A 19-year-old man with autism presented with a solitary erythematous nodule on his chin that had been present for three months. The patient's mother thought the lesion was not particularly painful or pruritic, but she occasionally noticed him picking at the spot. They had not noticed any drainage. He had no fever or chills, and no history of dental or oral symptoms. He had no other lesions. He was prescribed a 10-day course of oral clindamycin, which reduced the size of the lesion. However, the lesion persisted.
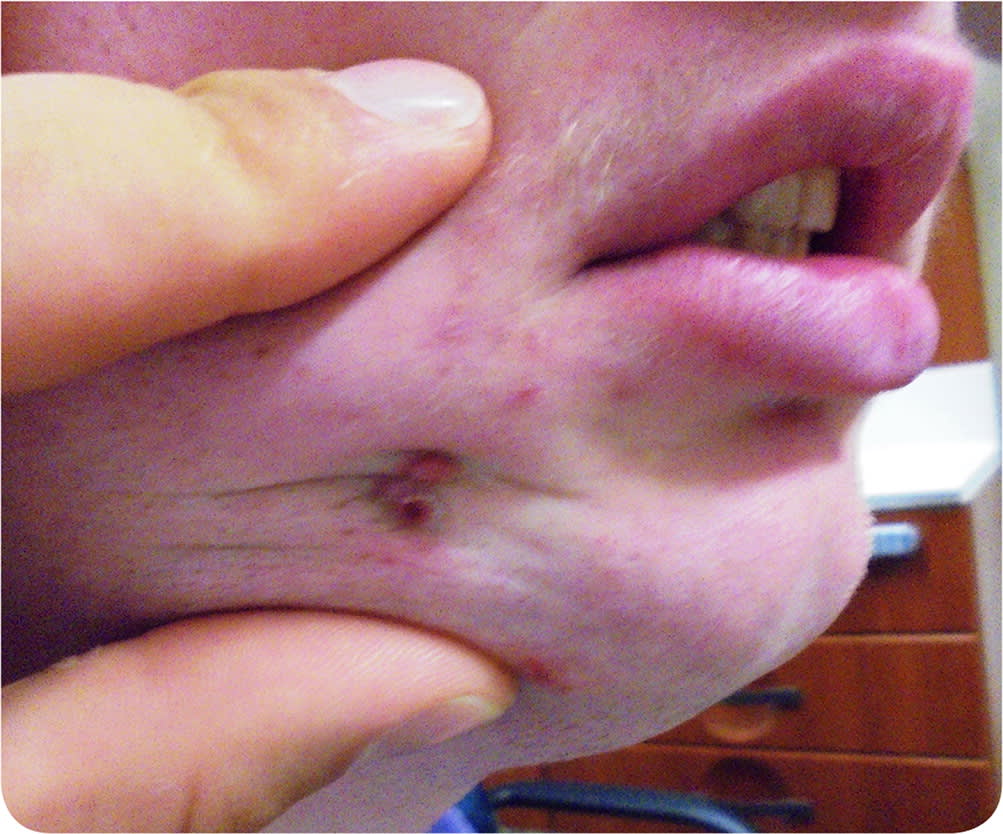
Physical examination revealed a cluster of two 2- to 4-mm, erythematous, crusted, dome-shaped papules situated within a dimpling on the patient's lateral chin (Figure 1). On palpation, the area was slightly indurated, and the lesions seemed fixed and immobile when the surrounding skin was manipulated. There was no fluctuance or discharge. On palpation of the buccal mucosa, an indurated subcutaneous cord was appreciated emanating from the lesion and tracking down to the angle of the mandible.
FIGURE 1
Question
Based on the patient's history and physical examination findings, which one of the following is the most appropriate next step?
A. Perform punch biopsy of the erythematous lesion.
B. Prescribe a 10-day course of oral trimethoprim/sulfamethoxazole.
C. Prescribe a course of topical salicylic acid 17% solution.
D. Prescribe topical benzoyl peroxide 5% wash and tretinoin 0.05% cream (Retin-A).
E. Refer the patient for oral imaging and dental examination.
Discussion
The correct answer is E: refer the patient for oral imaging and dental examination. A panoramic radiograph showed a well-defined periapical radiolucency around the distal root of the tooth, consistent with an abscess (Figure 2). An orocutaneous fistula may also be known as a dental sinus, periapical abscess with sinus, or odontogenic cutaneous sinus tract. It occurs when a tract forms between the skin surface and an infection within the oral cavity. It is rare and can be misdiagnosed and ineffectively treated with antibiotics or surgical procedures.1
FIGURE 2
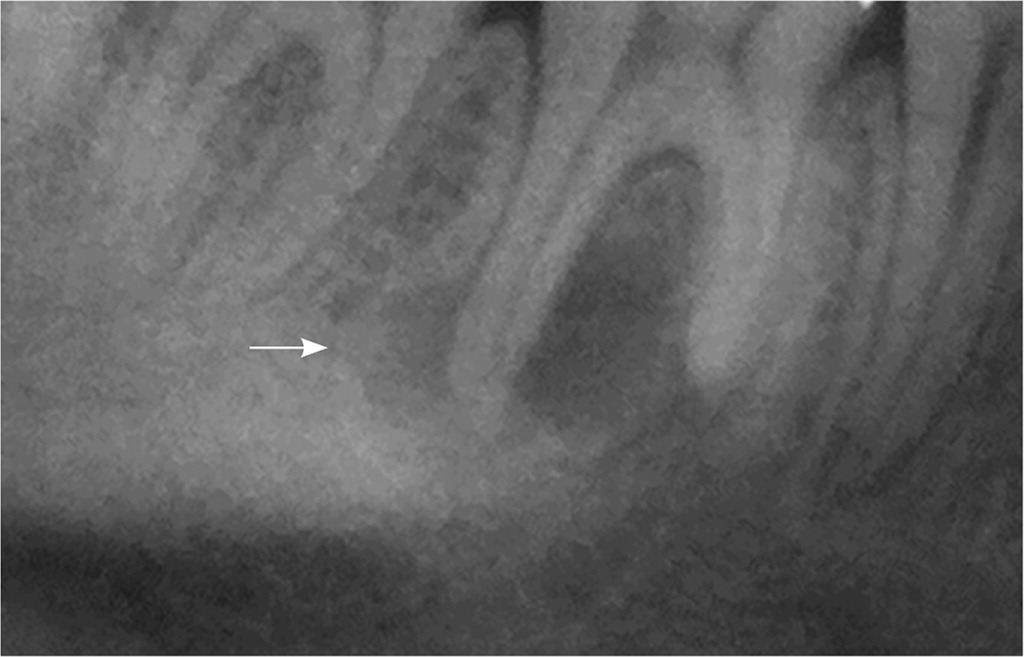
A panoramic radiograph showing a well-defined periapical radiolucency around the distal root of the tooth (arrow), consistent with an abscess.
Orocutaneous fistulas present as erythematous nodules that are often associated with intermittent drainage and tooth or jaw pain. Infections that arise from dental caries, pulpal necrosis, pericoronitis, or traumatic injury may erode the cortical plate of the jaw, leading to a subperiosteal abscess. Fluid from the abscess may form a tract or fistula with surrounding soft tissue.2 One-half of orocutaneous fistulas are not associated with dental symptoms. This is likely because of the drainage of fluid through the sinus tract, which relieves pressure from the primary site of infection.3 Most dental sinuses (80%) develop from mandibular abscesses and drain into the chin or submandibular area.1 They can also arise on the nose, nasolabial folds, and inner canthus of the eyes. A punctum is usually present. Pus can often be drained from the site with gentle pressure.2
Palpation of the cheek, lips, and orobuccal mucosa may demonstrate a firm indurated cord, which represents the sinus tract. A plain radiograph of the jaw may reveal the infected tooth or bone. When possible, the drainage should be sent for culture.4 Treatment of dental sinuses involves root canal of restorable teeth or extraction of unrestorable teeth. Surgical debridement may be necessary. Antibiotics may be used as an adjunct.1 The fistula typically closes within five to 14 days of treatment. If the fistula does not close, surgical excision and debridement of the cutaneous sinus may be necessary.5
A skin biopsy would be appropriate to evaluate for cutaneous neoplasm or to clarify a diagnosis. Biopsy of an orocutaneous fistula is unnecessary and would typically lead to a recurrence.1
Another course of antibiotics may improve the appearance of an orocutaneous fistula, but it would likely not be sufficient to control the source of the infection.
Salicylic acid is a topical keratolytic used to treat calluses, corns, warts, and molluscum contagiosum. It is not appropriate for the treatment of a dental sinus.
Topical benzoyl peroxide 5% wash and tretinoin 0.05% cream would be an appropriate treatment regimen for mild to moderate acne vulgaris. The combination would not benefit a dental sinus.
The opinions and assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the U.S. Navy, the U.S. Department of Defense, or the U.S. government.
