Contact dermatitis is a common inflammatory skin condition characterized by erythematous and pruritic skin lesions that occur after contact with a foreign substance. There are two forms of contact dermatitis: irritant and allergic. Irritant contact dermatitis is caused by the non–immune-modulated irritation of the skin by a substance, leading to skin changes. Allergic contact dermatitis is a delayed hypersensitivity reaction in which a foreign substance comes into contact with the skin; skin changes occur after reexposure to the substance. The most common substances that cause contact dermatitis include poison ivy, nickel, and fragrances. Contact dermatitis usually leads to erythema and scaling with visible borders. Itching and discomfort may also occur. Acute cases may involve a dramatic flare with erythema, vesicles, and bullae; chronic cases may involve lichen with cracks and fissures. When a possible causative substance is known, the first step in confirming the diagnosis is determining whether the problem resolves with avoidance of the substance. Localized acute allergic contact dermatitis lesions are successfully treated with mid- or high-potency topical steroids, such as triamcinolone 0.1% or clobetasol 0.05%. If allergic contact dermatitis involves an extensive area of skin (greater than 20 percent), systemic steroid therapy is often required and offers relief within 12 to 24 hours. In patients with severe rhus dermatitis, oral prednisone should be tapered over two to three weeks because rapid discontinuation of steroids can cause rebound dermatitis. If treatment fails and the diagnosis or specific allergen remains unknown, patch testing should be performed.
Contact dermatitis is a common inflammatory skin condition characterized by erythematous and pruritic skin lesions after contact with a foreign substance. The condition can be categorized as irritant or allergic. Irritant contact dermatitis is caused by non–immune-modulated irritation of the skin by a substance, leading to skin changes.1 Allergic contact dermatitis is a delayed hypersensitivity reaction in which a foreign substance comes into contact with the skin; skin changes occur with reexposure.
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendation | Evidence rating | References |
|---|---|---|
| In patients with contact dermatitis, the priority is to identify and avoid the causative substance. | C | 3 |
| Localized acute allergic contact dermatitis lesions are successfully treated with mid- or high-potency topical steroids, such as triamcinolone 0.1% (Kenalog, Aristocort) or clobetasol 0.05% (Temovate). | C | 4 |
| On areas with thinner skin (e.g., flexural surfaces, eyelids, face, anogenital region), lower-potency steroids, such as desonide ointment (Desowen), can be helpful and minimize the risk of skin atrophy. | C | 4 |
| If allergic contact dermatitis involves extensive areas of the skin (greater than 20 percent), systemic steroid therapy is often required and offers relief within 12 to 24 hours. | C | 4 |
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.xml.
Epidemiology
Data from the National Health Interview Survey (n = 30,074) showed a 12-month prevalence for occupational contact dermatitis of 1,700 per 100,000 workers.2 According to another study, the industries with the highest rates of contact dermatitis are natural resources and mining, manufacturing, and health services.3
Occupational skin diseases rank second only to traumatic injuries as the most common types of occupational disease. Chemical irritants, such as solvents and cutting fluids used in machining, account for most cases of irritant contact dermatitis. One study showed that hands were primarily affected in 64 percent of workers with allergic contact dermatitis and 80 percent of those with the irritant form.4
Pathophysiology
Irritant contact dermatitis is caused by skin injury, direct cytotoxic effects, or cutaneous inflammation from contact with an irritant. Symptoms may occur immediately and may persist if the irritant is unrecognized.
Allergic contact dermatitis is caused by a type IV, T cell–mediated, delayed hypersensitivity reaction in which a foreign substance comes into contact with the skin and is linked to skin protein, forming an antigen complex that leads to sensitization. Upon reexposure of the epidermis to the antigen, the sensitized T cells initiate an inflammatory cascade, causing the skin changes associated with allergic contact dermatitis.1
Common substances that cause contact dermatitis include poison ivy, nickel, and fragrances.4 Patch testing data have shown that out of 3,700 known contact allergens, nickel caused contact dermatitis in 14.3 percent of patients, fragrance mix in 14 percent, neomycin in 11.6 percent, balsam of Peru in 10.4 percent, and thimerosal in 10.4 percent.5
Nickel is a component of many different types of metals, including white gold, German silver, nickel and gold plating, solder, and stainless steel.6 Unilateral nickel-induced facial dermatitis elicited by cell phone use has been reported.7 Hairdressers have been diagnosed with allergy-related hand eczema from prolonged skin contact with nickel-containing scissors and crochet hooks.8
Of the approximately 2,500 fragrance ingredients currently used in perfumes, at least 100 are known contact allergens.9 In addition to perfumes, these fragrances are used in cosmetics, shampoos and other hair products, soaps, moisturizers, and deodorants. Fragrance mix produces a patch testing reaction in about 10 percent of patients with eczema; 1.7 to 4.1 percent of the general population is sensitized to fragrance mix.9 Allergic contact dermatitis caused by fragrance occurs predominantly in women with facial or hand eczema.9
Balsam of Peru is used in many personal products and cosmetics as a fragrance or as a fragrance masker in products labeled “unscented.” Balsam is also found in many foods and beverages, including spices, ketchup, chili sauce, barbecue sauce, citrus products, colas, beers, wines, bakery items, candy, ice cream, chocolate, and tomatoes.10 Studies show that balsam-restricted diets improve systemic contact dermatitis in patients with contact allergy to balsam of Peru.10
Neomycin is a common over-the-counter topical antibiotic. Because of the antibacterial and antifungal properties of organomercurials, thimerosal has been used as a topical disinfectant and preservative in medical preparations.11
Clinical Presentation
The clinical presentation of contact dermatitis varies based on the causative allergen or irritant and the affected area of skin. Table 1 summarizes the features that help distinguish between irritant and allergic contact dermatitis.1
Table 1. Features to Help Distinguish Between Irritant and Allergic Contact Dermatitis
| Feature | Irritant | Allergic |
|---|---|---|
| Location | Usually the hands | Usually exposed areas of skin, often the hands |
| Symptoms | Burning, pruritus, pain | Pruritus is the dominant symptom |
| Surface appearance | Dry and fissured skin | Vesicles and bullae |
| Lesion borders | Less distinct borders | Distinct angles, lines, and borders |
Information from reference 1.
Contact dermatitis usually manifests as erythema and scaling with relatively well-demarcated, visible borders. The hands, face, and neck are usually involved, although any area can be affected. Irritant contact dermatitis may occur on the lips with excessive lip licking and in the diaper region (irritant diaper dermatitis). Some manifestations of contact dermatitis can be both allergic and irritant. The patient may describe itching and discomfort, but some patients seek medical care based on the appearance of the rash. Acute cases may involve a dramatic flare with erythema, vesicles, and bullae; chronic cases may involve lichen with cracks and fissures. Patient history is crucial in making the diagnosis, and the causative substance must be determined to resolve the dermatitis and prevent further damage.
A common cause of allergic contact dermatitis is exposure to urushiol, a substance in the sap of rhus plants (e.g., poison ivy, oak, sumac). Rhus plants often brush across the skin causing linear streaks of erythema and vesicles (Figure 1). Rhus dermatitis may also cover large areas of the body, including the face and genitals, leading to severe discomfort and distress. More than 70 percent of persons who are exposed to urushiol can become sensitized.12
Figure 1.

A linear pattern of allergic contact dermatitis from poison ivy.
Allergic contact dermatitis caused by metals in jewelry often can be diagnosed with observation of the rash. Less expensive jewelry, and metal belt buckles and pant closures containing nickel commonly cause allergic contact dermatitis (Figure 2). Inexpensive kits that use dimethylglyoxime to test metals for nickel are widely available to consumers online.
Figure 2.
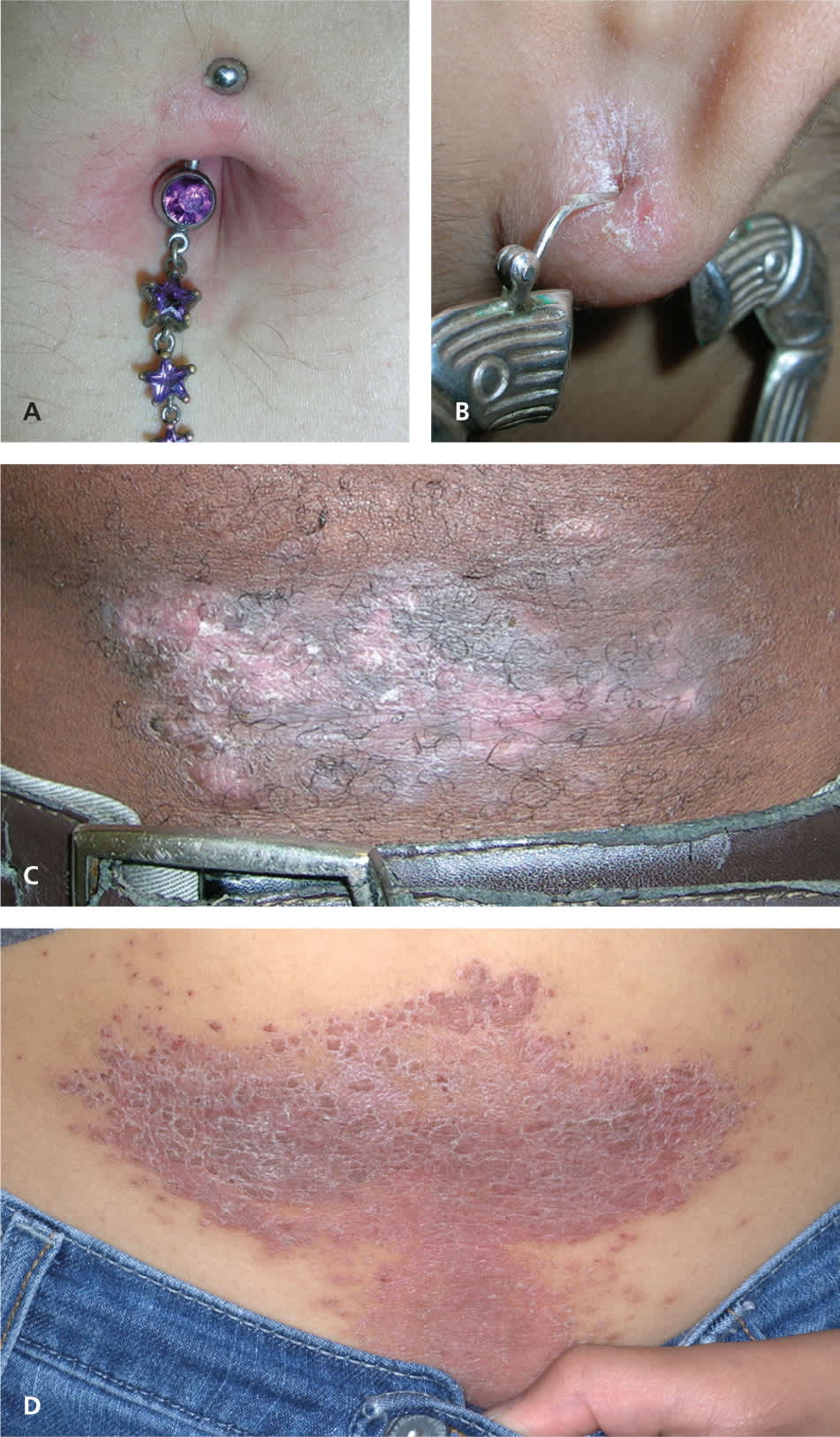
Common causes of allergic contact dermatitis from nickel exposure. Reaction to metal in (A) belly-button ring, (B) earring, (C) belt buckle, (D) pant closure. Note the scaling and erythema typical of this reaction.
Allergic contact dermatitis from topical products (e.g., medicines, cosmetics, adhesive tape) often produces reactions with well-demarcated borders (Figures 3 and 413 ). Dermatitis of the hand has variable presentations, from mild irritant dermatitis to a more severe allergic contact dermatitis (Figure 5). Dermatitis of the foot is more common on the dorsal surfaces rather than on the soles (Figure 6).
Figure 3.
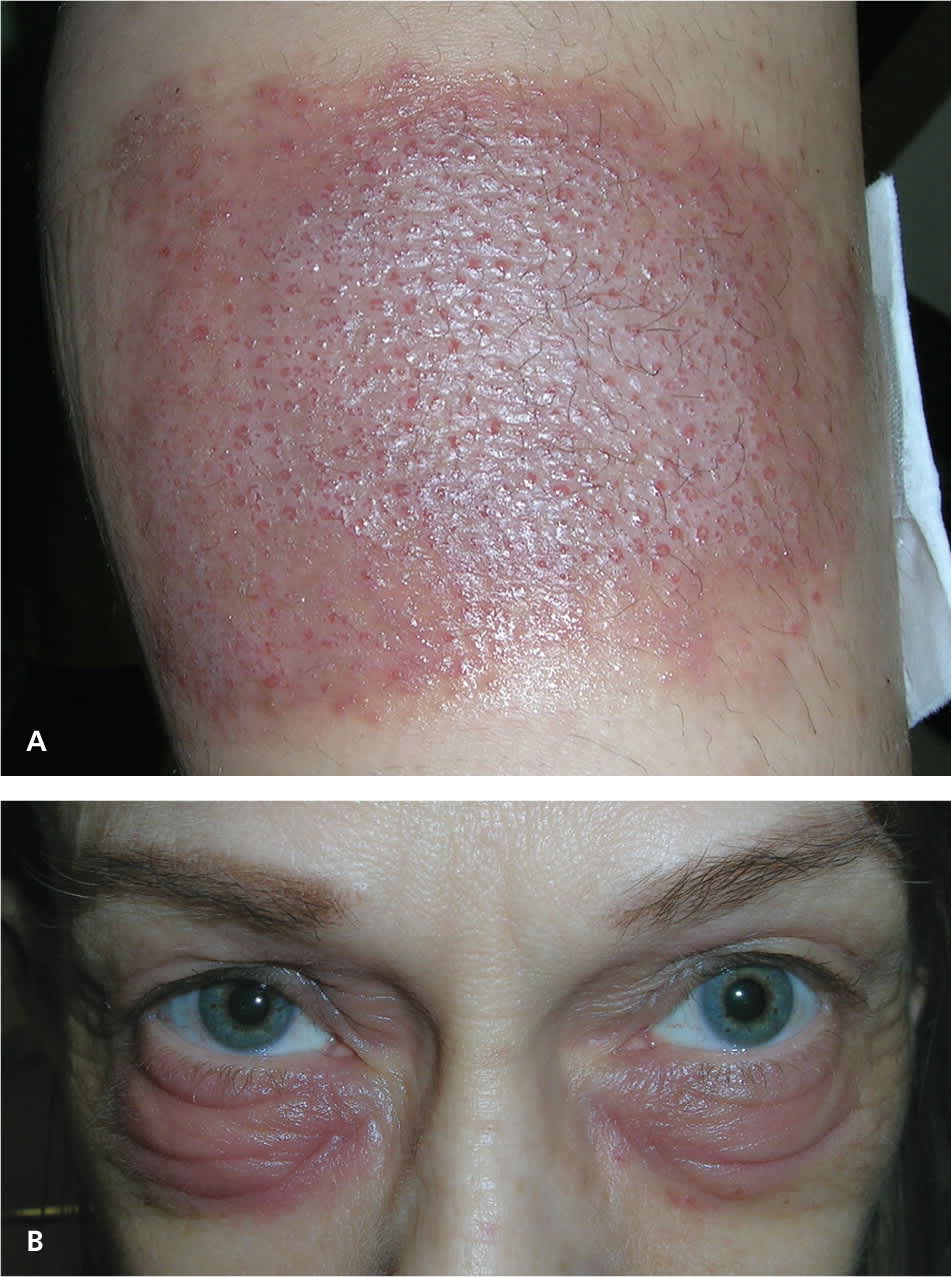
Allergic contact dermatitis caused by neomycin (A) on the leg in the pattern of a large nonstick pad used to cover the antibiotic ointment and (B) under the eyes.
Figure 4.

Acute allergic contact dermatitis caused by (A) topical herbal medicine for a sprained ankle (severe reaction), (B) fragrance in deodorant, and (C) adhesive tape used after abdominal hysterectomy.
Reprinted with permission from Halstater B, Usatine RP. Contact dermatitis. In: Milgrom EC, Usatine RP, Tan RA, Spector SL. Practical Allergy. Philadelphia, Pa.: Elsevier; 2004.
Figure 5.

Contact dermatitis of the hand. (A) Irritant contact dermatitis in a health care worker. (B) Allergic contact dermatitis in a custodial engineer.
Figure 6.

Allergic contact dermatitis from new shoes. Note the typical distribution on the dorsum of the feet.
Diagnosis
The diagnosis of contact dermatitis is most often made with history and physical examination findings. Table 2 summarizes the differential diagnosis of contact dermatitis.
Table 2. Differential Diagnosis of Contact Dermatitis
| Conditions | Distinguishing features | Method for diagnosis | Treatment principles |
|---|---|---|---|
| Atopic dermatitis | More widespread than contact dermatitis and follows a certain distribution involving flexor surfaces | History and clinical appearance, skin biopsy when uncertain | Topical steroids and emollients |
| Dyshidrotic eczema | Occurs on the hands and feet with clear, deep-seated vesicles resembling tapioca; erythema; and scaling | History and clinical appearance, skin biopsy when uncertain | Topical steroids and emollients |
| Inverse psoriasis | Well-demarcated erythema in intertriginous areas | History and clinical appearance, skin biopsy when uncertain | Topical steroids and topical calcineurin inhibitors |
| Latex allergy | Erythema, pruritus, and possibly a systemic reaction | History and clinical appearance, allergy testing when uncertain | Avoidance of latex |
| Palmoplantar psoriasis | Plaques and pustules on the palms and soles | History and clinical appearance, skin biopsy when uncertain | Potent topical steroids and oral retinoids |
| Scabies | Burrows and typical distribution on hands, feet, waist, axilla, or groin | History and clinical appearance, skin scraping when uncertain | Overnight therapy with permethrin (Elimite) |
| Tinea pedis | Usually occurs between toes, on the soles, and on the sides of the feet; whereas contact dermatitis is more common on the dorsum of the foot | History and clinical appearance, potassium hydroxide testing when uncertain | Topical and/or oral antifungal medications |
Irritant and allergic contact dermatitis may be complicated by bacterial superinfection, and bacterial culture should be considered with the presence of exudate, weeping, and crusting. A potassium hydroxide (KOH) preparation is useful if tinea or Candida infection is suspected, because these fungal infections can have erythema and scaling similar to contact dermatitis. If the KOH preparation has negative results but a fungal etiology is still suspected, a fungal culture should be sent for laboratory testing. Dermoscopy and microscopy can be used to look for scabies and mites.
When a possible causative substance is known, the first step in confirming the diagnosis is observing whether the problem resolves with avoidance of the substance. If avoidance and empiric treatment do not resolve the dermatitis or the allergen remains unknown, patch testing may be indicated. In one study, patch testing had a sensitivity and specificity of between 70 and 80 percent.14 However, it is expensive and time-consuming, and prohibits the patient from showering (a “sponge bath” technique may be used). Patch testing should not be confused with other types of allergy testing. Skin prick and radioallergosorbent tests are used for the diagnosis of type I hypersensitivity, such as respiratory, latex, and food allergies, but not for contact dermatitis.
The patient may be referred to a dermatologist with experience in patch testing, or patch test kits and individual allergens can be purchased for testing in the physician’s office. One kit is the TRUE (Thin-layer Rapid Use Epicutaneous) Test, which consists of three panels with 29 antigens commonly involved in allergic contact dermatitis (Table 315 and Figure 7). Although the TRUE Test is expensive, reimbursement compensates for the cost of the test.
Table 3. TRUE Test Allergen Panels: Patch Test for Contact Dermatitis
| Panel 1.1 |
| 1. Nickel sulfate |
| 2. Wool alcohols |
| 3. Neomycin |
| 4. Potassium dichromate |
| 5. Caine mix |
| 6. Fragrance mix |
| 7. Colophony |
| 8. Paraben mix |
| 9. Negative control |
| 10. Balsam of Peru |
| 11. Ethylenediamine dihydrochloride |
| 12. Cobalt dichloride |
| Panel 2.1 |
| 13. p-tert-butylphenol formaldehyde resin |
| 14. Epoxy resin |
| 15. Carba mix |
| 16. Black rubber mix |
| 17. Methylchloroisothiazolinone/methylisothiazolinone |
| 18. Quaternium-15 |
| 19. Mercaptobenzothiazole |
| 20. p-Phenylenediamine |
| 21. Formaldehyde |
| 22. Mercapto mix |
| 23. Thimerosal |
| 24. Thiuram mix |
| Panel 3.1 |
| 25. Diazolidinyl urea |
| 26. Imidazolidinyl urea |
| 27. Budesonide (Rhinocort) |
| 28. Tixocortol-21-pivalate |
| 29. Quinoline mix |
note: See Figure 7B for a photo of the panels with a positive reaction for No. 20, p-Phenylenediamine.
TRUE = Thin-layer Rapid Use Epicutaneous.
Adapted with permission from T.R.U.E. Test Patch Test System, manufactured for SmartPractice by Mekos Laboratories. http://www.truetest.com/panelallergens.aspx. Accessed April 15, 2010.
Figure 7.

(A) Allergic contact dermatitis from a chemical in hair dye. (B) Patch testing in the same patient. The positive TRUE Test result for No. 20 (p-Phenylenediamine), an ingredient in hair dye, was crucial in identifying the patient’s allergy. See Table 3 for names of each allergen in the panels.
In a recent meta-analysis, the most prevalent allergens detected using the TRUE Test were nickel (14.7 percent of patients), thimerosal (5.0 percent), cobalt (4.8 percent), fragrance mix (3.4 percent), and balsam of Peru (3.0 percent).5 The TRUE Test may miss some important antigens, however. If the suspected allergen is not included in the TRUE Test, the patient may be referred to a subspecialist who offers customized patch testing. Personal products, such as cosmetics and lotions, can be diluted for specialized patch testing.
Management
In patients with contact dermatitis, the priority is to identify and avoid the causative substance.3 Cool compresses can soothe the symptoms of acute contact dermatitis, and calamine lotion and colloidal oatmeal baths may help dry and soothe acute, oozing lesions.4
Localized acute allergic contact dermatitis lesions are successfully treated with mid- or high-potency topical steroids, such as triamcinolone 0.1% (Kenalog, Aristocort) or clobetasol 0.05% (Temovate).4 On areas with thinner skin (e.g., flexural surfaces, eyelids, face, anogenital region), lower-potency steroids, such as desonide ointment (Desowen), can be helpful and minimize the risk of skin atrophy.4 There are insufficient data to support the use of topical steroids for irritant contact dermatitis. However, because it is difficult to clinically distinguish between allergic and irritant contact dermatitis, these agents are often used successfully for the irritant form.
If allergic contact dermatitis involves an extensive area of skin (greater than 20 percent), systemic steroid therapy is often required and offers relief within 12 to 24 hours.4 Five to seven days of prednisone, 0.5 to 1 mg per kg daily, is recommended. If the patient is comfortable after this initial therapy, the dose may be reduced by 50 percent for the next five to seven days. The rate of reduction of the steroid dosage depends on factors such as the severity and duration of allergic contact dermatitis, and how effectively the allergen can be avoided.4 In severe rhus dermatitis, oral prednisone should be tapered over two to three weeks because rapid discontinuation of steroids can cause rebound dermatitis. A steroid dose pack has insufficient dosing and duration and should not be prescribed. There is no evidence to support the use of long-acting injectable steroids in the treatment of contact dermatitis.
In patients with nickel-induced contact dermatitis, it is helpful to cover the metal tab of jeans with an iron-on patch (most effective) or a few coats of clear nail polish. Clear nail polish can also be used on belt buckles, but may need to be reapplied often.
Some patients may be allergic to preservatives used in the base of steroid creams. Steroid ointment is recommended because it allows the medication to maintain contact with the skin longer and there is little risk of an allergic reaction (allergic reaction to the steroid itself is rare). Also, soaking the affected areas before applying the steroid is thought to help improve penetration and increase its effectiveness.16
Although antihistamines are generally not effective for pruritus associated with allergic contact dermatitis, they are commonly used. Sedation from more soporific antihistamines (e.g., diphenhydramine [Benadryl], hydroxyzine [Vistaril]) may offer some degree of relief.4 Emollients, moisturizers, or barrier creams may be instituted as secondary prevention strategies to help avoid continued exposure.4 To prevent irritant contact dermatitis of the hands, persons should avoid latex gloves; wear nonlatex gloves when working with potentially irritating substances, such as solvents, soaps, and detergents; use cotton liners under the gloves for comfort and absorption of sweat; and keep hands clean, dry, and well moisturized when possible.
