
A written policy, systematic process, and simple tools can help you to prescribe opioids safely and securely.

Physicians are often reluctant to prescribe opioids for patients with chronic pain despite initiatives to promote evaluation and treatment and even the development of national pain management guidelines.1 Among their concerns are the potential for patient addiction, medication tolerance, physical dependence, and the possibility of abuse, misuse, or diversion of opioid medications. This last area is a growing problem as 4.9 million people 12 years or older were nonmedical users of pain relievers in 2012, and the growth rate of new nonmedical users of pain medication is second only to marijuana.2 Concerns about patient safety and the potential for regulatory sanctions led to growing interest in discontinuing chronic opioid therapy prescribing in our 24-provider urban family medicine clinic, which is affiliated with the University of Michigan Health System's Department of Family Medicine. The clinic team agreed that creating a controlled substance policy was in order. Establishing policy and procedures would minimize differences between individual providers' approaches to chronic pain management and the associated confusion that we feared made it easier for misuse and abuse to fly under the radar. We also believed it would enhance our ability to educate resident physicians about chronic pain management.
A work group of staff from all five of the department's community-based family medicine clinics began developing an opioid monitoring process for eventual use department-wide. This article describes the components of our systematic, patient-centered approach for treating patients with chronic pain, which can be adopted in other primary care settings.
Evaluation protocol
We follow a multi-step process for evaluating any patient considered a candidate for chronic opioid therapy. (See “Clinic flow diagram.”) The patient is given a copy of our policies for treating chronic pain and prescribing opioid medication and a controlled substance agreement, which he or she must sign. In addition, we obtain a urine drug screen and a report from the state of Michigan listing what controlled substances, if any, have been prescribed for the patient within the past year. It is also our policy that new patients must provide medical records from previous doctors. Once we have received and reviewed the patient's lab work, report, and medical records, we are able to make an informed decision as to whether a patient is eligible to receive chronic opioid therapy in our office.
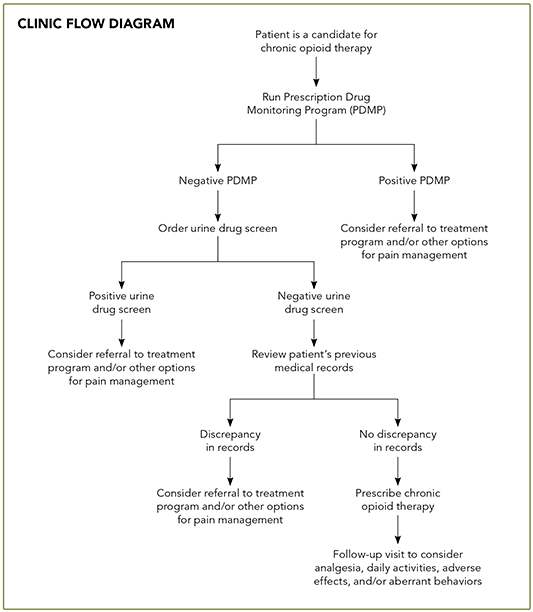
CLINIC FLOW DIAGRAM
Chronic pain and opioid medication policies
Our Chronic Pain and Opioid Medication Policies were developed by a committee that included at least one physician champion per site as well as various other staff members, including clinic managers, nurses, and medical assistants. The committee garnered input from clinic staff and administrators in establishing policies designed to foster a therapeutic physician-patient relationship and reduce stress for clinical staff.
The document states that most patients will need to come in for a visit every one to three months, although the frequency of visits is ultimately at the discretion of the physician. In addition, we stipulate that prescriptions are written to last until the next office visit and refills are generally not provided over the phone unless pre-arranged and documented by a physician in the medical record. The document also states that lost or stolen prescriptions or medications are not replaced and that we expect patients to comply with other recommended medical treatments, including consultations and imaging studies. Patients are given a hard copy of these policies to review annually.
The University of Michigan Health System has its own set of chronic pain guidelines, which serve as an adjunctive resource for managing patients who receive chronic opioid therapy. The guidelines include several helpful tools, such as a sample controlled substance agreement and clinic policy in addition to a selected medication table that includes dosages and cost information. The appendices attached to the university's guidelines provide several helpful tables to guide opioid discontinuance and assess opioid risk.
CHRONIC PAIN AND OPIOID MEDICATION POLICIES
Before your doctor first decides to prescribe opioid pain medications for you, we will need medical records from your previous doctors and a urine drug screen. We will also obtain a report from the state that shows which controlled substances, if any, have been prescribed for you in the past year. We require these items in order to make good decisions about your treatment.
Please note that at least once a year you will need to provide a urine sample. We will also obtain a report from the state, at least once yearly, that outlines the prescriptions you have received from pharmacies.
As part of your opioid treatment plan, we will require that you sign a controlled substance agreement once a year. Please read this agreement carefully, as it has useful and detailed information that is not discussed in this policy letter.
To provide you with the best possible care, we will need to monitor your prescriptions. This will be done during scheduled office visits. Most patients will need to be seen at least every one to three months.
Your prescriptions will be written to last until your next visit. If you have a problem with your condition between office visits, you should schedule an office visit with your health care provider at that time. Please note that opioid prescription refills will not be given over the phone unless you have arranged this ahead of time with your doctor. Any medications that are lost or stolen will not be replaced.
Additionally, you will be expected to use other medical treatments to improve your pain. It may not be possible to completely remove all of your pain. However, our goal in many cases is to return your functionality to an accepted level. Your health care team is able to provide the best treatment for you if we have good communication. You and your health care providers should be respectful of each other for treatment to continue.
YOUR RESPONSIBILITIES
- Give a urine sample when asked.
- Have your medical records sent to us.
- Come to all of your appointments.
- Work with your doctor on other ways to improve your pain.
OUR RESPONSIBILITIES
- Listen and respond to you.
- Keep good track of your medications.
- Work with you to maximize your functionality.
Patient pain questionnaire
A pain questionnaire helps physicians gather objective information from patients who present for visits to discuss their chronic pain. Although their use is not required in our practice, pain questionnaires have proven to be useful tools for physicians who aren't comfortable initiating or managing chronic pain medication by providing a framework for the office visit. In our system, most physicians use the University of Michigan Pain Disability Index and Oswestry Low Back Pain Scale Questionnaire.3,4 Medical assistants can also administer the questionnaires, depending on the office protocols in place. The physician is then able to review and discuss the responses with the patient during the visit and use them to help guide medication management decisions. At the end of the office visit, the completed questionnaire may be scanned into the patient's medical record or recycled in a confidential manner. The questionnaire also may be used as a teaching tool in working with resident physicians and medical students.
Risk assessment tools
Numerous tools are available for physicians to assess a patient's risk for addiction or misuse and determine which patients are good candidates for chronic opioid therapy. For example, the Screener and Opioid Assessment for Patients in Pain (SOAPP®) is a 14-item, self-administered questionnaire.5 Each item is worth up to four points, and a score of eight or greater indicates a high risk of opioid abuse. The Opioid Risk Tool is also a self-administered questionnaire with five items.6 Scores less than three indicate low risk for aberrant behaviors, and scores greater than or equal to eight are high risk. These are just two of several tools available for assessing risk.7
Controlled substance agreement
A controlled substance agreement is an essential part of our process because it not only informs patients about the side effects and risks associated with chronic opioid therapy but also requires that patients acknowledge those risks and attest that they understand our policies. A medical assistant or physician gives the patient the policy document and controlled substance agreement for review and signature, puts the signed original in the medical record, and gives the patient a copy. Patients who refuse to sign the agreement are precluded from receiving chronic opioid therapy. (For items to include, see “Essential elements of a controlled substance agreement.”)
ESSENTIAL ELEMENTS OF A CONTROLLED SUBSTANCE AGREEMENT
- Patient name, birthdate, medical record number, and primary care provider
- Common side effects and risks associated with opioid pain medications – including, but not limited to, severe constipation, trouble breathing, and addiction
- Expectations of patient behavior: – Arrive at appointments and lab tests on time
– Bring prescription bottles to appointments
– Participate in urine drug screens
– Comply with recommended therapies and referrals
- Statements acknowledging that: – The physician will check a prescription fill history with the proper monitoring agencies
– The physician may discontinue treatment based on his or her clinical judgment
– Violation of the agreement can result in termination of controlled substance prescription distribution and/or the delivery of patient care services
- Conditions under which the physician or clinic may end the agreement
- Parameters for filling prescribed medications, for example: – Prescriptions only distributed by the primary prescribing doctor's office
– No controlled-substance prescriptions from on-call doctors
– No refills given outside of normal clinic hours
– Length of time required to process refills
– Contact information for pharmacy where prescriptions may be filled
– Individual authorized to pick up the prescription from the clinic (ID required)
Urine drug screen
We conduct urine drug screens annually. This allows the physician to determine if the patient is taking any other substances, prescribed or illicit, which might interfere with a therapeutic physician-patient relationship. Presence of these substances in the urine might signify that a patient is receiving controlled substances from multiple providers or engaging in substance abuse. Also, an absence of prescribed substances might signify prescription medication misuse, such as illegal distribution of prescription drugs. Although the specific management of these situations is handled case-by-case, the test results may require termination of the controlled substance agreement in addition to referral to a mental health provider who specializes in substance abuse.
Prescription drug monitoring
State-level prescription drug monitoring support is provided to clinic physicians through the Michigan Automated Prescription System (MAPS), an automated system for collecting prescription information on Schedule II–V controlled substances. Prescription data collected by pharmacies and dispensing providers are securely stored in a centralized MAPS database and used to determine if patients are receiving controlled substances from other providers.
Almost all states have a similar program. The National Association of State Controlled Substances Authorities has a list of resources. In our department, medical assistants retrieve the reports for the physicians at least once a year, but any staff member can theoretically run the reports once registration with the program is complete. Physicians may review the reports at any time in the office. The reports can then be scanned into the medical record or destroyed in a confidential manner, similar to any medical record.
Our practice's electronic health record (EHR) prompts us to run the drug monitoring database report, perform an annual review of the controlled substance agreement, and order any necessary drug screenings. Prior to implementing our EHR in 2012, we used a stand-alone clinical decision support system that provided the same functionality. Regardless of method, it is important to have a system with automated prompts relevant to opioid monitoring for patients with chronic pain.
Follow-up chronic pain visits
At follow-up visits, physicians can again use pain questionnaires to assess the patient's level of pain and functional status. Physicians can also inquire about adverse effects of treatment. If pain is inadequately controlled but the patient doesn't report any adverse effects, physicians may decide to adjust the dosage of chronic opioid therapy, add nonopioid pain medications, or refer the patient to other professionals such as pain psychologists, physical therapists, or pain management specialists. In addition, physicians may discuss the results of ongoing state-level prescription drug monitoring reports and urine drug screens at these follow-up visits.
Keeping it going
Implementing an opioid monitoring process for patients with chronic pain does not need to be expensive or complicated. (See “Opioid medication policy: a real-world example.”) Using the materials and resources included in this article can help you to get started. Physicians in our clinic have reported that our approach has helped improve the quality of care delivered to non-cancer patients suffering from chronic pain and has made overall workflow more efficient.
Because of retirements, employee job changes, and residency graduations, additional and ongoing education of our clinic team will be required to support long-term improvement efforts. It is our intention to continue with post-implementation monitoring as a way of assessing longer-term gains in practice improvement.
OPIOID MEDICATION POLICY: A REAL-WORLD EXAMPLE
MJ is a 45-year-old new patient who presents to your office for management of his chronic back and leg pain. He is a mechanical engineer who suffered a fall five years ago, which resulted in a herniated lumbar disc. Multiple lumbar surgeries were performed, culminating in an L4-S1 fusion. The patient has moderately severe back pain (7 to 8 out of 10) with right-sided radicular symptoms. He reports a previous diagnosis of a failed back syndrome.
During the course of your risk assessment, he scores a 10 on your opioid risk tool, which you interpret to suggest a high risk for aberrant behavior. To determine whether you will be able to prescribe chronic opioid therapy for this patient, you inform him that you will need to request a report through your state's prescription monitoring program, obtain a urine drug screen, and request his medical records from his previous physician. Unfortunately, the state program reports opioid prescriptions from multiple physicians in the state and the urine tests positive for cocaine. At his follow-up visit, you inform him that your office will not be able to prescribe chronic opioid therapy for him. You offer to treat him with nonopioid therapy and refer him to a local substance abuse program.
