erythema nodosum (associated with benign disease), lupus pernio (sarcoidosis of the nose), and plaques (associated with more chronic disease).5 There is no definitive test for sarcoidosis, and the diagnosis is based on clinical presentation and pathologic features, with exclusion of other causes.
Tertiary syphilis can present as cutaneous granulomas (gumma) and ulcers with round, irregular, or serpiginous shape. Diagnosis is made by direct visualization of organisms or serologic testing. Screening with nontreponemal tests (e.g., Venereal Disease Research Laboratories and rapid plasma reagin testing) requires confirmation with treponemal tests, such as fluorescent treponemal antibody absorption testing. Syphilis lesions generally heal without scarring.6
Summary Table
| Condition | Characteristics |
|---|---|
| Cutaneous tuberculosis | Usually caused by Mycobacterium tuberculosis; subcutaneous abscesses can lead to breakdown of skin or lymphadenitis, which liquefy and cause a watery or caseous discharge |
| Hansen disease (leprosy) | Chronic, indolent, tropical disease; caused by Mycobacterium leprae; peripheral neuropathy and nerve enlargement are common |
| Leishmaniasis | Manifestations include painless ulcers; leishmaniasis recidivans that leads to ulcerations, scarring, and new ulcerations; and diffuse cutaneous leishmaniasis characterized by nodules and plaques, especially on cooler regions of the body (e.g., nose, earlobes, digits) |
| Sarcoidosis | Chronic disease with cutaneous manifestations, including erythema nodosum, lupus-like lesions, and plaques; histopathologic manifestations include noncaseating granulomas |
| Tertiary syphilis | Cutaneous granulomas (gumma) and ulcers, with a round, irregular, or serpiginous shape |
