
These simple strategies based on self-determination theory can help you maximize your patients’ motivation to change.

Facilitating patient behavior change is a constant challenge for primary care physicians and other clinicians. According to one estimate, up to 75% of primary care visits involve engaging patients in changing a habit or starting medications.1 Given the time pressure and complex psychosocial dynamics we encounter daily in primary care, it can be daunting to effectively promote behavior changes that will improve health outcomes. Ultimately, the motivation to change must come from patients themselves. The key question is how can we maximize our patients’ motivation to change?
The answer lies in self-determination theory (SDT). By incorporating simple, evidence-based strategies rooted in SDT,2 clinicians can help facilitate behavior change, foster stronger patient relationships, improve patient outcomes, and reduce frustration for both clinicians and patients.
KEY POINTS
- Self-determination theory posits that individuals have three basic psychological needs that are essential for motivation and well-being — autonomy, belonging, and competence.
- By understanding these needs and actively supporting them through simple, evidence-based strategies, clinicians can enhance their effectiveness in helping patients internalize behavior change and achieve lasting results.
- This approach shifts clinical dialogue from “need-thwarting” to “need-supporting.”
WHAT IS SELF-DETERMINATION THEORY?
SDT is a well-established framework for understanding human motivation. It posits that all individuals have an inherent drive to flourish,3 but to reach their full potential, they require certain environmental supports. Specifically, SDT identifies three basic psychological needs that are essential for motivation and well-being:4
- Autonomy — the sense of agency and control in one’s actions and decisions;
- Relatedness — the need for connection, feeling understood and valued by others;
- Competence — the feeling of growth, mastery, and effectiveness in one’s pursuits.
We have adapted these terms and developed a simple “ABC” mnemonic — Autonomy, Belonging, and Competence — to help clinicians remember these core needs and integrate them seamlessly into patient care.
According to SDT, the extent to which these psychological needs are supported or thwarted determines the quality of an individual’s motivation. Motivation can range from fully externally regulated or “controlled” (non-self-determined) to fully internally regulated or “autonomous” (self-determined).
SDT has strong evidence supporting its effectiveness across diverse contexts, including health care.3,5 Research has shown that SDT-based interventions significantly improve behaviors and outcomes that are critical in primary care, such as smoking cessation, physical activity, and healthy eating.6 Clinician techniques that support autonomy have been linked to better health outcomes, enhanced patient engagement, and improved well-being.5,6 These principles align with many of the behavior change techniques already used in primary care (see Table 1).7
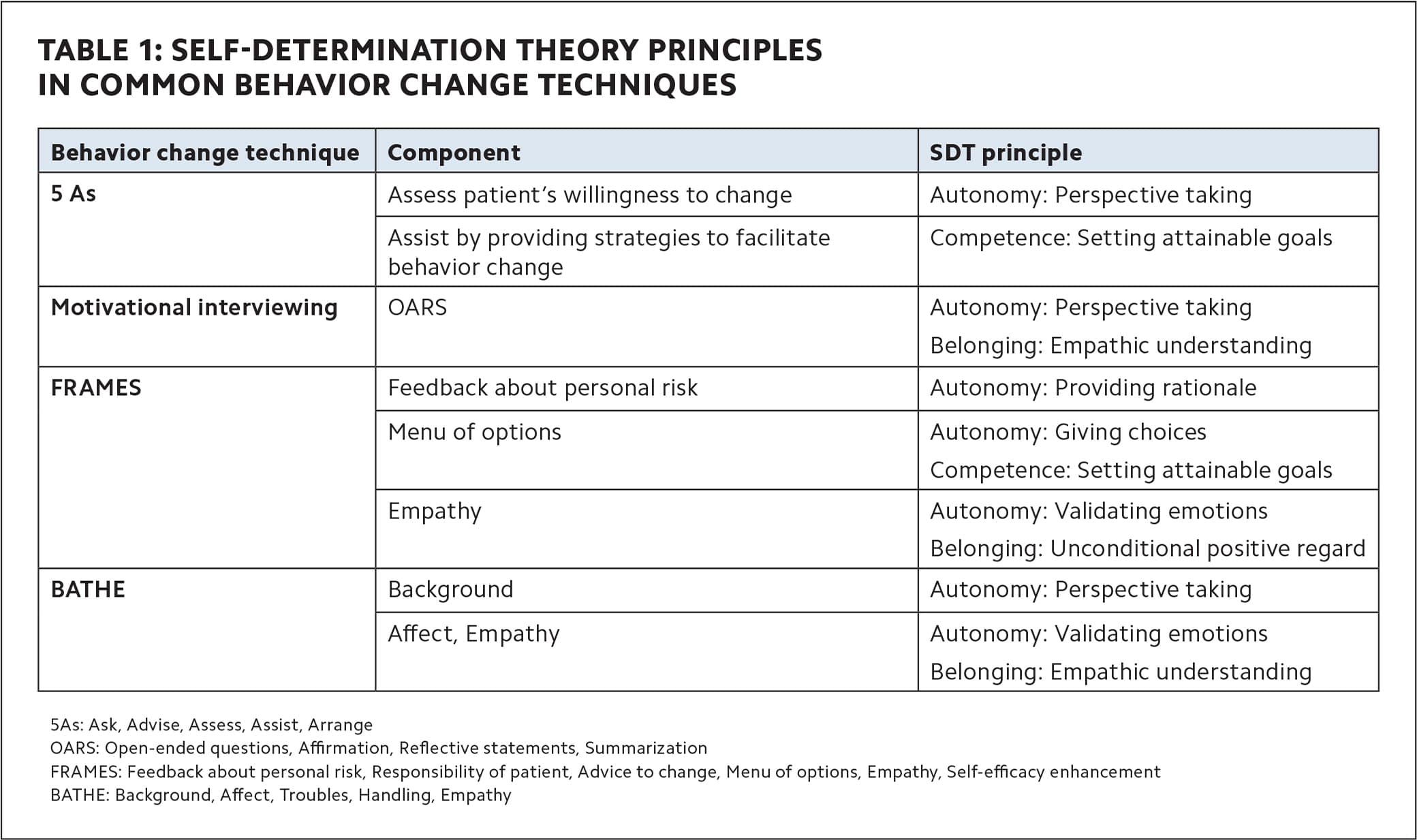
SELF-DETERMINATION THEORY PRINCIPLES IN COMMON BEHAVIOR CHANGE TECHNIQUES
| Behavior change technique | Component | SDT principle |
|---|---|---|
| 5 As | Assess patient’s willingness to change | Autonomy: Perspective taking |
| Assist by providing strategies to facilitate behavior change | Competence: Setting attainable goals | |
| Motivational interviewing | OARS | Autonomy: Perspective taking Belonging: Empathic understanding |
| FRAMES | Feedback about personal risk | Autonomy: Providing rationale |
| Menu of options | Autonomy: Giving choices Competence: Setting attainable goals |
|
| Empathy | Autonomy: Validating emotions Belonging: Unconditional positive regard |
|
| BATHE | Background | Autonomy: Perspective taking |
| Affect, Empathy | Autonomy: Validating emotions Belonging: Empathic understanding |
HOW DOES THE SDT FRAMEWORK LEAD TO HEALTH BEHAVIOR CHANGE?
Changing health-related behavior is a complex process. In the early stages, patients are often motivated by external pressures, such as the desire to lose weight, meet societal expectations, or avoid illness. In other words, their motivation is driven by outcomes or rewards associated with the behavior, rather than by personal interest or enjoyment.3 For example, patients might exercise or follow a strict diet to achieve a certain body image or avoid health risks. While such motivations can prompt action, it is often short-lived and can lead to frustration, or a sense of being controlled.
Over time, as patients internalize behaviors, their motivation can shift from external to a more self-determined form aligned with their personal values and interests.5 For example, while wearing a seatbelt is required by law, most people eventually do so not because of legal pressure, but because they recognize the safety benefits. Similarly, engaging in health-related behaviors, such as exercise, can evolve from a way to meet external standards to an activity that fosters pride and well-being, which supports long-term commitment.
This shift toward self-determined behavior occurs when patients’ basic psychological needs — autonomy, belonging, and competence — are supported. When we provide patients with the rationale for a behavior, such as the health benefits of a new habit or treatment plan, they can begin to understand its value and are more likely to adopt it as their own (autonomy), rather than feeling they are simply being told what to do. Furthermore, patients are more likely to adopt behaviors that align with their values if the recommendation comes from a trusted source or respected community (belonging). This sense of belonging helps them internalize the behavior and makes it feel more self-directed. As patients see their efforts leading to growth and mastery (competence), such as improved energy and vitality from consistent sleep hygiene, they are more likely to persist.
In contrast, when basic psychological needs are not supported, patients are more likely to experience little or no motivation, or to continue behaviors out of obligation (controlled motivation). This can result in stress, frustration, and difficulty maintaining change.
By understanding the psychological mechanisms behind motivation and actively supporting autonomy, belonging, and competence, clinicians can enhance their effectiveness in helping patients internalize behavior change and achieve lasting results.
A: AUTONOMY
To support patients’ autonomy, actively engage them in discussions about their experiences with their medical conditions and their motivations for change. By providing a meaningful rationale for your recommendations and offering patients choices in how to proceed, you can help empower them to make a decision that resonates with their personal goals and values. Additionally, providing nonjudgmental information and avoiding controlling language, such as “you must” and “you should,” can help nurture the patient’s autonomous motivation without causing unnecessary pressure or resistance.8 The four strategies outlined in Table 2 offer a good starting point for fostering autonomy.2
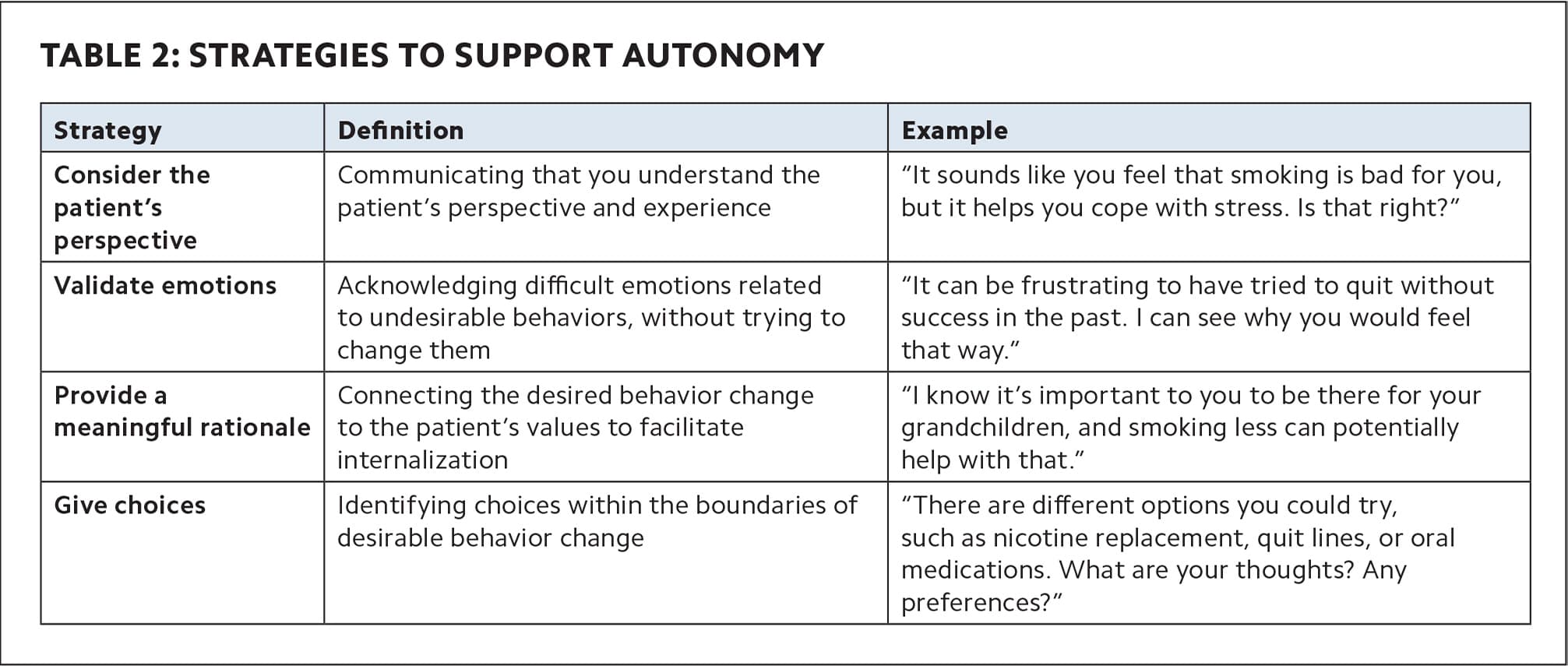
STRATEGIES TO SUPPORT AUTONOMY
| Strategy | Definition | Example |
|---|---|---|
| Consider the patient’s perspective | Communicating that you understand the patient’s perspective and experience | “It sounds like you feel that smoking is bad for you, but it helps you cope with stress. Is that right?” |
| Validate emotions | Acknowledging difficult emotions related to undesirable behaviors, without trying to change them | “It can be frustrating to have tried to quit without success in the past. I can see why you would feel that way.” |
| Provide a meaningful rationale | Connecting the desired behavior change to the patient’s values to facilitate internalization | “I know it’s important to you to be there for your grandchildren, and smoking less can potentially help with that.” |
| Give choices | Identifying choices within the boundaries of desirable behavior change | “There are different options you could try, such as nicotine replacement, quit lines, or oral medications. What are your thoughts? Any preferences?” |
B: BELONGING
To foster a sense of patient belonging (or relatedness), demonstrate unconditional positive regard, separating the behavior from the person, and maintain a nonjudgmental atmosphere, regardless of success or failure. This can be challenging at times, particularly when you feel pressured by time constraints or quality metrics that emphasize specific clinical outcomes. However, if patients perceive that care is contingent on a particular behavior or result, it can actually decrease their likelihood of achieving the desired outcome.
The most effective approach is to meet patients where they are, collaborating in a way that helps them feel heard, respected, and cared for. When these conditions are present, patients are more likely to listen to, internalize, and engage with medical recommendations.5,9 Strategies that support a sense of belonging are summarized in Table 3.
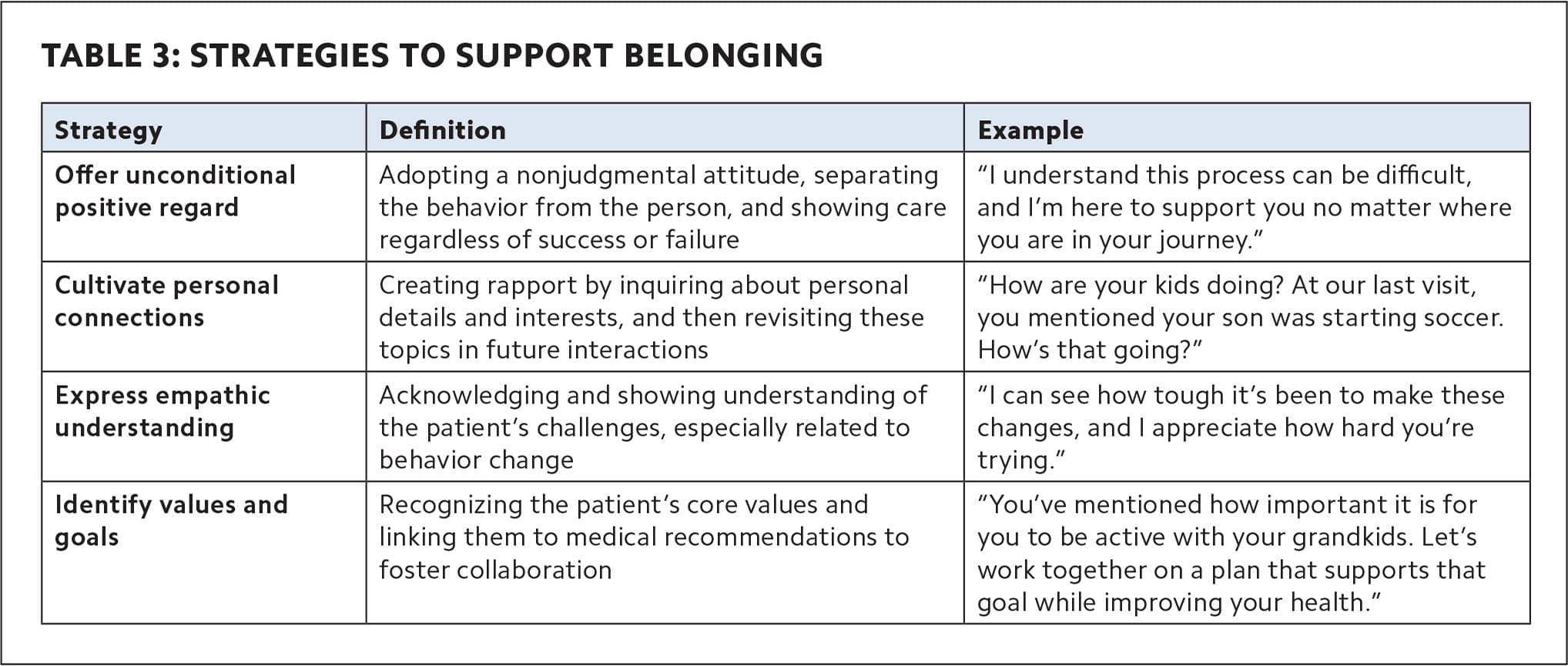
STRATEGIES TO SUPPORT BELONGING
| Strategy | Definition | Example |
|---|---|---|
| Offer unconditional positive regard | Adopting a nonjudgmental attitude, separating the behavior from the person, and showing care regardless of success or failure | “I understand this process can be difficult, and I’m here to support you no matter where you are in your journey.” |
| Cultivate personal connections | Creating rapport by inquiring about personal details and interests, and then revisiting these topics in future interactions | “How are your kids doing? At our last visit, you mentioned your son was starting soccer. How’s that going?” |
| Express empathic understanding | Acknowledging and showing understanding of the patient’s challenges, especially related to behavior change | “I can see how tough it’s been to make these changes, and I appreciate how hard you’re trying.” |
| Identify values and goals | Recognizing the patient’s core values and linking them to medical recommendations to foster collaboration | “You’ve mentioned how important it is for you to be active with your grandkids. Let’s work together on a plan that supports that goal while improving your health.” |
C: COMPETENCE
To support patient competence, collaborate with them to set attainable goals, offer encouragement, and provide structured guidance to help them succeed.5 Building competence also requires giving timely, specific, and actionable feedback regarding their progress. Work together with patients to set goals that are within the “optimal challenge zone” — neither too easy, which can be unengaging, nor too difficult, which can be overwhelming.
Other key elements of supporting patients’ sense of competence include celebrating successes, problem-solving any setbacks, scaffolding (identifying next steps to advance), and focusing on potential barriers to behavior change rather than on the individual’s personal shortcomings (see Table 4).9,10
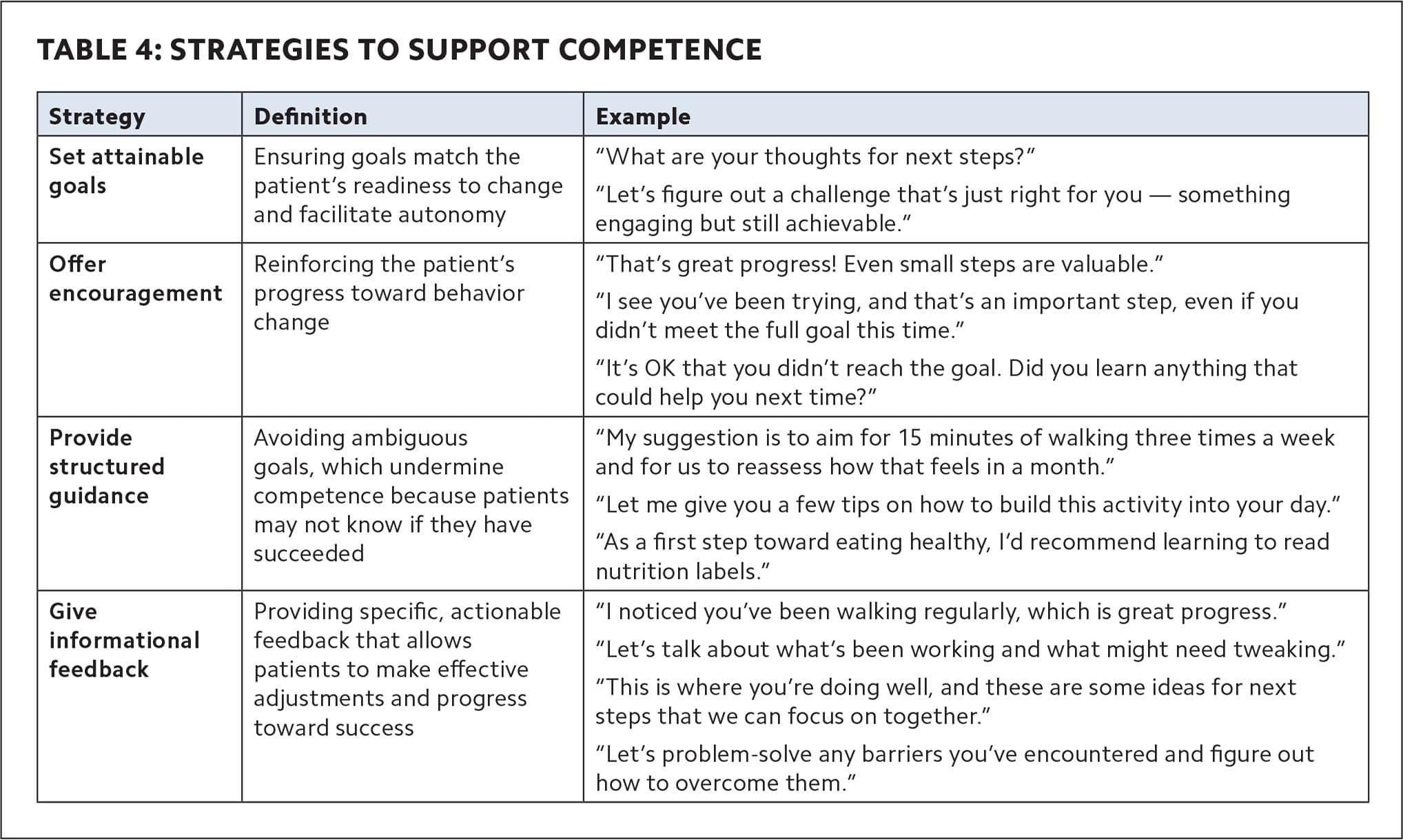
STRATEGIES TO SUPPORT COMPETENCE
| Strategy | Definition | Example |
|---|---|---|
| Set attainable goals | Ensuring goals match the patient’s readiness to change and facilitate autonomy | “What are your thoughts for next steps?” “Let’s figure out a challenge that’s just right for you — something engaging but still achievable.” |
| Offer encouragement | Reinforcing the patient’s progress toward behavior change | “That’s great progress! Even small steps are valuable.” “I see you’ve been trying, and that’s an important step, even if you didn’t meet the full goal this time.” “It’s OK that you didn’t reach the goal. Did you learn anything that could help you next time?” |
| Provide structured guidance | Avoiding ambiguous goals, which undermine competence because patients may not know if they have succeeded | “My suggestion is to aim for 15 minutes of walking three times a week and for us to reassess how that feels in a month.” “Let me give you a few tips on how to build this activity into your day.” “As a first step toward eating healthy, I’d recommend learning to read nutrition labels.” |
| Give informational feedback | Providing specific, actionable feedback that allows patients to make effective adjustments and progress toward success | “I noticed you’ve been walking regularly, which is great progress.” “Let’s talk about what’s been working and what might need tweaking.” “This is where you’re doing well, and these are some ideas for next steps that we can focus on together.” “Let’s problem-solve any barriers you’ve encountered and figure out how to overcome them.” |
MOVING FROM NEED-THWARTING TO NEED-SUPPORTING DIALOGUE
SDT provides an evidence-based framework for enhancing patient motivation and lasting behavior change by supporting basic psychological needs — autonomy, belonging, and competence. This approach shifts clinical dialogue from “need-thwarting” to “need-supporting” (see Table 5), which helps patients transition from controlled to autonomous motivation. In addition, this approach fosters more effective interactions and reduces frustration when addressing unhealthy behaviors. Even small changes in how we as clinicians communicate with patients and support their basic psychological needs can have a significant impact on patients’ adherence to recommendations, success in behavior change, and overall health and well-being.
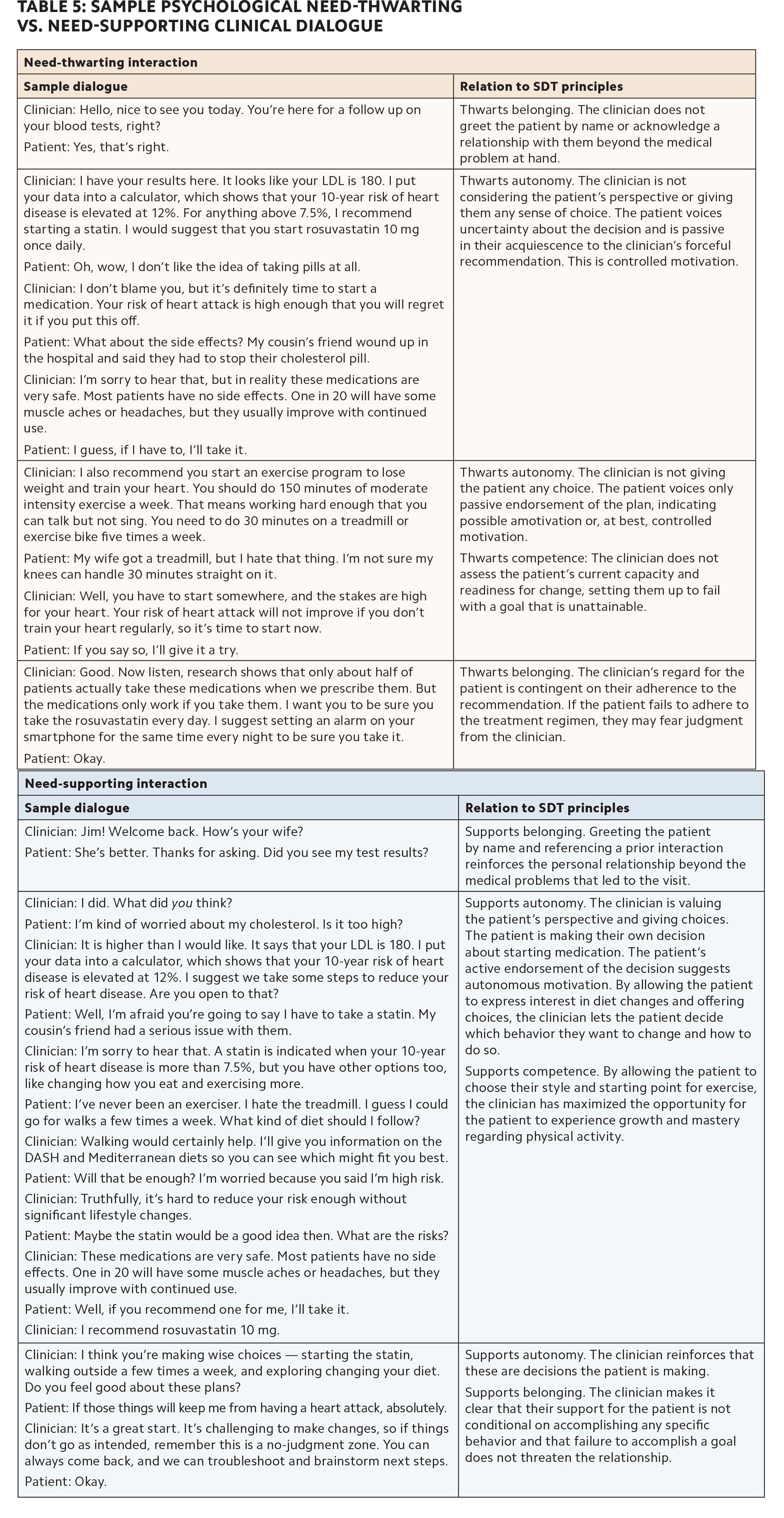
SAMPLE PSYCHOLOGICAL NEED-THWARTING VS. NEED-SUPPORTING CLINICAL DIALOGUE
| Need-thwarting interaction | Need-supporting interaction | ||
|---|---|---|---|
| Sample dialogue | Relation to SDT principles | Sample dialogue | Relation to SDT principles |
| Clinician: Hello, nice to see you today. You’re here for a follow up on your blood tests, right? Patient: Yes, that’s right. |
Thwarts belonging. The clinician does not greet the patient by name or acknowledge a relationship with them beyond the medical problem at hand. | Clinician: Jim! Welcome back. How’s your wife? Patient: She’s better. Thanks for asking. Did you see my test results? |
Supports belonging. Greeting the patient by name and referencing a prior interaction reinforces the personal relationship beyond the medical problems that led to the visit. |
| Clinician: I have your results here. It looks like your LDL is 180. I put your data into a calculator, which shows that your 10-year risk of heart disease is elevated at 12%. For anything above 7.5%, I recommend starting a statin. I would suggest that you start rosuvastatin 10 mg once daily. Patient: Oh, wow, I don’t like the idea of taking pills at all. Clinician: I don’t blame you, but it’s definitely time to start a medication. Your risk of heart attack is high enough that you will regret it if you put this off. Patient: What about the side effects? My cousin’s friend wound up in the hospital and said they had to stop their cholesterol pill. Clinician: I’m sorry to hear that, but in reality these medications are very safe. Most patients have no side effects. One in 20 will have some muscle aches or headaches, but they usually improve with continued use. Patient: I guess, if I have to, I’ll take it. |
Thwarts autonomy. The clinician is not considering the patient’s perspective or giving them any sense of choice. The patient voices uncertainty about the decision and is passive in their acquiescence to the clinician’s forceful recommendation. This is controlled motivation. | Clinician: I did. What did you think? Patient: I’m kind of worried about my cholesterol. Is it too high? Clinician: It is higher than I would like. It says that your LDL is 180. I put your data into a calculator, which shows that your 10-year risk of heart disease is elevated at 12%. I suggest we take some steps to reduce your risk of heart disease. Are you open to that? Patient: Well, I’m afraid you’re going to say I have to take a statin. My cousin’s friend had a serious issue with them. Clinician: I’m sorry to hear that. A statin is indicated when your 10-year risk of heart disease is more than 7.5%, but you have other options too, like changing how you eat and exercising more. |
Supports autonomy. The clinician is valuing the patient’s perspective and giving choices. The patient is making their own decision about starting medication. The patient’s active endorsement of the decision suggests autonomous motivation. By allowing the patient to express interest in diet changes and offering choices, the clinician lets the patient decide which behavior they want to change and how to do so. |
| Clinician: I also recommend you start an exercise program to lose weight and train your heart. You should do 150 minutes of moderate intensity exercise a week. That means working hard enough that you can talk but not sing. You need to do 30 minutes on a treadmill or exercise bike five times a week. Patient: My wife got a treadmill, but I hate that thing. I’m not sure my knees can handle 30 minutes straight on it. Clinician: Well, you have to start somewhere, and the stakes are high for your heart. Your risk of heart attack will not improve if you don’t train your heart regularly, so it’s time to start now. Patient: If you say so, I’ll give it a try. |
Thwarts autonomy. The clinician is not giving the patient any choice. The patient voices only passive endorsement of the plan, indicating possible amotivation or, at best, controlled motivation. Thwarts competence: The clinician does not assess the patient’s current capacity and readiness for change, setting them up to fail with a goal that is unattainable. |
Patient: I’ve never been an exerciser. I hate the treadmill. I guess I could go for walks a few times a week. What kind of diet should I follow? Clinician: Walking would certainly help. I’ll give you information on the DASH and Mediterranean diets so you can see which might fit you best. Patient: Will that be enough? I’m worried because you said I’m high risk. Clinician: Truthfully, it’s hard to reduce your risk enough without significant lifestyle changes. Patient: Maybe the statin would be a good idea then. What are the risks? Clinician: These medications are very safe. Most patients have no side effects. One in 20 will have some muscle aches or headaches, but they usually improve with continued use. Patient: Well, if you recommend one for me, I’ll take it. Clinician: I recommend rosuvastatin 10 mg. |
Supports competence. By allowing the patient to choose their style and starting point for exercise, the clinician has maximized the opportunity for the patient to experience growth and mastery regarding physical activity. |
| Clinician: Good. Now listen, research shows that only about half of patients actually take these medications when we prescribe them. But the medications only work if you take them. I want you to be sure you take the rosuvastatin every day. I suggest setting an alarm on your smartphone for the same time every night to be sure you take it. Patient: Okay. |
Thwarts belonging. The clinician’s regard for the patient is contingent on their adherence to the recommendation. If the patient fails to adhere to the treatment regimen, they may fear judgment from the clinician. | Clinician: I think you’re making wise choices — starting the statin, walking outside a few times a week, and exploring changing your diet. Do you feel good about these plans? Patient: If those things will keep me from having a heart attack, absolutely. Clinician: It’s a great start. It’s challenging to make changes, so if things don’t go as intended, remember this is a no-judgment zone. You can always come back, and we can troubleshoot and brainstorm next steps. Patient: Okay. |
Supports autonomy. The clinician reinforces that these are decisions the patient is making. Supports belonging. The clinician makes it clear that their support for the patient is not conditional on accomplishing any specific behavior and that failure to accomplish a goal does not threaten the relationship. |
