CMMI VALUE-BASED PAYMENT MODELS OF NOTE
| Model | Elements that reduce barriers to participation for independent practices |
|---|---|
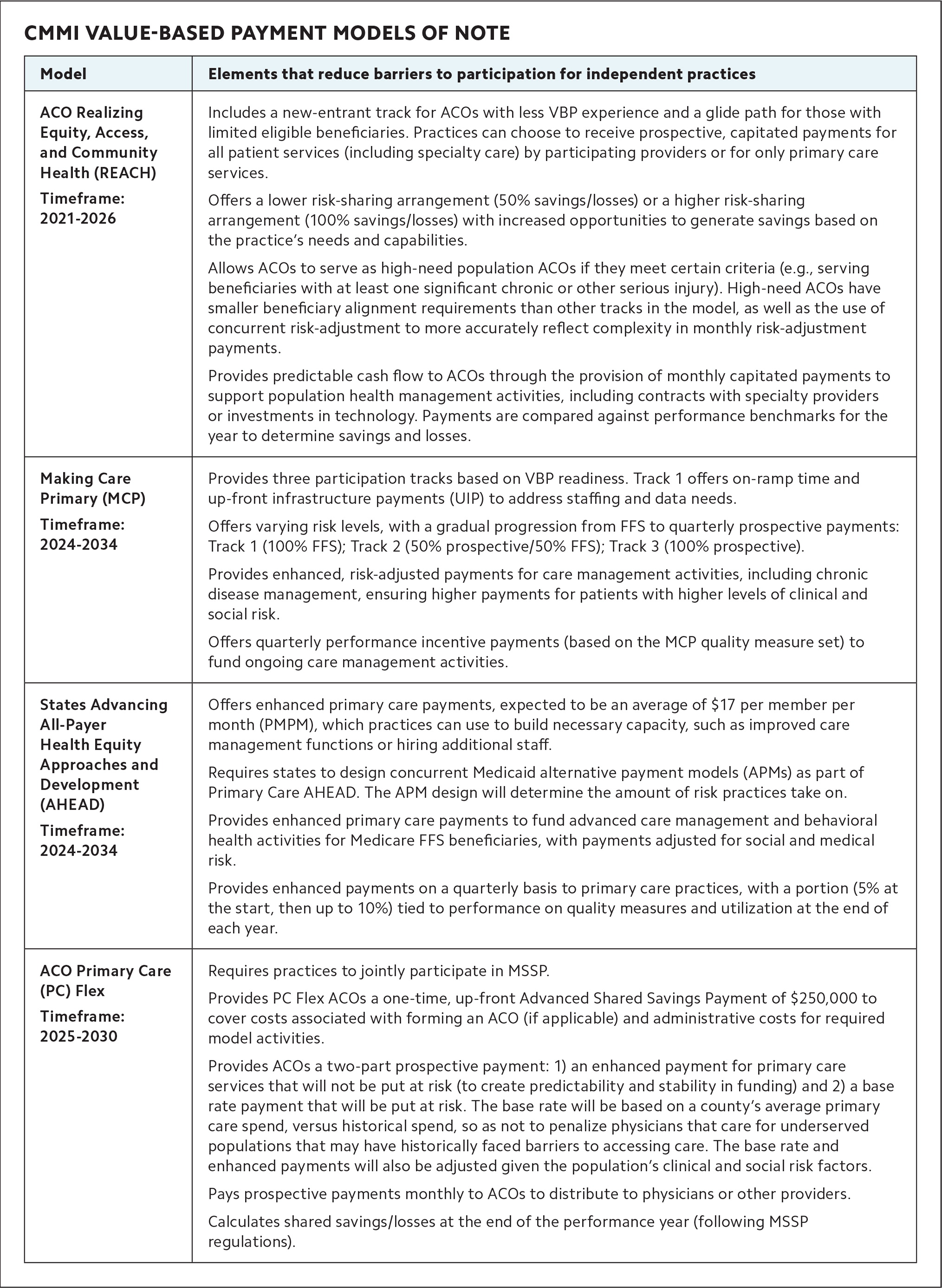
| ACO Realizing Equity, Access, and Community Health (REACH) Timeframe: 2021–2026 |
Includes a new-entrant track for ACOs with less VBP experience and a glide path for those with limited eligible beneficiaries. Practices can choose to receive prospective, capitated payments for all patient services (including specialty care) by participating providers or for only primary care services. Offers a lower risk-sharing arrangement (50% savings/losses) or a higher risk-sharing arrangement (100% savings/losses) with increased opportunities to generate savings based on the practice's needs and capabilities. Allows ACOs to serve as high-need population ACOs if they meet certain criteria (e.g., serving beneficiaries with at least one significant chronic or other serious injury). High-need ACOs have smaller beneficiary alignment requirements than other tracks in the model, as well as the use of concurrent risk-adjustment to more accurately reflect complexity in monthly risk-adjustment payments. Provides predictable cash flow to ACOs through the provision of monthly capitated payments to support population health management activities, including contracts with specialty providers or investments in technology. Payments are compared against performance benchmarks for the year to determine savings and losses. |
| Making Care Primary (MCP) Timeframe: 2024–2025 (was previously 2034) |
Provides three participation tracks based on VBP readiness. Track 1 offers on-ramp time and up-front infrastructure payments (UIP) to address staffing and data needs. Offers varying risk levels, with a gradual progression from FFS to quarterly prospective payments: Track 1 (100% FFS); Track 2 (50% prospective/50% FFS); Track 3 (100% prospective). Provides enhanced, risk-adjusted payments for care management activities, including chronic disease management, ensuring higher payments for patients with higher levels of clinical and social risk. Offers quarterly performance incentive payments (based on the MCP quality measure set) to fund ongoing care management activities. |
| States Advancing All-Payer Health Equity Approaches and Development (AHEAD) Timeframe: 2024–2034 |
Offers enhanced primary care payments, expected to be an average of $17 per member per month (PMPM), which practices can use to build necessary capacity, such as improved care management functions or hiring additional staff. Requires states to design concurrent Medicaid alternative payment models (APMs) as part of Primary Care AHEAD. The APM design will determine the amount of risk practices take on. Provides enhanced primary care payments to fund advanced care management and behavioral health activities for Medicare FFS beneficiaries, with payments adjusted for social and medical risk. Provides enhanced payments on a quarterly basis to primary care practices, with a portion (5% at the start, then up to 10%) tied to performance on quality measures and utilization at the end of each year. |
| ACO Primary Care (PC) Flex Timeframe: 2025–2030 |
Requires practices to jointly participate in MSSP. Provides PC Flex ACOs a one-time, up-front Advanced Shared Savings Payment of $250,000 to cover costs associated with forming an ACO (if applicable) and administrative costs for required model activities. Provides ACOs a two-part prospective payment: 1) an enhanced payment for primary care services that will not be put at risk (to create predictability and stability in funding) and 2) a base rate payment that will be put at risk. The base rate will be based on a county's average primary care spend, versus historical spend, so as not to penalize physicians that care for underserved populations that may have historically faced barriers to accessing care. The base rate and enhanced payments will also be adjusted given the population's clinical and social risk factors. Pays prospective payments monthly to ACOs to distribute to physicians or other providers. Calculates shared savings/losses at the end of the performance year (following MSSP regulations). |