
How will this emerging trend take shape? Is it good for medicine – for doctors? And will there still be a place for independent physicians?
If you have been monitoring the anecdotal evidence lately, you may be under the impression that the employment of physicians is universal in the United States and independent physicians (i.e., those who own their practices) have gone the way of the dinosaur. This perception, while not accurate, is not implausible either.
Yes, there are still physicians in America who own their own shops, hire their own personnel, pay their own bills, manage to earn a profit, and are happy doing so. However, these hardy individuals are in fact dwindling in numbers, and although the physician employment trend has not swept the board entirely, it is real and increasingly prevalent. This article will explore how prevalent physician employment is, its pros and cons, and whether there is still a place for independent physicians.
What the surveys show
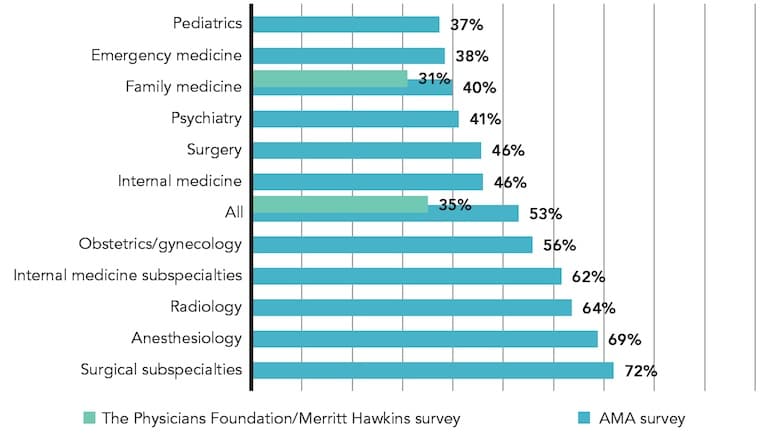
The American Medical Association reported in its 2012 Practice Benchmark Survey that a slight majority (53 percent) of physicians owned their practices, down from 61 percent in 2007/2008; 42 percent of physicians were employees, and 5 percent were independent contractors.1 The percentage of physicians who identified as practice owners varied widely across specialties, from a high of 72 percent for surgical subspecialties to a low of 37 percent for pediatrics. For family medicine, the percentage of physicians who owned their practices was 40 percent; 58 percent of physicians were employed, and 3 percent were independent contractors. (See “Physicians as owners by specialty.”)
PHYSICIANS AS OWNERS BY SPECIALTY
Sources:
Kane CK, Emmons DW. Policy Research Perspectives: New Data on Physician Practice Arrangements: Private Practice Remains Strong Despite Shifts Toward Hospital Employment. Chicago: American Medical Association; 2013. http://www.ama-assn.org/resources/doc/health-policy/x-pub/prp-physicianpractice-arrangements.pdf.
Survey of America's Physicians: Practice Patterns and Perspectives. Boston: The Physicians Foundation/Merritt Hawkins; 2014.
More recent data from the September 2014 Survey of America's Physicians: Practice Patterns and Perspectives, conducted by Merritt Hawkins for The Physicians Foundation, indicate that only 35 percent of all physicians identify as independent.2 Among family medicine physicians, the rate drops to 31 percent. These numbers vary by region, with some states remaining relative bastions of independent practice while others are dominated by the employed physician model. (See “Independent physicians by state.”)
INDEPENDENT PHYSICIANS BY STATE
| TOP 10 | BOTTOM 10 | ||||
|---|---|---|---|---|---|
| 1 | Louisiana | 52% | 41 | Vermont | 24% |
| 2 | Texas | 49% | 42 | Minnesota | 23% |
| 3 | New Jersey | 45% | 43 | Massachusetts | 23% |
| 4 | Illinois | 44% | 44 | Alaska | 19% |
| 5 | Arkansas | 43% | 45 | Indiana | 19% |
| 6 | Hawaii | 42% | 46 | New Mexico | 18% |
| 7 | Idaho | 42% | 47 | New Hampshire | 18% |
| 8 | Arizona | 39% | 48 | South Dakota | 17% |
| 9 | Utah | 38% | 49 | Wisconsin | 12% |
| 10 | Tennessee | 38% | 50 | North Dakota | 7% |
Source: Survey of America's Physicians: Practice Patterns and Perspectives. Boston: The Physicians Foundation/Merritt Hawkins; 2014.
The rate of independent vs. employed practice also varies by physician age. According to the same study, 66 percent of physicians 45 years old or younger identify as employed, compared with only 26 percent of those age 46 and older.2
Back to the future
For physicians who were in practice in the 1990s, the growing prevalence of the employed physician model will seem familiar. As in the '90s, hospitals and other entities are buying practices and employing physicians as a way to achieve efficiencies associated with system-wide integration, manage large population groups, and better position themselves for value-based or bundled payments. Although the integration in the '90s often ended in disintegration, with many hospitals later selling off the practices they had bought, this latest effort appears to have some differences.3 For example, there is now a greater emphasis on reaching quality goals and expanding information technology to support the work.
Family physicians are the linchpin of these efforts because they provide critically important care coordination, ensuring quality requirements are met while resources are used appropriately. And although the health system is moving toward value-based payment, volume is by no means an obsolete payment metric. According to Merritt Hawkins' 2013 Inpatient/Outpatient Physician Revenue Survey, family physicians generate an average of more than $2 million per year on behalf of their affiliated hospitals through admissions, prescriptions, tests, and procedures.
That is a primary reason why hospitals continue to employ physicians, even though a recent study commissioned by the Kentucky Hospital Association indicates that 58 percent of hospitals reported losing more than $100,000 annually per employed doctor. Though they may be in the red on physician contracts, hospitals often make up the difference through the downstream revenue physicians generate. In addition, hospitals have become better at monitoring physician productivity and are quicker to adjust physician compensation accordingly, or terminate physicians if their productivity falls below stipulated levels.
Another difference from the last employment go-round is that the types of entities employing physicians are proliferating and now extend far beyond traditional acute care hospitals. The most rapidly growing sites of service, including urgent care centers, retail clinics, surgery centers, Federally Qualified Health Centers, large employers, academic medical centers, and insurance companies, all use the employed model.
This trend is reflected in the physician search assignments Merritt Hawkins conducts. In 2014, more than 90 percent of our 3,158 searches featured employment of the physician, whether by a hospital, medical group, or any of the other entities referenced above. Fewer than 10 percent featured a true independent setting, down from more than 45 percent in 2004.
Pros and cons
Generalizing about the pros and cons of employed practice, or any practice type, is difficult because of the variety of experiences. For example, a 55-year-old employed physician who recently sold his small practice to a hospital yet still works in the same office with the same staff might have a vastly different experience than a 35-year-old employed physician who has worked for a large health system since day one after residency.
In either setting, however, employed practice does tend to have certain advantages over independent practice. Namely, employed practice often gives physicians income security, more predictable work hours, and relief from many of the hassles of running a practice.
Interestingly, though, employed practice does not necessarily lessen physicians' nonclinical workload. According to The Physicians Foundation survey, employed and independent physicians spent 10.6 hours and 9.8 hours, respectively, on nonclinical paperwork.2
Another potential advantage of employed practice is that it gives interested physicians an opportunity to influence a larger organization that, conceivably, has a larger impact on the health care system. Particularly in this time of great change in health care, it is invaluable for organizations to have physician input and leadership.
Despite its advantages, the employed model does not have the enthusiastic endorsement of all physicians, even among those who are employed. In The Physicians Foundation survey cited previously, 63 percent of physicians said they do not believe the employment of physicians by hospitals is a positive trend likely to enhance quality of care and decrease costs.2 Even a slight majority of employed physicians (51 percent) indicated they do not believe hospital employment of physicians is a positive trend.
One potential downside of the employed model is an increase in physician turnover, which can erode continuity of care. Employed physicians may not have the same financial and emotional stake in their practices as do independent physicians, making it relatively easy for them to move on as practice conditions or other opportunities dictate. The physician data company SK&A estimates that the annual relocation rate is 14 percent for family physicians, a turnover rate that can be disruptive to employers and patients alike.
The employed model also may exacerbate growing shortages among primary care physicians. The Physicians Foundation survey indicates that physicians saw an average of 23.4 patients per day in 2008 and 19.5 patients per day in 2014, a decline of 17 percent.2 Physician hours worked per week also declined, from 56.9 hours per week in 2008 to 52.8 hours per week in 2014. This represents a 6 percent decline in overall physician FTEs, or a loss of about 45,000 physicians from the workforce. Some of this decline may be linked to the rise in physician employment because employed doctors typically work set schedules and see fewer patients than independent physicians. The Physicians Foundation survey found that employed physicians see 1.7 fewer patients per day on average than independent physicians, a small difference that can add up to large numbers of patients over the course of a year.
Another common concern is that employed physicians have less clinical autonomy than their colleagues in independent practice. However, The Physicians Foundation survey found little difference between the two groups; 68 percent of employed physicians and 71 percent of independent physicians indicated at least some limitations on their clinical autonomy.2
An additional, more subjective concern is the effect of physician employment on the nature of the medical profession. Will physicians be less likely to take ownership of their patients' health and be fully engaged patient advocates if they are financially beholden to large, corporate organizations? Will medicine cease being a calling and become in effect a trade? These concerns may not ultimately prove valid but are worthy of reflection as medicine continues to evolve.
Staying independent
Although the physician practice landscape is changing, avenues still exist for physicians who wish to retain their independence. In fact, being small and independent may be an advantage when it comes to making decisions, getting buy-in, and implementing changes. One of the keys to future success for independent practices will be continuing to refine and upgrade their practice methods, such as contracting out billing and collections, collecting copayments and deductibles at the time of service, fully utilizing existing staff, and implementing automated patient scheduling and appointment reminder systems. They may also need to build additional revenue streams, for example, by incorporating nurse practitioners and physician assistants who can increase patient volume and extend available hours or by adding new services such as wellness programs.
Physicians seeking to navigate the ever-growing performance-based payment system while staying independent should look for local partners. For example, the Texas Medical Association and Blue Cross/Blue Shield of Texas recently launched a support service that enables physicians to provide coordinated, collaborative care and perform like an accountable care organization (ACO) without being employed by a larger entity. Similarly, independent practices can join independent practice associations or merge with other practices to form ACOs, provide the strength in numbers needed to negotiate favorable contracts, and reduce the cost of information technology, personnel, and other support systems while preserving their autonomy.
It may also be possible for an independent physician to align with a hospital without being employed. The physician enterprise model, also known as “practice leasing,” is an arrangement in which a hospital operates a medical practice at a fixed percentage of collections. This allows the practice to use the hospital or hospital system's back office for contracting, coding, and billing on a fee basis while preserving its private practice autonomy. For example, through more efficient management, a hospital might be able to increase a two-physician practice's collections from $1 million to $1.1 million and reduce its overhead from $500,000 to $450,000, increasing physician income from $250,000 to $325,000. This type of arrangement is easier to undo if necessary than, say, a practice acquisition.
Some physicians are finding it easier to maintain their independence by converting to a direct primary care or concierge model, in which third-party payments are reduced or eliminated and patients pay directly for their primary care needs. In The Physicians Foundation survey, 7 percent of physicians indicated they now practice some form of concierge medicine while 13 percent said they are planning to transition in whole or in part to this model.2 (See “Physicians practicing or intending to practice some form of concierge medicine by state.”)
PHYSICIANS PRACTICING OR INTENDING TO PRACTICE SOME FORM OF CONCIERGE MEDICINE BY STATE
| TOP FIVE | BOTTOM FIVE | ||||
|---|---|---|---|---|---|
| 1 | Wyoming | 38% | 46 | Oregon | 11% |
| 2 | Nevada | 31% | 47 | Wisconsin | 11% |
| 3 | Louisiana | 29% | 48 | Nebraska | 9% |
| 4 | Florida | 29% | 49 | Delaware | 9% |
| 5 | Texas | 29% | 50 | Vermont | 4% |
Source: Survey of America's Physicians: Practice Patterns and Perspectives. Boston: The Physicians Foundation/Merritt Hawkins; 2014.
Where there's a will
In the 1990s, the decline of independent practice was generally seen as a fait accompli, a perspective that has returned to health care today, and for many good reasons. The employed physician model is not going away in part because many physicians, overwhelmed by the costs and pressures of private practice, are seeking employment as a refuge, and because the market is pushing for greater integration. That said, it is still too early to close the book on independent practices, particularly those that are agile and willing to adapt and innovate. Where physicians have the will to maintain their autonomy, they will almost certainly find a way.
