Rosacea is a common, but often overlooked, skin condition of uncertain etiology that can lead to significant facial disfigurement, ocular complications, and severe emotional distress. The progression of rosacea is variable; however, typical stages include: (1) facial flushing, (2) erythema and/or edema and ocular symptoms, (3) papules and pustules, and (4) rhinophyma. A history of exacerbation by sun exposure, stress, cold weather, hot beverages, alcohol consumption, or certain foods helps determine the diagnosis; the first line of treatment is avoidance of these triggering or exacerbating factors. Most patients respond well to long-term topical antibiotic treatment. Oral or topical retinoid therapy may also be effective. Laser treatment is an option for progressive telangiectasis or rhinophyma. Family physicians should be able to identify and effectively treat the majority of patients with rosacea. Consultation with subspecialists may be required for the management of rhinophyma, ocular complications, or severe disease.
Rosacea is a common, but often overlooked, skin condition that can lead to significant facial disfigurement, emotional suffering, and serious ocular complications if left untreated. Little is known about the epidemiology of rosacea, but the condition most frequently occurs in persons between 30 and 50 years of age and in fair-skinned persons of northern European descent.1,2 Studies1 have shown that women are affected about two to three times more frequently than men. Rosacea may be underdiag-nosed1,3 because patients may not discuss the symptoms with their physician and because some physicians may not recognize the disorder. Rosacea may be overlooked in nonwhites because of a low index of suspicion or because skin pigmentation results in an atypical presentation.4 Ocular complications and late manifestations of rosacea may occur in a disproportionate number of dark-skinned persons.5 Although rosacea can occur in the teenaged years,6 the incidence of rosacea in this age group is probably low. The incidence of rhinophyma, the most obvious stigma of rosacea, is unknown and occurs more often in men.7 The prevalence of rosacea appears to be increasing in the United States3,8; this may be a result of the aging of the “baby-boom” generation, rather than an increase in incidence.
Pathophysiology
Rosacea results from an inflammatory process about which little is known.3,7 The stimulus includes a wide variety of foods as well as environmental, chemical, psychologic, and emotional factors (Table 1). It is unclear what role, if any, these factors have in the causation or exacerbation of this condition. In particular, the link between emotional stress and rosacea is not well understood. Studies have found possible associations between rosacea and the face mite Demodex folliculorum,9,10 Helicobacter pylori infection,11–13 and migraine headaches.3,14
TABLE 1 Common Factors that May Aggravate Rosacea*
| Aggravating factor | Percentage (%) |
|---|---|
| Sun exposure | 61 |
| Emotional stress | 60 |
| Hot weather | 53 |
| Alcohol | 45 |
| Spicy foods | 43 |
| Exercise | 39 |
| Wind | 38 |
| Hot baths | 37 |
| Cold weather | 36 |
| Hot drinks | 36 |
| Skin-care products | 24 |
*—Percentages of rosacea patients affected by the most common factors that may trigger rosacea flare-ups, based on a survey of more than 400 persons with rosacea by the National Rosacea Society.
Information retrieved June 2002 fromwww.rosacea.org/copintro.html.
Clinical Features
Rosacea is an indiscrete disease with a variety of facial skin and ocular manifestations that differ from patient to patient.7 The predominant, presenting complaints of rosacea are intermittent, central facial flushing and erythema. Itching is always absent; however, many patients complain of a stinging pain (which can be severe) associated with flushing episodes. These flushing episodes are often socially embarrassing and can occur unpredictably or can be linked to environmental, chemical, food, or emotional triggers. Common triggers include exposure to the sun, cold weather, sudden emotion (laughter or embarrassment), hot beverages, and alcohol consumption (Table 1).8 Unfortunately, some people associate rosacea and rhinophyma with alcohol abuse; however, many patients who have rosacea neither drink alcohol nor report alcohol as a trigger for their rosacea.
Central facial erythema and telangiectasis are predominant in the early stages of rosacea3,8 (Figures 1 and 2). This progresses to a chronic inflammatory infiltrate with central facial papules and, less commonly, sterile pustules. Intermittent or chronic facial edema may also occur. Some patients develop rhinophyma, a coarse hypertrophy of the connective tissue and sebaceous glands of the nose (Figures 3 and 4). The stages of rosacea are summarized in Table 2.
FIGURE 1.

Papular rosacea with nasal erythema and telangiectasias.
FIGURE 2.

Prominent erythema with pustules. This could be confused with the malar rash of systemic lupus erythematosus.
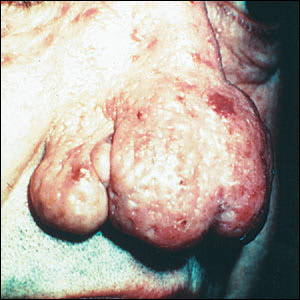
FIGURE 3.

Rhinophyma with a few papules and telangiectasias also visible.
FIGURE 4.
Advanced rhinophyma.
TABLE 2 Stages of Rosacea and Their Symptoms
| Pre-rosacea | Inflammatory |
| Flushing and blushing | Papules and pustules |
| Vascular | Late |
| Erythema, and/or edema | Rhinophyma |
| Ocular symptoms | |
Ocular problems occur in at least 50 percent of patients with rosacea [Evidence level B, non-randomized studies].15 The most common complication of the eye associated with rosacea is an intermittent inflammatory conjunctivitis, with or without blepharitis (Figure 5). Prominent symptoms include eyes that are itchy, burning, or dry; a gritty or foreign body sensation; and erythema and swelling of the eyelid. The ocular changes can become chronic. Corneal neovascularization and keratitis can occur, leading to corneal scarring and perforation. Episcleritis and iritis have also been reported to occur in patients with rosacea.15
FIGURE 5.

Inflammatory conjunctivitis with blepharitis.
Differential Diagnosis
Acne is commonly confused with rosacea, especially in middle-aged adults with late-onset acne. Telangiectasis is consistent with rosacea, but comedo formation is not. Eye symptoms are not associated with acne, so a careful examination for eye symptoms or a finding of ocular pathology will help confirm the diagnosis of rosacea.2 Application of topical steroids to the face may induce an acneform eruption resembling the pustular form of rosacea. Steroid-induced acne presents with a more perioral distribution of the skin lesions. This distribution and a thorough history of medication use usually distinguish between the two conditions.16
Photodermatitis (or polymorphous light eruption) is triggered by exposure to sunlight and has skin manifestations similar to rosacea. This condition is distinguishable from rosacea because it affects all sun-exposed areas of the body, and patients will develop light sensitivity with repeated exposure.
In patients with the malar rash of systemic lupus erythematosus, papules may be present, but pustules are rare. Occasionally, rosacea may present with a granulomatous appearance that may be difficult to distinguish from facial sarcoid. A skin biopsy may be necessary for a definitive diagnosis.17
A careful history will usually distinguish between rosacea and allergic conjunctivitis in patients who present with recurrent conjunctivitis or blepharitis. Concurrent skin changes usually confirm the diagnosis of rosacea. Seborrheic dermatitis has similar skin manifestations but with a distinctive distribution pattern at the scalp, eyebrows, and nasolabial folds.
Finally, patients who present with unusually severe facial flushing may need to be evaluated for mastocytosis or carcinoid syndrome,18 particularly if flushing is systemic or does not have an obvious trigger. In carcinoid syndrome, gastrointestinal, cardiac, and pulmonary symptoms are found. The differential diagnosis for rosacea is listed in Table 3.
TABLE 3 Differential Diagnosis of Rosacea
| Acne | |
| Adult-onset acne | |
| Drug-induced acne | |
| Steroid-induced acne | |
| Photodermatitis (polymorphous light eruption) | |
| Systemic lupus erythematosus | |
| Sarcoidosis | |
| Allergic conjunctivitis | |
| Seborrheic dermatitis | |
| Mastocytosis | |
| Carcinoid syndrome | |
Complications
Patients with rosacea suffer from a variety of emotional and social stigmas.19 Patients often have feelings of low self-esteem when facial features change and papules, pustules, and other “unsightly” features of the disorder progress. Patients may report feelings of embarrassment or anxiety about their facial flushing and erythema in social situations. This anxiety may resemble panic disorder and can cause some patients to become reclusive.20Patients may also feel that their facial disfigurement lessens their sexual desirability or impedes their career advancement. Rosacea patients may also be inaccurately viewed as abusers of alcohol.
Ocular complications often occur in patients with rosacea, and can be severe enough to require corneal replacement. Early consultation with an ophthalmologist is essential for patients with suspected corneal involvement and should be considered in any patient with refractory conjunctivitis or blepharitis.17
Treatment
PREVENTION
The initial therapeutic step is avoidance of exacerbating factors for rosacea [Evidence level C, consensus/expert opinion].8 Physicians should advise their patients to carefully monitor their exposure to the sun and to regularly use sunscreen products. One study21 suggests that patients with rosacea may better tolerate sunscreens containing simethicone or cyclomethicone. Irritating skin care products and heavy cosmetics should be avoided. Other factors commonly associated with rosacea exacerbations are listed in Table 1.
ANTIBIOTICS
Oral antibiotics, such as tetracycline, doxycycline (Vibramycin), and metronidazole (Flagyl) effectively treat papulopustular rosacea. Topical metronidazole (cream [MetroCream] or gel [MetroGel]) administered twice daily is as effective as oral tetracycline22 and is considered the agent of choice for pustular and papular rosacea [Evidence level A, randomized controlled trials]; however, some patients experience burning and stinging with the use of topical metronidazole. Some studies23 suggest that topical metronidazole also reduces erythema and telangiectasis in some patients. Topical clindamycin (Cleocin) is an effective alternative in patients who are pregnant; the use of oral tetracycline or metronidazole is undesirable during pregnancy24 [Evidence level A, randomized controlled trial]. The antibiotic gel or cream should be applied across the entire face, rather than “spot treating” the lesions.25
Rosacea is a chronic, relapsing disorder, and long-term treatment is generally required. Control of symptoms can be successfully maintained by long-term use of metronidazole gel.25
SECOND-LINE THERAPIES
In recalcitrant cases where antibiotics have failed or were partially successful, oral isotretinoin (Accutane) or topical tretinoin (RetinA) therapy may be effective26,27 [Evidence level B, nonrandomized studies]. Retinoid treatment (especially in the topical form) may help recalcitrant papular and pustular forms of rosacea but may worsen erythema and telangiectasis.3 Some authorities question the role of retinoids in rosacea treatment.
Other second-line therapies include: trimethoprim-sulfamethoxazole (Bactrim, Septra), methotrexate, dapsone, primaquine, chloroquine (Aralen), and oral prednisone; however, no studies have evaluated the comparative efficacy or optimal dosing regimens of these agents.3,7
Topical corticosteroids must be avoided on the face.16 The use of fluorinated topical steroids on the face frequently produces a rosacea-like syndrome, and even low-potency, nonfluorinated steroids may worsen pre-existing rosacea and delay the resolution of steroid-induced flare-ups by months.16,17
TREATMENT OF OCULAR ROSACEA
Oral tetracycline and doxycycline effectively control the ocular symptoms of rosacea; these are the only agents that have been rigorously studied in the treatment of ocular rosacea2,15 [Evidence level B, nonrandomized studies]. A short course of topical corticosteroid solution may be useful for symptomatic relief of ocular rosacea2; however, ocular steroid therapy should be initiated and managed by an ophthalmologist because experience with this treatment is limited. Liquid tears are useful for dry eyes and relief of ocular itching.2 Low-dose treatment with oral isotretinoin (10 mg, three times weekly for two to three months) has also been successful in recalcitrant ocular cases2 [Evidence level C, expert opinion].
TREATMENT OF ERYTHEMA AND FLUSHING
Oral and topical antibiotics are often ineffective in the treatment of erythema and flushing. The most effective way to prevent the occurrence of flushing episodes and the progression of the disease is to avoid the associated trigger factors. Low-dose clonidine (Catapres; 0.05 mg twice daily) may be effective in controlling flushing, especially in women who are postmenopausal.18 A nonselective beta blocker (such as long-acting propranolol [Inderal], 80 to 240 mg daily, and nadolol [Corgard], 40 to 80 mg daily) may also be used to treat erythema and flushing.18
TREATMENT OF TELANGIECTASIS
One of the most difficult problems associated with rosacea is telangiectasis (Figure 1). Green-tinted cosmetics can be used to help mask erythema and telangiectasis.8 Treatment with a pulsed dye laser may be effective in advanced cases28,29 [Evidence level B, nonrandomized studies]. If performed by an experienced physician, laser therapy usually has no complications. Temporary hyperpigmentation of treated areas may occur in 5 to 20 percent of patients.28 Repeat treatments are sometimes necessary.
TREATMENT OF RHINOPHYMA
The initial stages of rhinophyma may respond to antibiotic treatment, but more advanced cases must be treated with surgery. A number of techniques have been advocated, including dermabrasion, cryosurgery, and excision of hypertrophic tissue by electrosurgery or with a laser.30
NEW CONCEPTS AND TREATMENTS
Recent research has yielded insight into the role of vascular endothelial growth factors (VEGF) in a variety of disorders, including rosacea.31 Retinoids appear to modulate the expression of VEGFs in the skin; this may explain the therapeutic benefit of isotretinoin in the treatment of rosacea observed in some studies.32 Medications targeted specifically for VEGFs in the skin may be developed.
Azelaic acid (Azelex) is a new topical agent that has been approved by the U.S. Food and Drug Administration for the treatment of acne. It is available in a 20 percent cream base and appears to be safe and well tolerated. A randomized, double-blinded study showed that azelaic acid was as effective as topical metronidazole in the treatment of pustular and papular forms of rosacea and had comparable side effects.33
Patient Education
Patients should be informed that there is no cure for rosacea, but that the variety of treatments available can effectively manage the disorder and minimize the progression of its symptoms. Patients can take an active role in the treatment of rosacea by learning about trigger factors and taking avoidance measures. Patients should be educated about the regular use of topical sunscreens, the appropriate use of concealing makeup, and the need for careful follow-up of ocular symptoms.
