
Am Fam Physician. 2013;87(10):723-724
Author disclosure: No relevant financial affiliations.
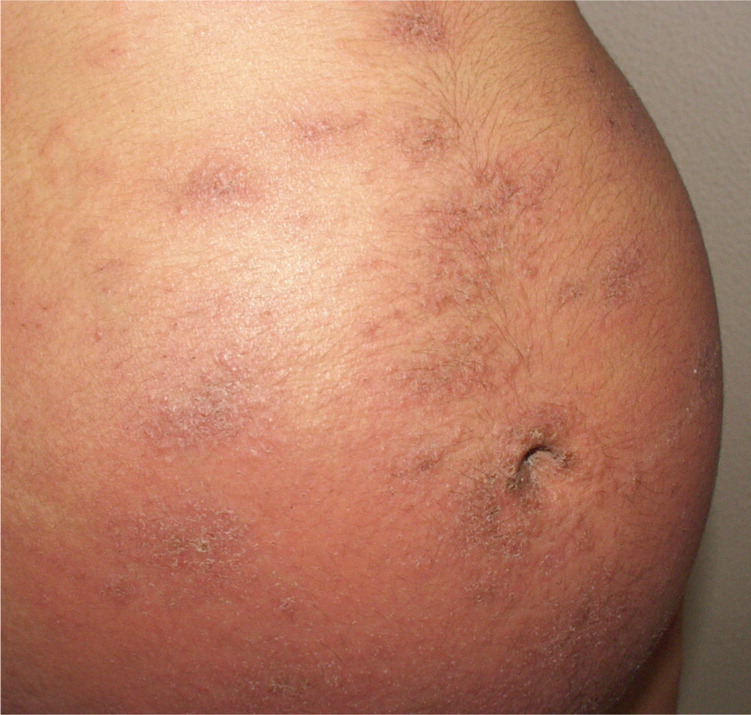
A 28-year-old woman presented with a pruritic rash at 32 weeks' gestation. The rash, which first appeared 20 days earlier, started in the periumbilical area, then became widespread. The physical examination revealed urticarial, eczematous plaques with erosive and crusted blisters on her arms, chest, back, and abdomen (Figures 1 and 2). The striae gravidarum were spared.

She was taking iodine, folic acid, iron, and vitamin B12. She was otherwise healthy and had no significant medical history. Results of a complete blood count and metabolic profile were normal.
Question
Discussion
The answer is C: pemphigoid gestationis (herpes gestationis). Pemphigoid gestationis is a rare autoimmune, blistering dermatosis of pregnancy that occurs in one out of 50,000 pregnancies.1 The disease usually occurs in the third trimester and is characterized by severe pruritus followed by an extended eruption that begins in the periumbilical area. Lesions consist of urticarial and eczematous papules, plaques, blisters, and vesicles. Mucous membranes and striae gravidarum are generally spared.
The rash may disappear in the last weeks of pregnancy, followed by a postpartum flare-up. Skin involvement occurs in up to 10 percent of infants delivered to mothers with pemphigoid gestationis. Premature delivery and intrauterine growth retardation may occur in 20 percent of pregnancies affected by the condition. Early appearance of the rash is associated with a higher rate of fetal complications.1 Postpartum flare-ups may occur with menstruation or with oral contraceptive use in up to 25 percent of patients.2 If the rash recurs in subsequent pregnancies, it usually has a more severe course than in the earlier pregnancy.
Up to 10 percent of pemphigoid gestationis cases are related to autoimmune disorders and hydatidiform moles. The histopathology of a skin biopsy will demonstrate a perivascular infiltrate of lymphocytes and eosinophils and a subepidermal blister. Oral antihistamines are the standard treatment, with prednisone reserved for more severe cases.3
A drug eruption presents as a pruritic, erythematous rash on the trunk and extremities, usually within hours of taking the drug. Palms and soles may be affected. Systemic and mucosal involvement and blistering may occur in severe cases.
Intrahepatic cholestasis of pregnancy is a liver disorder that occurs in the third trimester. It is characterized by maternal pruritus affecting the palms and soles, and increased rates of preterm labor and adverse fetal outcomes.4,5 There are no dermatologic features, except for excoriation from the pruritus. Jaundice occurs in up to 15 percent of persons with the condition.5
PUPPP is a common disease that occurs in the third trimester of pregnancy. It does not cause systemic symptoms. The rash begins as pruritic papules and plaques on the striae gravidarum and spreads to the rest of the abdomen and extremities. PUPPP is more common in twin and first pregnancies.6 It does not cause fetal complications.
Approximately five out of 10,000 pregnant women have varicella (chickenpox).7 It causes fever and a disseminated pruritic, vesicular, umbilicated rash with crusted lesions. If the infection occurs in the first 20 weeks of gestation, it can be transmitted to the fetus.
| Condition | Characteristics | Fetal risks |
|---|---|---|
| Drug eruption | Pruritic, erythematous rash on the trunk and extremities; systemic and mucosal involvement and blistering in severe cases | None |
| Intrahepatic cholestasis of pregnancy | Intense pruritus with no dermatologic features; jaundice is possible | Preterm labor |
| Pemphigoid gestationis (herpes gestationis) | Severe pruritus; subepidermal blisters and urticarial, eczematous rash; starts in periumbilical region | Premature delivery; intrauterine growth retardation |
| Pruritic urticarial papules and plaques of pregnancy | Pruritic papules and plaques; starts on the pregnancy striae; no systemic symptoms | None |
| Varicella (chickenpox) | Pruritic, vesicular, umbilicated rash; disseminated; fever | Congenital varicella |
