
Learn about the new skin biopsy codes, and follow these tips to make sure you get full credit for the skin procedures you perform.

It is often easier for family physicians to perform skin procedures than it is to correctly code for them. The codes are complicated, and many electronic health record systems and even the CPT manual use different terms than physicians use to describe these services. Incomplete or unclear documentation can lead to submitting lower-valued codes, which not only reduces practice revenue but also lowers physicians’ work relative value units (wRVUs), affecting their productivity-based compensation.
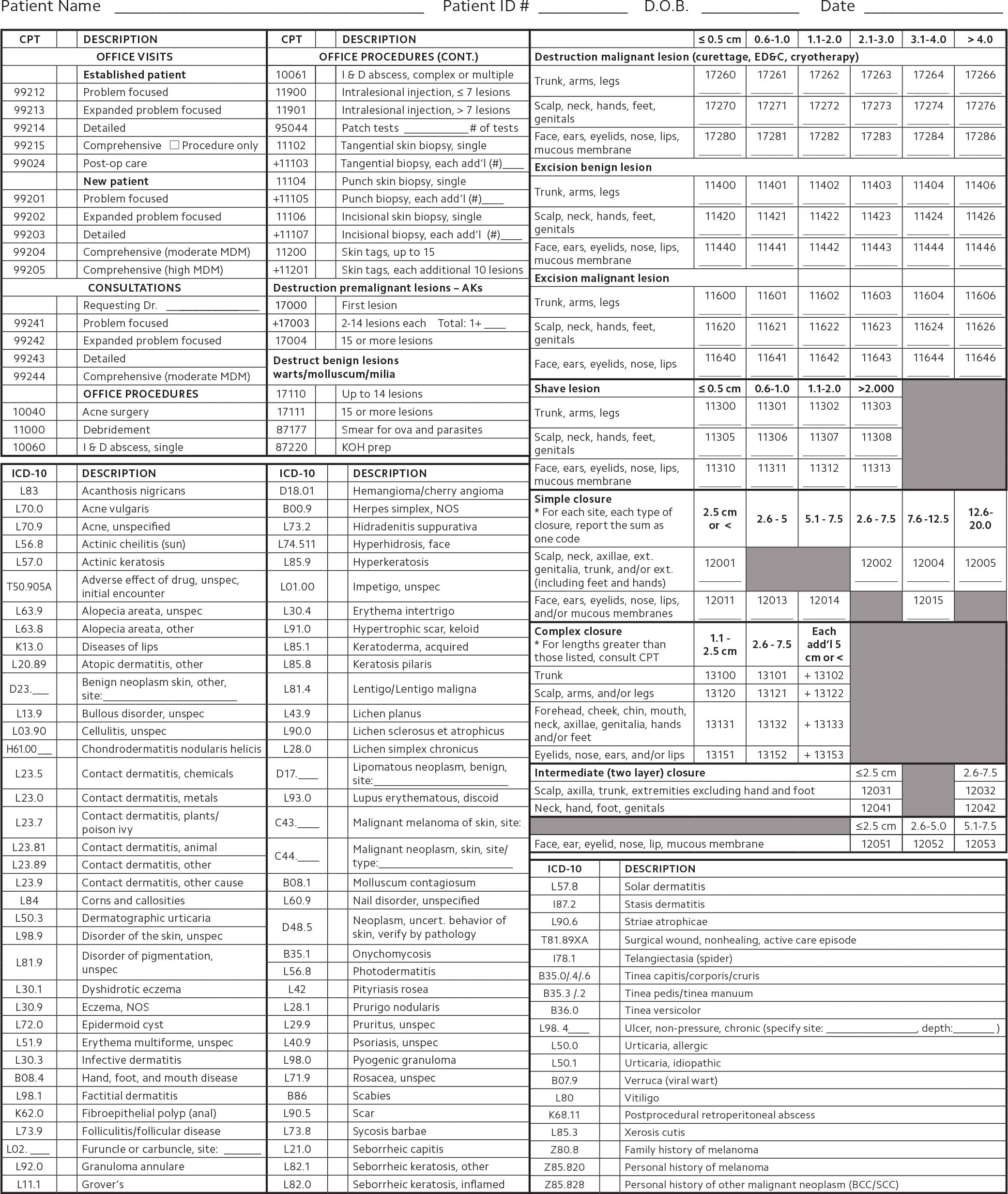
Correct coding for skin procedures is not impossible. This article will detail how to code for two types of common skin procedures — biopsies and destruction of lesions — as well as how to code when multiple skin procedures are performed on the same day. The “Skin care encounter form” features codes for the skin procedures most commonly performed by family physicians.
KEY POINTS
- CPT created new codes in 2019 for tangential, punch, and incisional biopsies and deleted two old biopsy codes.
- Codes for shave and excisional biopsies, as well as destruction of benign, premalignant, and malignant lesions and skin tags, have not changed.
- When performing multiple skin procedures for the same patient on the same day, report the highest-valued code first, without a modifier.
PERFORMING BIOPSIES USING THE 2019 CODES
CPT deleted skin biopsy code 11100 and add-on code 11101 this year and introduced three base codes and three add-on codes that are defined by the method of biopsy — tangential, punch, or incisional — rather than size or anatomic location. (See “New biopsy codes.”) Simple closure, when needed, is included in the payment for all three biopsy types and should not be billed separately. If you need to manipulate the wound to get the edges to align, that is also not separately billable.
NEW BIOPSY CODES
| CPT code | Description | wRVU | Total nonfacility RVUs | Global days |
|---|---|---|---|---|
| 11102 | Tangential biopsy of skin (e.g., shave, scoop, saucerize, curette), single lesion | 0.66 | 2.80 | 0 |
| +11103 | Each additional lesion | 0.38 | 1.51 | N/A |
| 11104 | Punch biopsy of skin (including simple closure, when performed), single lesion | 0.83 | 3.52 | 0 |
| +11105 | Each additional lesion | 0.45 | 1.73 | N/A |
| 11106 | Incisional biopsy of skin (e.g., wedge; including simple closure, when performed), single lesion | 1.01 | 4.26 | 0 |
| +11107 | Each additional lesion | 0.54 | 2.04 | N/A |
Tangential biopsies (codes 11102–11103), which include shave, scoop, saucerization, or curette techniques, are performed with a sharp blade and remove a sample of epidermal tissue, with or without a portion of the underlying dermis. These are not considered excisional biopsies, which remove the entire lesion with margins.
Punch biopsies (codes 11104–11105) use a punch tool to remove a full-thickness cylindrical sample of the skin.
Incisional biopsies (codes 11106–11107) use a sharp blade to remove a full-thickness sample of tissue via a vertical incision or wedge, penetrating deep to the dermis and into the subcutaneous space. This method may sample subcutaneous fat.
When multiple biopsies are performed for the same patient on the same date, only one primary biopsy code may be reported, depending on the following:
- If multiple biopsies are performed using the same technique, report the primary code with the highest RVUs, then use the corresponding add-on code for the other biopsies.
- If multiple biopsies are performed using different techniques, report the primary code with the highest RVUs, then use the add-on code that is specific to the other biopsies performed.
When billing for these services, record the method and the number of units in your documentation. Although the location of the biopsy is not required to select a code, you should document it as well. An example of coding for multiple biopsies is shown below.
CPT left unchanged the codes for shave biopsies and excisional biopsies of benign or malignant lesions. Here are some reminders for those codes.
Shave biopsies (codes 11300–11313) use a sharp instrument to remove epidermal or dermal lesions without a full-thickness excision. They are used for therapeutic removal when the lesion is symptomatic, such as rubbing on a waist band or bra line. Shave biopsy codes are selected based on the location and size of the lesion. Simple closure, if needed, is included in the procedure and is not separately billable. Be sure to document the location and size of each lesion.
Excisional biopsies include two sets of codes, for excision of benign lesions (codes 11400–11471) or malignant lesions (codes 11600–11646). These codes are for full-thickness removal and should be selected based on the lesion type, the location, and the size of the excision, not the size of the lesion itself. The excision size is the largest diameter of the lesion plus twice the narrowest margin required to remove the lesion. Because excision code selection depends in part on lesion type, you must wait to submit the claim until after you receive the pathology report. For all other biopsies, you may submit the claim at the time of service. Excision codes include simple wound repair, so this should not be reported separately. Layered closures may be billed separately, although the Centers for Medicare & Medicaid Services (CMS) does not pay for it in these cases. Again, be sure to document the size and location of each lesion, as well as the type.
DESTRUCTION OF BENIGN, PREMALIGNANT, AND MALIGNANT LESIONS
There are three sets of CPT codes for destruction of benign and premalignant lesions, as well as a fourth for treating malignant lesions.
Destruction of premalignant lesions (actinic keratoses) should be billed based on the number of lesions. The first should be billed with code 17000, and each additional lesion, up to 14, should be billed with add-on code 17003. The destruction of 15 or more lesions should be billed with a single unit of code 17004.
For the destruction of benign lesions (seborrheic keratoses and warts), bill a single unit of code 17110 to treat up to 14 lesions and a single unit of code 17111 for 15 or more.
Removing skin tags can be tricky as payers may consider the procedure cosmetic and not cover it. Explain this to the patient, and document whether the skin tags are irritated or bleeding. Use a single unit of code 11200 for removing up to 15 lesions, and use add-on code 11201 for each additional block of up to 10 more.
The coding for destruction of malignant lesions is different than for benign lesions. Use a code from the 17260–17286 range for each lesion, and select the code based on the location and size of the lesion, not the defect. These codes include local anesthesia and are used for all destruction methods, including electrosurgery, cryosurgery, laser treatment, and chemical treatment.
Note that more specific codes exist for destruction of benign and premalignant lesions on the mouth (40820), eyelid (67850), conjunctiva (68135), anus (46900–46924), penis (54050–54060), vulva (56501–56515), and vagina (57061–57065), and these codes should be used instead of codes in the integumentary system section of CPT. Destruction of lesions in the genital area may be coded according to whether it is considered simple or extensive, although CPT does not define these terms. Destruction of some genital lesions also are coded based on the method used.
PERFORMING MULTIPLE PROCEDURES ON THE SAME DAY
Multiple skin procedures are often performed at the same patient visit. This leads to questions about bundling and how to use modifiers when billing for more than one procedure on the same day. To bill these correctly and avoid denials, follow three steps:
- Check the total RVUs for each code to determine which is valued highest (CMS provides this information at https://www.cms.gov/apps/physician-fee-schedule/search/search-criteria.aspx).
- Check the National Correct Coding Initiative (NCCI) edits (https://go.cms.gov/2yLPjKp).
- Report the highest-valued code on the claim form without a modifier. If the second procedure is the same as the first or is bundled into the first based on NCCI edits, submit that code too, with modifier 59, “Distinct procedural service.” If the second procedure is not bundled into the first, use modifier 51, “Multiple procedures” (although Medicare contractors may not require modifier 51).
Note that payment amounts may vary when multiple procedures are performed on the same calendar day. The highest valued procedure may be paid at 100 percent, and procedures two through five may be paid at 50 percent. Billing more than five procedures may trigger a manual review by the payer.
Finally, remember to submit a wound repair code if allowed by CPT and, if you addressed an issue in addition to the skin procedures (hypertension, for example), include the appropriate E/M office visit code with modifier 25, “Significant, separately identifiable evaluation and management service.” Most payers will pay for the E/M code, but some have additional edits for skin procedures, making it a challenge to get both the office visit and the skin procedures paid.
Here are some common procedure combinations and how to code for them:
Example 1: Physician performs a punch biopsy and treats three actinic keratoses.
| Procedure | CPT code | Total RVUs |
|---|---|---|
| Punch biopsy | 11104 | 3.52 |
| Destruction of premalignant lesion | 17000-59 | 1.85 |
| Destruction of premalignant lesions (additional) | 17003 17003 | 0.16 0.16 |
The biopsy has the highest RVUs, so it is reported first without a modifier. The first actinic keratosis removal is bundled into 11104, so attach modifier 59. The second two actinic keratosis removals are add-on codes and don’t require a modifier.
Example 2: Physician treats three seborrheic keratoses and one actinic keratosis, and performs an incisional biopsy on a different lesion.
| Procedure | CPT code | Total RVUs |
|---|---|---|
| Incisional biopsy | 11106 | 4.26 |
| Destruction of benign lesion | 17110-59 | 3.13 |
| Destruction of premalignant lesions | 17000-59 | 1.85 |
The treatment of all three keratoses is bundled into the incisional biopsy code, which is listed first because it has the highest RVUs. Attach modifier 59 to the lesion destruction codes to indicate the services involved different lesions.
Example 3: Physician destroys a malignant lesion and performs a punch biopsy on a different lesion.
| Procedure | CPT code | Total RVUs |
|---|---|---|
| Destruction of malignant lesion | 17261 | 4.11 |
| Punch biopsy | 11104-59 | 3.52 |
The punch biopsy is bundled into the destruction of a malignant lesion. Attach modifier 59 to the punch biopsy code to indicate that it was performed on a different lesion. If this had been the same lesion, you would report only the destruction.
Example 4: Physician treats one wart and one actinic keratosis.
| Procedure | CPT code | Total RVUs |
|---|---|---|
| Destruction of benign lesion | 17110 | 3.13 |
| Destruction of premalignant lesion | 17000-59 | 1.85 |
The code with the highest RVUs is reported first. Code 17000 is bundled into 17110, so attach modifier 59 to 17000 to indicate it was a separate lesion.
Example 5: Physician performs an incisional biopsy and a punch biopsy and destroys a single actinic keratosis. All are different lesions.
| Procedure | CPT code | Total RVUs |
|---|---|---|
| Incisional biopsy | 11106 | 4.26 |
| Punch biopsy | 11105 | 1.73 |
| Destruction of benign lesions | 17000-59 | 3.13 |
The procedure with the highest RVUs is reported first without a modifier. When performing two biopsies in the 11102–11107 series with different methods, use the add-on code for the second method — 11105 for the punch biopsy in this example. Add-on codes don’t require a modifier. The benign lesion destruction requires modifier 59 to indicate it was done on a separate lesion.
Of course, this is only a handful of the possible procedures that could be done on the same day. Access to up-to-date RVU and NCCI edit information is essential to correctly bill these procedures.
Documenting and coding skin procedures carefully will result in accurate payment and wRVU assignment.
