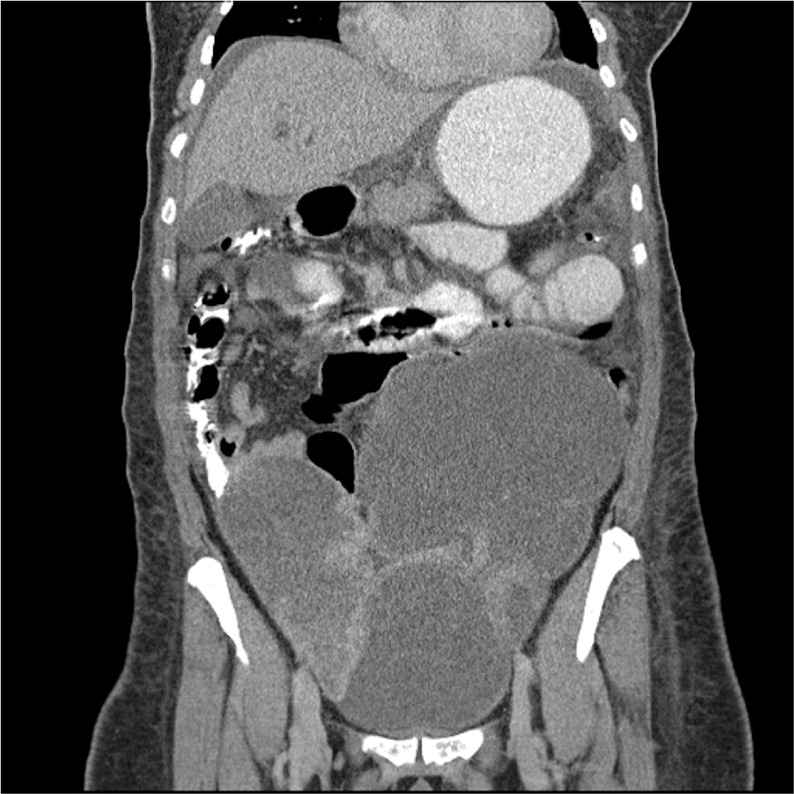
A 58-year-old woman who had never visited a physician was admitted to the hospital with generalized weakness and progressive abdominal distension of one month's duration. A palpable lower abdominal mass was found on physical examination. Computed tomography (CT) of the abdomen and pelvis showed bilateral ovarian tumors with mass effect on adjacent ureters and the small bowel (see accompanying figure). Bony metastases also were detected on CT. The patient was scheduled for urgent surgical intervention, but she developed coffee-ground emesis. An emergent upper endoscopy was performed and revealed a 1-cm, nonbleeding ulcer with an irregular base and slightly raised borders located on the angularis of the stomach. A biopsy of the ulcer was performed during the endoscopy.
Question
Based on the patient's history, physical examination, and imaging findings, which one of the following is the most likely diagnosis?
A. Blumer shelf tumor.
B. Irish node.
C. Krukenberg tumor.
D. Sister Mary Joseph node.
E. Virchow node.
Discussion
The answer is C: Krukenberg tumor.1 The biopsy of this patient's ulcer was consistent with signet ring cell gastric adenocarcinoma. Krukenberg tumor reflects the metastatic spread of a gastrointestinal malignancy to the ovaries, classically from a stomach cancer, by lymphatic, hematologic, or direct peritoneal seeding. At the time of presentation, the tumors often are bilateral and bulky, and may cause ureteral and intestinal obstruction. Ovarian involvement leads to poor prognosis, with median survival of less than one year. Treatment options include chemotherapy and surgical debulking.
Blumer shelf tumor represents metastatic seeding of a primary gastrointestinal tumor (usually stomach) into the caudal portion of the peritoneal cavity, or the pouch of Douglas. Digital rectal examination may detect an appreciable mass. Symptoms may include lower abdominal pain, change in bowel habits, and tenesmus.
Irish node is a palpable left anterior axillary lymph node. It is thought to arise from intrathoracic metastatic spread of an intra-abdominal malignancy, particularly gastric cancer.
Sister Mary Joseph node is a malignant umbilical tumor associated with metastatic spread of an intra-abdominal malignancy, commonly gastric cancer. The route of spread is along the falciform ligament. Prognosis is particularly poor because Sister Mary Joseph node indicates advanced disease.
Similar to Irish node, Virchow node (Troiser sign) is a palpable, firm left supraclavicular lymph node that is related to metastatic spread of intra-abdominal cancer. It can present as the initial sign of an undetected gastric cancer.
Summary Table
| Condition | Characteristics |
|---|---|
| Blumer shelf tumor | Metastatic spread of gastric cancer to the pouch of Douglas |
| Irish node | Metastatic spread of gastric cancer to the left anterior axillary lymph node |
| Krukenberg tumor | Metastatic spread of gastric cancer to the ovaries |
| Sister Mary Joseph node | Metastatic spread of gastric cancer to the umbilicus |
| Virchow node | Metastatic spread of gastric cancer to the left supraclavicular lymph node |
