A 22-year-old woman presented with malodorous vaginal discharge and soreness that began one week earlier. She had dyspareunia, but no itching, dysuria, or lower abdominal pain. She was not douching or using any local intravaginal chemical treatment. She had multiple sex partners and had chlamydia infection twice within the previous year. She had one pregnancy, which was uncomplicated.
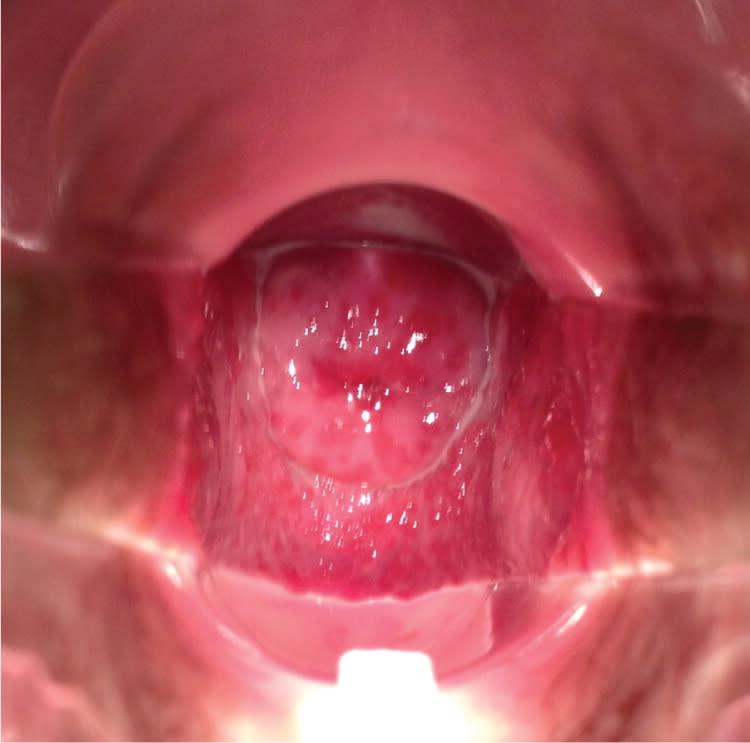
Examination of the vulva was unremarkable. Speculum examination of the vagina revealed multiple small, erythematous macules covering the vaginal wall and ectocervix (see accompanying figure), and a moderate amount of homogeneous yellowish discharge. Microscopic examination of the vaginal secretions with saline showed a motile organism and an excessive number of leukocytes. Results of a potassium hydroxide preparation and rapid testing for chlamydia, gonorrhea, and human immunodeficiency virus infections were negative.
Figure.
Question
Based on the patient's history, physical examination, and microscopy findings, which one of the following is the most likely diagnosis?
A. Bacterial vaginosis.
B. Irritant or allergic contact dermatitis.
C. Trichomoniasis.
D. Vulvovaginal candidiasis.
Discussion
The answer is C: Trichomoniasis. This is a common vaginal infection caused by the protozoan Trichomonas vaginalis. Most men infected with T. vaginalis are asymptomatic, but one-half of women report symptoms.1 The infection is predominantly transmitted via sexual contact.1 In the United States, there are an estimated 7.4 million new cases of trichomoniasis annually.2
The clinical presentation of trichomoniasis is a copious, yellow-gray, homogeneous, frothy, purulent discharge and an alkaline vaginal pH. An inflamed strawberry cervix occurs in about 5% to 10% of cases.2,3 The strawberry cervix is the most specific clinical finding (specificity of 99%, P < .001), with a positive predictive value of 90% for the diagnosis of trichomoniasis.4 The diagnosis is confirmed by observing motile, flagellated organisms and leukocytes on microscopy. Microscopy is nondiagnostic in one-fourth of infected patients. A rapid test that takes 10 minutes for results is approximately 90% sensitive and 97% specific.5 Culture is the most sensitive and specific method of diagnosis.2,5,6
Bacterial vaginosis is the most common cause of vaginal discharge in the United States, accounting for 40% to 50% of cases in women of childbearing age.2 It is caused by an overgrowth of anaerobic bacteria and is associated with a nonpruritic, malodorous vaginal discharge. More than 50% of women with bacterial vaginosis are asymptomatic.5 The condition can be diagnosed if three of the following are present: thin, dull-gray, homogeneous, malodorous discharge that adheres to the vaginal wall; elevated vaginal pH (more than 4.5); a fishy odor noted after adding potassium hydroxide to the discharge (“whiff test”); or epithelial cells coated with coccobacilli (clue cells) on microscopic evaluation. These diagnostic criteria are approximately 90% sensitive and 90% specific.2,5
Irritant or allergic contact dermatitis is a noninfectious cause of vaginitis that may be associated with use of feminine hygiene products, lubricants, or contraceptive materials. It is associated with acute burning and pain on contact with the irritant, as well as vulvar erythema. Vulvar edema may be present, but vaginal discharge is minimal. Diagnosis is based on history and physical examination findings, with exclusion of other causes of vaginitis.5
Candidiasis is the second most common cause of vaginitis in the United States; Candida albicans causes 80% to 90% of cases.2 Risk factors are diabetes mellitus; pregnancy; antibiotic use; receptive oral sex; first intercourse; and use of oral contraceptives, an intrauterine device, or a diaphragm. The discharge is usually white and thick (resembling cottage cheese), with itching and dysuria. There is no odor, and the pH is normal. Women with candidiasis may have vulvar and vaginal erythema, and occasionally scaling and fissures of vulvar tissue. Microscopic examination shows pseudohyphae, mycelia tangles, or budding yeast cells in 50% to 70% of patients.2,5
Summary Table
| Condition | Characteristics | Diagnosis |
|---|---|---|
| Bacterial vaginosis | Fishy odor that increases after sexual intercourse; thin, dull-gray, nonpruritic, homogeneous discharge that adheres to vaginal wall | Elevated vaginal pH (> 4.5); clue cells (epithelial cells coated with coccobacilli); positive whiff test (fishy odor noted after adding potassium hydroxide to the discharge) |
| Irritant or allergic contact dermatitis | Acute pain and burning on contact with irritant; vulvar erythema and possibly edema; minimal discharge | Diagnosis of exclusion |
| Trichomoniasis | Copious, malodorous, yellow-gray, frothy, purulent discharge; strawberry cervix; vaginal irritation; usually pruritus | Elevated vaginal pH (> 4.5); motile trichomonads; many polymorphs; whiff test may be positive |
| Vulvovaginal candidiasis | Thick, white (“cottage cheese”) discharge with pruritus and dysuria; no odor | Normal vaginal pH; microscopy shows pseudohyphae, mycelia tangles, or budding yeast cells; negative whiff test |
