Atopic dermatitis, also known as atopic eczema, is a chronic pruritic skin condition affecting approximately 17.8 million persons in the United States. It can lead to significant morbidity. A simplified version of the U.K. Working Party’s Diagnostic Criteria can help make the diagnosis. Asking about the presence and frequency of symptoms can allow physicians to grade the severity of the disease and response to treatment. Management consists of relieving symptoms and lengthening time between flare-ups. Regular, liberal use of emollients is recommended. The primary pharmacologic treatment is topical corticosteroids. Twice-daily or more frequent application has not been shown to be more effective than once-daily application. A maintenance regimen of topical corticosteroids may reduce relapse rates in patients who have recurrent moderate to severe atopic dermatitis. Pimecrolimus and tacrolimus are calcineurin inhibitors that are recommended as second-line treatment for persons with moderate to severe atopic dermatitis and who are at risk of atrophy from topical corticosteroids. Although the U.S. Food and Drug Administration has issued a boxed warning about a possible link between these medications and skin malignancies and lymphoma, studies have not demonstrated a clear link. Topical and oral antibiotics may be used to treat secondary bacterial infections, but are not effective in preventing atopic dermatitis flare-ups. The effectiveness of alternative therapies, such as Chinese herbal preparations, homeopathy, hypnotherapy/biofeedback, and massage therapy, has not been established.
Atopic dermatitis, also known as atopic eczema, is a chronic inflammatory skin condition characterized by pruritic, erythematous, and scaly skin lesions often localized to the flexural surfaces of the body (Figure 1). It can present with asthma and allergic rhinitis as part of an allergic triad; an estimated 30 percent of children with atopic dermatitis develop asthma later in life.1 The onset of atopic dermatitis generally is before two years of age, with only 10 percent of cases diagnosed after five years of age.2 A 2003 survey of children in the United States estimated an overall prevalence of approximately 11 percent, and as high as 19 percent in some states.3 A 2007 U.S. population-based survey suggested an estimated 17.8 million persons are living with atopic dermatitis, and most cases have not been diagnosed.4 Early diagnosis and treatment may prevent significant morbidity from sleep disturbances, chronic postinflammatory skin changes, scarring from picking and scratching, and the development of secondary skin infections with Staphylococcus, Streptococcus, and herpes species.5
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendation | Evidence rating | References |
|---|---|---|
| Emollients are a mainstay of therapy for atopic dermatitis. | C | 12, 27 |
| Topical corticosteroids are first-line treatment for atopic dermatitis flare-ups. | A | 12, 13 |
| Topical calcineurin inhibitors are second-line treatment for moderate to severe atopic dermatitis. | A | 12, 15, 17 |
| Antibiotics are not useful in reducing flare-ups of atopic dermatitis unless there is clear evidence of a secondary infection. | A | 24, 25 |
| Ultraviolet phototherapy is effective for treating severe or refractory atopic dermatitis. | B | 12, 25 |
| The immunomodulatory agents cyclosporine (Sandimmune) and interferon gamma-1b are effective for treating severe or refractory atopic dermatitis. | A | 12, 25 |
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.xml.
Figure 1.

Atopic dermatitis on the flexural surface of the arm.
Pathophysiology
A genetic defect in the filaggrin protein is thought to cause atopic dermatitis by disrupting the epidermis. This disruption, in turn, results in contact between immune cells in the dermis and antigens from the external environment leading to intense itching, scratching, and inflammation.6 Scratching can then lead to further disruption and inflammation of the epidermal skin barrier; this has been described as the itchscratch cycle.2
Clinical Presentation and Differential Diagnosis
Atopic dermatitis can present in three clinical phases. Acute atopic dermatitis presents with a vesicular, weeping, crusting eruption (Figure 2). Subacute atopic dermatitis presents with dry, scaly, erythematous papules and plaques (Figure 3). Chronic atopic dermatitis demonstrates lichenification from repeated scratching (Figures 4 and 5). A more subtle presentation of atopic dermatitis that commonly occurs in children is pityriasis alba, which is characterized by hypopigmented, poorly demarcated plaques with fine scale. Atopic dermatitis tends to involve the flexural surfaces of the body, anterior and lateral neck, eyelids, forehead, face, wrists, dorsa of the feet, and hands. Because atopic dermatitis has many appearances, the differential diagnosis is broad (Table 1).7
Figure 2.
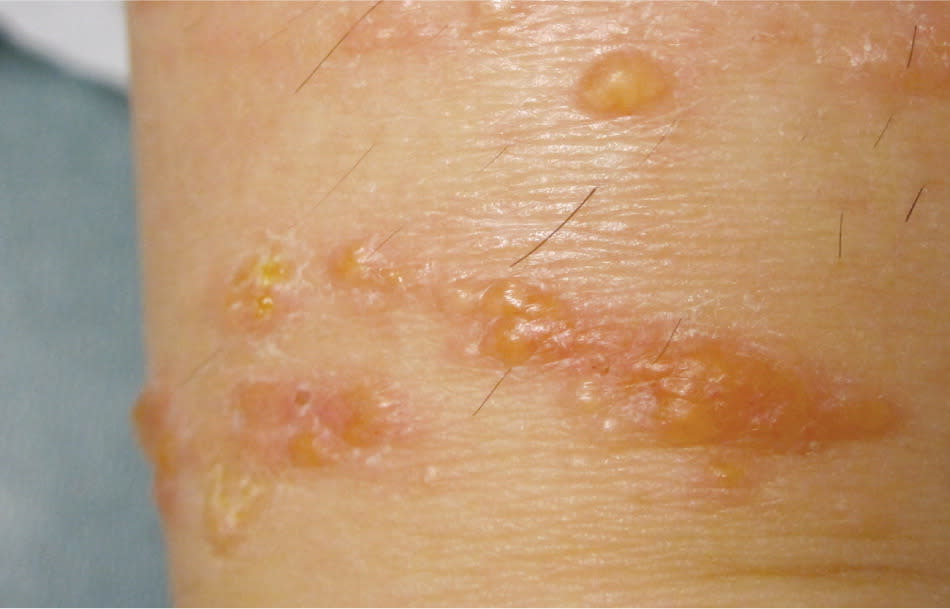
Acute atopic dermatitis in its weeping, blistering form.
Figure 3.

Subacute atopic dermatitis in its dry, scaly, papular form.
Figure 4.

Chronic atopic dermatitis in its lichenified form. Note the associated hyperpigmentation.
Figure 5.

Chronic atopic dermatitis demonstrating a lichenified plaque, as well as depigmentation resulting from repeated scratching.
Table 1. Differential Diagnosis for Atopic Dermatitis
| Candidiasis |
| Conditions that cause generalized pruritus |
| Contact dermatitis |
| Dermatitis herpetiformis |
| Impetigo |
| Lichen simplex chronicus |
| Nummular eczema |
| Psoriasis |
| Scabies |
| Seborrheic dermatitis |
| Urticaria |
| Xerosis |
Information from reference 7.
Diagnosis and Classification
Diagnosis of atopic dermatitis is based on history and physical examination. There are many proposed diagnostic criteria; however, a 2008 systematic review concluded that the U.K. Working Party’s Diagnostic Criteria are the most extensively validated.8 A simplified version of these criteria has a sensitivity and specificity of up to 95 and 97 percent, respectively.9,10 The simplified criteria include itchy skin, with at least three of the following: history of asthma or allergic rhinitis; history of flexural involvement; history of generalized dry skin; onset of rash before two years of age; and visible flexural dermatitis. It is helpful to ask patients about the number of days per week they experience symptoms, such as pruritus, bleeding, oozing clear fluid, or dry and flaky skin.
Complications
Patients with atopic dermatitis can develop a secondary bacterial infection from skin flora, particularly Staphylococcus and Streptococcus species. Secondarily infected atopic dermatitis presents with pustules and crusts, and should be suspected if symptoms do not respond to conventional therapy, or if the patient presents with fever and malaise or rapidly worsening symptoms. Patients with atopic dermatitis are also at risk of developing herpes simplex virus infection, known as Kaposi varicelliform eruption or eczema herpeticum. Eczematous skin enables a localized herpes outbreak to spread over the skin and create a painful papulovesicular rash (Figure 6). Other complications of atopic dermatitis include scars from picking and scratching, chronic postinflammatory skin changes, and skin atrophy from long-term treatment with topical corticosteroids.
Figure 6.

Eczema herpeticum in a young girl. Note the generalized papulovesicular rash.
Management
Table 2 summarizes the treatment approaches for atopic dermatitis.11–25 Indications for referral to a dermatologist are summarized in Table 3.11,26
Table 2. Atopic Dermatitis Treatment Summary
| Emollients | |
| Recommend regular and liberal use of emollients on a daily basis and other xerosis-reducing behaviors (e.g., taking low-heat showers, using emollient washes) | |
| Topical corticosteroids (first-line prescription management) | |
| When indicated: emollient use alone is not adequate to control symptoms | |
| Application: once or twice daily | |
| Vehicles: ointments, creams, lotions, solutions, tape, etc. | |
| Potencies: ranges from group I (most potent) to group VII (least potent); potency choice should be based on disease severity | |
| Adverse effects: atrophy, striae, telangiectasia, corticosteroid acne; potential risk of adrenal suppression and growth retardation with longer-term use of high-potency topical corticosteroids in children | |
| Main advantages: effective, cost-effective (most are available in generic form) | |
| Main disadvantage: risk of atrophy | |
| Other: consider longer treatment or occlusive therapy for lichenified plaques; consider maintenance dose (e.g., twice weekly) for persons with recurrent atopic dermatitis | |
| Topical calcineurin inhibitors (second-line prescription management) | |
| When indicated: short-term or intermittent long-term use in persons with moderate to severe atopic dermatitis, especially when there is concern that ongoing use of conventional topical corticosteroids will lead to atrophy or other complications | |
| Application: Twice daily | |
| Vehicles: pimecrolimus (Elidel) cream and tacrolimus (Protopic) ointment | |
| Potencies: | |
| Pimecrolimus 1% cream (indicated for persons two years and older) | |
| Tacrolimus 0.1% ointment (indicated for use in adults only) | |
| Tacrolimus 0.03% ointment (indicated for persons two years and older) | |
| Adverse effects: transient skin burning and irritation; FDA boxed warning about the potential risks of skin malignancies and lymphoma, but studies have not demonstrated these risks | |
| Main advantage: no risk of atrophy | |
| Main disadvantages: expensive, FDA boxed warning | |
| Other: | |
| Tacrolimus 0.1% ointment is considered at least as effective as a potent topical corticosteroid | |
| Pimecrolimus is considered weaker than moderate or potent topical corticosteroids, but has not been compared with mild agents | |
| Pimecrolimus may be preferred in some patients because of its cream formulation | |
| Antibiotics | |
| When indicated: clear evidence of a secondary infection | |
| Choice of antibiotics: agents with good coverage of Staphylococcus and Streptococcus species | |
| Other: antibiotics have not proven to be effective for improving atopic dermatitis by reducing staphylococcal colonization | |
| UV phototherapy and systemic immunomodulator therapies (e.g., cyclosporine (Sandimmune), interferon gamma-1b) | |
| When indicated: atopic dermatitis refractory to treatment with topical agents or severe widespread atopic dermatitis | |
| Other: UV phototherapy and systemic therapies require supervision and treatment by a dermatologist | |
FDA = U.S. Food and Drug Administration; UV = ultraviolet.
Table 3. Indications for Referral to a Dermatologist
| Uncertain diagnosis |
| Attempts at management have not controlled the symptoms |
| Patient has atopic dermatitis on the face that has not responded to treatment |
| Patient has frequent flare-ups or severe atopic dermatitis |
| Patient requires systemic therapies for flare-ups or maintenance |
| Condition is causing significant psychosocial disturbances (e.g., sleep disruption, school or work attendance problems) |
| Contact allergic dermatitis is suspected (especially on the face, eyelids, or hands) |
EMOLLIENTS
Xerosis (skin dryness) is a common finding in atopic dermatitis, and many patients attest that control of their xerosis mirrors control of their dermatitis (Figures 7 and 8). Consequently, patients with atopic dermatitis should liberally apply emollients to the entire body whether or not active symptoms are present.11,12 A randomized controlled trial of infants with moderate to severe atopic dermatitis revealed that regular emollient use reduced the need for topical corticosteroid use and improved symptoms.27
Figure 7.

Close-up photograph of the skin demonstrating dramatic xerosis.
Figure 8.

Leg of an infant with atopic dermatitis demonstrating xerosis.
Moisturizers help retain and replenish epidermal moisture. However, not all emollients are the same. In general, emollients with high oil content and low water content are recommended. Thick creams that are low in water (e.g., Cetaphil, Eucerin) or ointments (e.g., Aquaphor, petroleum jelly) are preferred. Although their superiority over conventional emollients is not well established, a new generation of barrier-repair moisturizers are now available and are designed to add ceramide lipids to skin in addition to hydration (e.g., Cerave, Restoraderm). To avoid xerosis, physicians should recommend that patients shower with warm instead of hot water and use an emollient wash while showering.
TOPICAL CORTICOSTEROIDS
Topical corticosteroids are first-line treatment for atopic dermatitis flare-ups.12,13 The potencies range from group I, which is most potent (e.g., clobetasol [Temovate]), through group VII, which is least potent (e.g., hydrocortisone 1%). In general, the potency should be tailored to the severity of the disease. For persons with lichenified plaques consistent with chronic eczema (e.g., lichen simplex chronicus), higher-potency corticosteroids for longer periods of time often are needed, and occlusive therapy can be helpful.
To avoid atrophy, mild-potency corticosteroids are recommended for the face, neck, axillae, groin, and flexor surfaces. If the patient is experiencing a significant flare-up, using moderate potencies in these areas for short periods of time (e.g., two weeks or less) is acceptable. Consultation with a dermatologist is recommended before using high-potency corticosteroids in children.11 Patients also should be counseled to apply the corticosteroid only to the affected areas of the skin.
Because of their respective occlusive properties, the vehicles for the corticosteroid also affect its potency. The ointment form often is more potent than the cream, and the cream usually is more potent than the lotion. However, patients may prefer different vehicles. For example, because ointments are oily, patients may find them undesirable.
Studies have demonstrated no significant difference in outcome with once-daily versus twice-daily or more frequent application of a corticosteroid.14 The “rule of hand” can be helpful in estimating the amount to prescribe (Table 4).28
Table 4. Amount of Topical Corticosteroids to Prescribe Based on the Rule of Hand*
| Location | Adult (g) | Older child (g) | Younger child (g) | Infant < one year (g) |
|---|---|---|---|---|
| Arm and hand | 60 | 40 | 20 | 15 |
| Back and buttocks | 100 | 70 | 40 | 20 |
| Entire body | 580 | 350 | 190 | 120 |
| Face and neck | 30 | 30 | 20 | 15 |
| Front of chest and abdomen | 100 | 50 | 30 | 15 |
| Hand and fingers (front and back) | 15 | 10 | 7.5 | 5 |
| Leg and foot | 110 | 60 | 30 | 20 |
*—According to the rule of hand, the area of the side of one adult hand is equal to 1 percent of body surface area, and requires 0.25 g of medication for one application. Amounts listed are for twice daily application for 14 days, rounded to the nearest 10 for amounts of 20 g or greater.
Information from reference 28.
After acute symptoms have resolved, it is common to have the patient return to emollient use only. However, for patients who have recurrent moderate to severe atopic dermatitis, a maintenance regimen may be considered. In a randomized double-blind controlled study of adults with moderate to severe atopic dermatitis, maintenance therapy with twice-weekly corticosteroid application, along with an emollient, significantly decreased relapse rates compared with emollients alone.29 A similar study in children with moderate to severe atopic dermatitis revealed that intermittent treatment with a topical corticosteroid reduced severity and relapse rates.30 Physicians should consider prescribing higher-potency topical corticosteroids for maintenance, and gradually tapering potency and application frequency to the minimum necessary to prevent relapses.
The principal complication of prolonged application of topical corticosteroids, especially those of higher-potency, is skin atrophy (Figure 9). Other local complications include telangiectasia, striae, hypopigmentation, and corticosteroid acne (Figure 10). Although high-potency agents have some potential for systemic absorption that leads to problems of adrenal suppression and growth retardation in children, this is uncommon and has not been observed with continuous use of mild- or moderate-potency corticosteroids.31,32
Figure 9.

Atrophy on flexural surface of the arm caused by long-term application of topical corticosteroids.
Figure 10.

Dramatic striae and telangiectasia caused by long-term oral corticosteroid use.
TOPICAL CALCINEURIN INHIBITORS
Topical calcineurin inhibitors, such as pimecrolimus (Elidel) and tacrolimus (Protopic), are immunomodulators and are considered second-line therapy.12 They generally are reserved for short-term or intermittent long-term therapy in persons with moderate to severe atopic dermatitis, especially when there is concern that ongoing use of topical corticosteroids is causing adverse effects, such as atrophy.15 Because these agents do not lead to skin atrophy, they are particularly useful for areas of thinner skin on the face, neck, and skin folds. Another benefit is that they do not demonstrate tachyphylaxis (i.e., a decrease in response to a medication when it is used repeatedly), even after prolonged treatment.33
In studies comparing the effectiveness of these agents, tacrolimus has been at least slightly more effective than pimecrolimus in the treatment of moderate to severe atopic dermatitis.34 Pimecrolimus is considered weaker than moderate or potent corticosteroids, but there have not been good studies comparing it with mild corticosteroids.16 Tacrolimus 0.1% has been shown to be at least as effective as a potent corticosteroid in adults, and more effective (at 0.1% or 0.03%) than a weak corticosteroid in children.17
The U.S. Food and Drug Administration issued a boxed warning for pimecrolimus and tacrolimus regarding reports of a possible link to lymphomas and skin malignancies. There also is concern about the possibility that these agents can cause systemic immunosuppression. However, studies to date have demonstrated no clear link to these malignancies, significant systemic absorption, or immunosuppression.18–23 Additionally, the American Academy of Dermatology did not find sufficient evidence linking these agents to malignancies, and stated that systemic immunosuppression is unlikely if continuous long-term use is avoided.15
ANTIBIOTICS
Patients with atopic dermatitis often are heavily colonized with Staphylococcus aureus, although colonization with methicillin-resistant S. aureus is uncommon.35 Studies have not demonstrated any benefits from antibiotic treatment in reducing atopic dermatitis flare-ups.24,25 However, when a patient has a secondary infection, short courses of oral antistaphylococcal agents are recommended for widespread infection, and topical agents, such as mupirocin (Bactroban) can be used for localized infection.11,36
ANTIHISTAMINES
Oral antihistamines are not recommended for the routine treatment of atopic dermatitis because they are not effective in treating the associated pruritus.25,37
SYSTEMIC AND ULTRAVIOLET PHOTOTHERAPY
For patients with conditions that are refractory to treatment with topical agents or who have severe widespread atopic dermatitis, options such as ultraviolet phototherapy and systemic immunomodulatory agents (e.g., cyclosporine [Sandimmune], interferon gamma-1b) can be prescribed under the guidance of a dermatologist.12,25 Rarely, short-term oral courses or intramuscular injections of corticosteroids can be used to treat severe atopic dermatitis flare-ups.13
COMPLEMENTARY AND ALTERNATIVE THERAPIES
The effectiveness of homeopathy, hypnotherapy/biofeedback, and massage therapy for the treatment of atopic dermatitis has not been established.11,12 Chinese herbal mixtures may demonstrate some effectiveness based on four small randomized controlled trials, but larger well-designed studies are lacking.38 Other forms of treatment (e.g., fish oil, vitamin E, minerals, multivitamins, probiotics) are not supported by evidence.12,25,39
Data Sources: We searched PubMed under clinical queries using the following terms: atopic dermatitis, eczema, prevalence of atopic eczema USA, diagnostic criteria atopic dermatitis, complications of atopic dermatitis, eczema herpeticum, atopic dermatitis treatment, safety reports on pimecrolimus and tacrolimus, and alternative treatments for atopic dermatitis. We also searched Essential Evidence Plus, the Agency for Healthcare Research and Quality Clinical Guidelines and Evidence Reports, the Institute for Clinical Systems Improvement, the National Guideline Clearinghouse, the U.S. Preventive Services Task Force, Clinical Evidence, the Cochrane Database of Systematic Reviews, Dynamed, and UpToDate. The search included meta-analyses, randomized controlled trials, clinical trials, and systematic reviews. Search dates: between March 14, 2011, and May 19, 2011.
