
Am Fam Physician. 2010;81(7):903-904
Author disclosure: Nothing to disclose.
A 37-year-old woman presented with a productive cough and chills, which began four weeks earlier. She was given azithromycin (Zithromax), but her symptoms did not improve. Instead, she experienced increasing productive cough with dark, foul-smelling sputum, and midsternal and left back pain that worsened when coughing. She did not have hemoptysis.
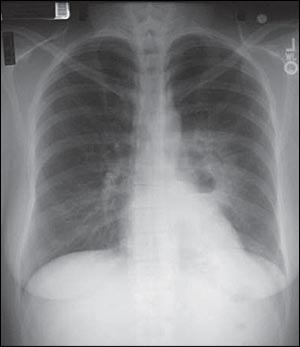
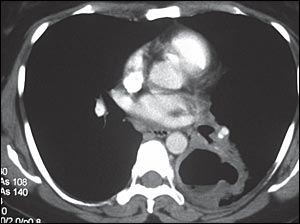
The patient had a fever of 102.3°F (39°C), pulse rate of 102 beats per minute, blood pressure of 121/65 mm Hg, and room air pulse oximetry measurement of 98 percent. Auscultation of the lungs revealed crackles in the left lower lung field. Except for mild tachycardia, the heart examination was unremarkable. Her white blood cell count was elevated at 14,500 per mm3 (14.5 × 109 per L) with no bands. Chest radiography (Figure 1) and computed tomography (CT, Figure 2) were performed.
Question
Discussion
The answer is D: lung abscess. Lung abscess is a localized cavity parenchyma necrosis often caused by microbial infection. The condition can be acute or chronic, if the symptoms last for more than one month.1 Lung abscesses are also categorized as primary or secondary. Primary abscesses are caused by aspiration and usually occur in otherwise healthy persons, whereas secondary abscesses are associated with systemic disease (e.g., malignancy, autoimmune disorders, other immunocompromised conditions).1 Bacteria-related lung abscesses are usually caused by anaerobes and are often polymicrobial, reflecting the normal flora in the oral cavity. Although aspiration is the usual route of bacterial entry, septic emboli from endocarditis or peritonsillar infections may occur.2
Symptoms of a lung abscess evolve over weeks to months and may include fever, productive cough, foul-smelling or bad-tasting sputum, night sweats, and hemoptysis.1–3 Diagnosis is confirmed through chest radiography or CT findings. Imaging reveals a cavitary lesion with fluid level. Bronchoscopy may be performed if malignancy is suspected.1–4
Antibiotic therapy is the first-line treatment for a lung abscess, followed by surgery in patients who do not respond to medical management or in the presence of malignancy. Clindamycin (Cleocin), with or without metronidazole (Flagyl), is the preferred agent. Treatment duration should be based on response to therapy.1,3 Factors that may predict a worse prognosis include hemoglobin level of less than 10 g per dL (100 g per L); larger abscess; and infection with Pseudomonas aeruginosa, Staphylococcus aureus, or Klebsiella pneumoniae.5
Aspergilloma has a wide variety of clinical presentations, including cough, weight loss, fever, and hemoptysis, although it may be asymptomatic. CT often demonstrates a soft tissue mass within the lung cavity, usually located in the upper lobe, that is typically separated from the cavity wall by airspace (air crescent sign).6
Bronchiectasis is caused by chronic inflammation of the airways. It is characterized by a productive, chronic cough that is sometimes accompanied by hemoptysis. The condition is either a focal or a diffuse process that usually affects the lower lobes. Chest CT findings include increased airway diameter, lack of peripheral airway tapering, airway constrictions, and ballooned cysts toward the end of the bronchus.7
| Condition | Characteristics |
|---|---|
| Aspergilloma | Varied clinical presentation similar to lung abscess, including cough, weight loss, fever, and hemoptysis; may be asymptomatic; CT reveals soft tissue mass in the lung, usually the upper lobe, separated from cavity wall by airspace (air crescent sign) |
| Bronchiectasis | Chronic, productive cough sometimes accompanied by hemoptysis; CT shows increased airway diameter, lack of peripheral airway tapering, airway constrictions, and ballooned cysts toward the end of the bronchus |
| Localized empyema | Symptoms similar to lung abscess; however, CT helps differentiate the conditions |
| Lung abscess | Localized lung parenchymal necrosis; symptoms include fever, productive cough, foul-smelling or bad-tasting sputum, night sweats, hemoptysis; radiography shows cavitary lesion with fluid level |
