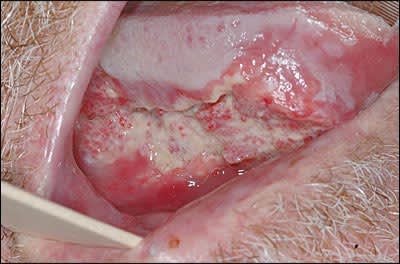
A 55-year-old man with a history of chronic alcoholism presented with pain under the tongue and discomfort when swallowing that had persisted for several weeks. The dorsal surface of the tongue had a relatively normal appearance. However, examination of the undersurface revealed a red and white exophytic growth along the posterolateral border of the right side of the tongue. The lesion was granular, irregular, and ulcerated (see accompanying figure). Cervical lymph nodes were palpable bilaterally.
Question
Based on the patient's history and physical examination, which one of the following is the most likely diagnosis?
A. Chronic traumatic ulcer.
B. Deep fungal infection.
C. Lymphangioma with surface ulcerations.
D. Rhabdomyosarcoma.
E. Squamous cell carcinoma.
Discussion
The correct answer is E: squamous cell carcinoma. Biopsy confirmed the diagnosis of squamous cell carcinoma, which is the most common malignancy in the oral cavity. It is characterized by local infiltration, cervical lymph node involvement, and distant metastasis, especially to the lungs. Early manifestations may include erythroplakia or leukoplakia. The lateral and ventral surfaces of the tongue are the most common sites for intraoral presentation, whereas the dorsal surface is rarely involved.
The initial lesion of squamous cell carcinoma typically progresses into an exophytic, cauliflower-like growth or a burrowing, endophytic growth pattern. The etiology of squamous cell carcinoma is multifactorial. Persons who use tobacco,1 alcohol,1,2 or betel nut3 are at high risk. Although there is increasing evidence implicating certain strains of human papillomavirus in the development of pharyngeal cancer,4 its role in carcinogenesis in the anterior oral cavity is unclear.
Treatment of squamous cell carcinoma includes surgical excision or radiation, alone or in combination, depending on the stage of the lesion. The prognosis is largely determined by the size of the tumor, nodal involvement, and distant metastasis (TNM staging). Patient education about risk factors, coupled with routine oral cancer screenings, may facilitate early detection. In particular, biopsy of persistent leukoplakic and erythroplakic lesions of undetermined etiology is needed.5
Chronic traumatic ulcers, which commonly occur on the lateral border of the tongue, can be caused by fractured, carious, or malpositioned teeth; ill-fitting dentures; and parafunctional habits, such as grinding or clenching. Chronic ulcers have erythematous, rolled borders around a central area of fibrinopurulent tissue and often persist until the causative factor is resolved.
Deep fungal infections, such as mucormycosis and histoplasmosis, may lead to exophytic, ulcerative lesions in the oral cavity with an indurated growth pattern similar to squamous cell carcinoma. These infections are more common in immunocompromised persons and in those with diabetes mellitus.
Lymphangiomas are benign hematomas of the lymphatic vessels that are usually diagnosed in early childhood.6 The tongue is the most common site in the oral cavity.6 The condition appears as a pebbly or granular mass, often with a purplish appearance from ulcerations and subsequent hemorrhage.
Rhabdomyosarcomas are rapidly growing, malignant neoplasms of skeletal origin that usually occur in the first decade of life. Rare cases occur in older persons, especially the pleomorphic form. The condition often affects the head and neck area, most commonly on the palate, and may appear as an exophytic, polypoid, painless mass.7
Summary Table
| Condition | Characteristics |
|---|---|
| Chronic traumatic ulcer | Central ulcerations with erythematous, rolled borders; commonly occurs on lateral border of tongue |
| Deep fungal infections | Red or white ulcerated mass with an indurated growth pattern similar to squamous cell carcinoma; commonly affects the tongue, buccal mucosa, and palate |
| Lymphangioma with surface ulcerations | Benign tumor with a pebbly surface, sometimes with purplish hemorrhagic areas; lesions with surface ulcerations are often noted on the tongue |
| Rhabdomyosarcoma | Exophytic, polypoid, painless mass that grows rapidly; often occurs in the head and neck area, most commonly on the palate |
| Squamous cell carcinoma | Red or white lesion with an irregular, fungating growth; surface ulcerations; commonly appears on lateral and ventral tongue surfaces or on the floor of the mouth |
