A 17-year-old baseball player presented with pain, bruising, and swelling in his knee 10 days after he injured his left upper leg by dragging his knee and anterior thigh while sliding into home plate. He was able to continue playing after the injury but later developed knee swelling with increasing firmness in the area. He also reported subjective weakness in his quadriceps.
Ice, compression, and ibuprofen provided some relief. He had no history of knee locking, clicking, catching, or instability and had no numbness or tingling. He did not have a previous injury.
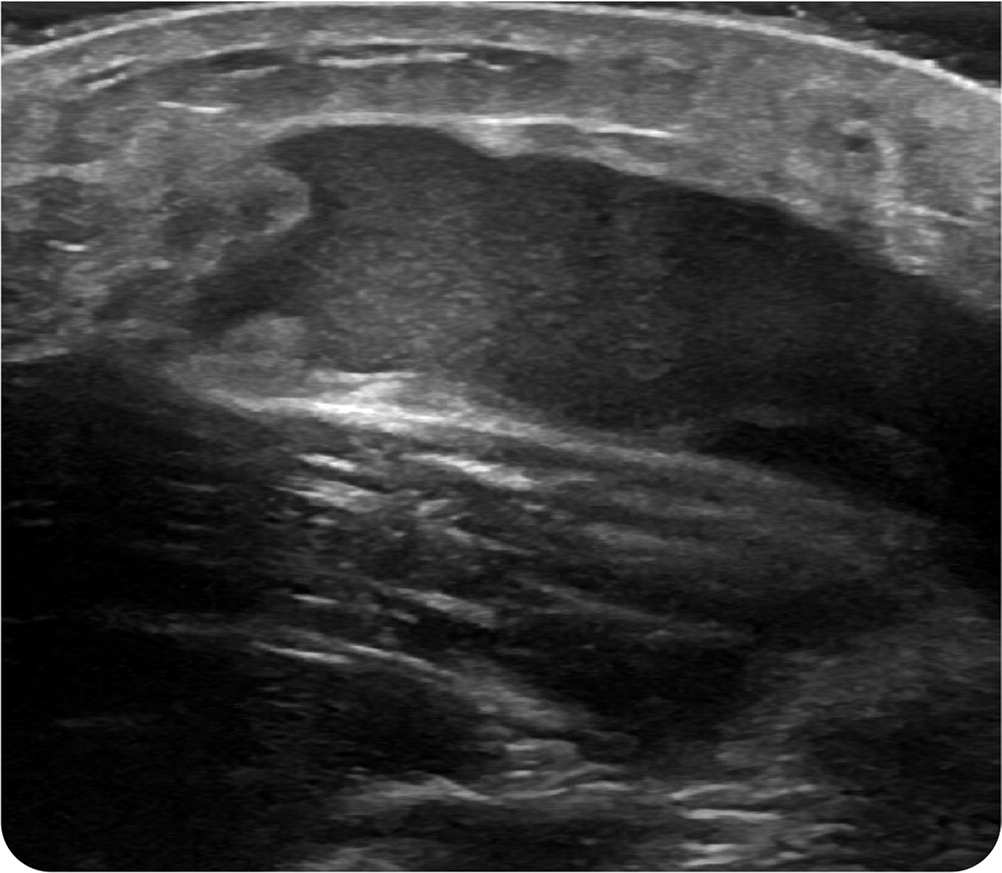
Physical examination revealed swelling over the distal quadriceps tendon and bruising along the anterior and medial aspect of the knee (Figure 1). There was tenderness on palpation over the quadriceps tendon and its insertion into the patella. Quadriceps strength was 5/5 with flexion and extension, although he reported some discomfort with flexion beyond 100 degrees. Radiographic findings were normal. Point-of-care ultrasonography was performed (Figure 2).
FIGURE 1

FIGURE 2
Question
Based on the patient's history, physical examination, and imaging findings, which one of the following is the most likely diagnosis?
A. Morel-Lavallée lesion.
B. Prepatellar bursitis.
C. Quadriceps tendon tear.
D. Septic arthritis.
Discussion
The answer is A: Morel-Lavallée lesion. These lesions are closed degloving injuries in which the subcutaneous tissue separates from the underlying musculature, creating a space that fills with blood, necrotic fat, and lymphatic fluid.1 A peripheral fibrous capsule eventually develops around the lesion, causing firmness on palpation.1,2
A shearing force is the usual mechanism of injury. Hours after initial injury, patients typically develop swelling, tenderness, and bruising that can persist for months unless appropriately treated. Delayed diagnosis can increase complications such as necrosis, infection, and disfigurement.2 Definitive diagnosis of a Morel-Lavallée lesion is made with magnetic resonance imaging2; however, point-of-care ultrasonography is increasingly being used to aid in the diagnosis and to quantify the fluid collection.
This patient's ultrasound findings (Figure 2) showed a heterogenous fluid collection that was 6 × 6 cm in size, with some solid components within the fluid pouch and rough borders of fat overlying the distal quadriceps tendon. Small lesions such as this (typically less than 50 mL) can be managed with compression and/or percutaneous aspiration.3,4 Larger lesions often require surgical intervention.3
Prepatellar bursitis is characterized by swelling and tenderness over the patellar tendon or anterior patella and evidence of fluid collection in the prepatellar bursa. It is typically caused by a direct blow or repetitive trauma to the knee.5
A quadriceps tendon tear typically occurs with a sudden and strong quadriceps contraction, such as when landing from a jump or quickly changing direction. Patients with this injury may report feeling or hearing a pop, and immediate swelling and tenderness develops at the superior border of the patella. Quadriceps weakness on leg extension may also occur. Because complete tendon tears are associated with avulsion fractures of the patella, radiography of the knee should be performed to rule out associated bony injury. Further imaging with magnetic resonance imaging or ultrasonography is recommended.6
Septic arthritis presents as a single warm, painful, swollen joint. It is accompanied by symptoms of systemic infection such as fevers, chills, or malaise. Positive results on Gram stain and culture of aspirated synovial fluid confirm the diagnosis.7
SUMMARY TABLE
| Condition | Characteristics | Diagnosis | Mechanism of injury |
|---|---|---|---|
| Morel-Lavallée lesion | Persistent swelling, tenderness, and bruising; formation of a fibrous capsule may eventually cause firmness on palpation | Magnetic resonance imaging, point-of-care ultrasonography | Shearing force injury |
| Prepatellar bursitis | Localized swelling and tenderness over the prepatellar bursa (superficial to the patella or patellar tendon) | Physical examination, ultrasonography | Direct blow or repetitive trauma to the knee |
| Quadriceps tendon tear | Associated with tenderness over the distal aspect of the quadriceps tendon and superior aspect of the patella, as well as quadriceps weakness | Plain radiography, magnetic resonance imaging, ultrasonography | Sudden and strong quadriceps contraction, such as when landing from a jump or quickly changing direction |
| Septic arthritis | Single warm, painful, swollen joint; symptoms of systemic infection, such as fever, chills, or malaise | Gram stain and culture of aspirated synovial fluid | No injury |
