Otalgia (ear pain) is a common presentation in the primary care setting with many diverse causes. Pain that originates from the ear is called primary otalgia, and the most common causes are otitis media and otitis externa. Examination of the ear usually reveals abnormal findings in patients with primary otalgia. Pain that originates outside the ear is called secondary otalgia, and the etiology can be difficult to establish because of the complex innervation of the ear. The most common causes of secondary otalgia include temporomandibular joint syndrome and dental infections. Primary otalgia is more common in children, whereas secondary otalgia is more common in adults. History and physical examination usually lead to the underlying cause; however, if the diagnosis is not immediately clear, a trial of symptomatic treatment, imaging studies, and consultation may be reasonable options. Otalgia may be the only presenting symptom in several serious conditions, such as temporal arteritis and malignant neoplasms. When risk factors for malignancy are present (e.g., smoking, alcohol use, diabetes mellitus, age 50 years or older), computed tomography, magnetic resonance imaging, or otolaryngology consultation may be warranted.
Patients with otalgia (ear pain) commonly present to their primary care physician. Pain that originates from the ear is known as primary otalgia, whereas pain that originates outside the ear is secondary otalgia. A comprehensive history and physical examination are essential to determine the etiology of primary or secondary otalgia.
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendation | Evidence rating | References |
|---|---|---|
| The diagnosis of acute otitis media requires moderate to severe bulging of the tympanic membrane, new onset of otorrhea not caused by otitis externa, or mild bulging of the tympanic membrane associated with recent onset of ear pain (less than 48 hours) or erythema. | C | 9 |
| Magnetic resonance imaging and referral for nasolaryngoscopy are recommended in the setting of otalgia with normal ear examination findings and symptoms of or risk factors for tumor. Laboratory evaluation with a complete blood count and erythrocyte sedimentation rate can be helpful. | C | 2, 14 |
| Patients 50 years and older with otalgia and a normal ear examination should be evaluated for temporal arteritis. | C | 14 |
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to http://www.aafp.org/afpsort.
Primary otalgia is more common in children, whereas secondary otalgia is more common in adults.1,2 The etiology of primary otalgia, which is usually identified on examination of the ear, is typically otitis externa or otitis media.3 The etiology of secondary otalgia is more complex because the nerves innervating the ear have a shared distribution to include the head, neck, chest, and abdomen2,4 (Figure 1). [corrected] The ear is innervated by several sensory nerves. The auricle is affected by cranial nerves V, VII, X, C2, and C3; the external auditory meatus and canal by cranial nerves V, VII, and X; the tympanic membrane by cranial nerves VII, IX, and X; and the middle ear by cranial nerves V, VII, and IX. Irritation of any portion of these nerves can result in otalgia.
FIGURE 1.
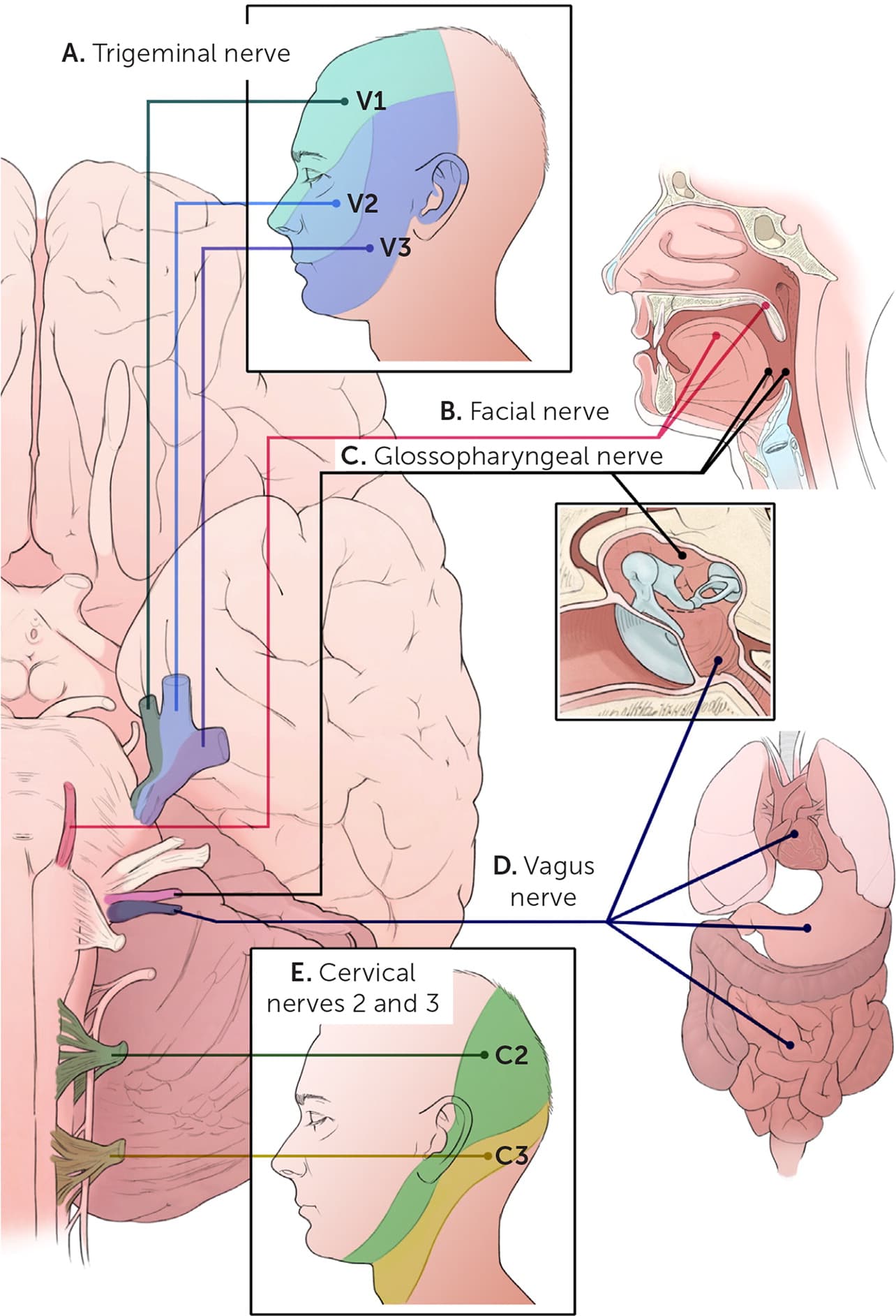
Sensory distribution of the nerves innervating the ear. (A) Trigeminal nerve (V): face, sinuses, teeth. (B) Facial nerve (VII): anterior two-thirds of the tongue, soft palate. (C) Glossopharyngeal nerve (IX): posterior one-third of the tongue, tonsils, pharynx, middle ears. (D) Vagus nerve (X): heart, lungs, trachea, bronchi, larynx, pharynx, gastrointestinal tract, middle ears. (E) Cervical nerves 2 and 3 (C2 and C3): external ears, ear canals, anterior region of the neck, posterior region of the neck.
Illustration by Catherine Delphia [corrected]
History
To determine the differential diagnosis of otalgia, the following factors should be considered: pain location, duration, aggravating factors, alleviating factors, associated symptoms, previous episodes, medical history, smoking status, and alcohol abuse.5 Symptoms such as otorrhea, tympanic membrane fullness, and vertigo suggest primary otalgia,3–5 whereas pain with chewing, sinusitis, dental procedures, and a history of gastroesophageal reflux suggest secondary otalgia.4–6 In adults, the absence of hearing loss is a cardinal finding associated with nonotologic disease.5 The character of pain also provides important clues. Pain that is continuous and progressively worsens is more likely to be associated with infection and primary otalgia. Intermittent pain is likely to be associated with secondary otalgia.2
Physical Examination
The physician should start the examination by asking the patient to localize the pain, which may reveal a secondary cause (e.g., localization to the temporomandibular joint [TMJ], myofascial pain localized to the mastoid process). Physical examination should include inspection of the auricle and periauricular region, as well as an otoscopic examination to visually inspect the tympanic membrane and the external auditory canal. Specific otoscopic examination findings for the etiology of otalgia are listed in Table 15,7 and Table 2.5,8 Detection of a middle ear effusion with moderate to severe bulging of the tympanic membrane, new-onset otorrhea not caused by otitis externa, or mild bulging of the tympanic membrane with recent onset of ear pain (less than 48 hours), especially with erythema, is key in the diagnosis of acute otitis media. The tympanic membrane is normally mobile, translucent, and intact. A tympanic membrane that has normal color and mobility is not typical for acute otitis media.9 Patients with otitis externa typically have pain, redness, swelling, and inflammation along the external auditory canal.
TABLE 1. Etiology of Primary Otalgia
| Etiology | History | Physical examination | Additional information |
|---|---|---|---|
| Common causes | |||
| Barotrauma | Pain starts while scuba diving or while flying in an airplane; patient may have experienced a recent blast injury | Tympanic membrane can show middle ear hemorrhage | Prevent with use of topical nasal decongestants or autoinflation |
| Eustachian tube dysfunction | Symptoms of pressure dysregulation | Tympanic membrane retraction or positive tympanographic findings | Also associated with aural fullness and intermittent symptoms7 |
| Foreign object | Commonly insects, small toys, peanuts; most common in children | Foreign object visible in ear canal | May require general anesthesia to remove |
| Otitis externa | Recent swimming with history of discharge | Pain with pulling on external ear; discharge may be present | More common in summer |
| Otitis media | Recent upper respiratory tract infection; children may pull on ears | Red, inflamed, cloudy tympanic membrane | Most common cause of ear pain |
| Uncommon causes | |||
| Cellulitis of auricle | Preceding insect bite, scratch, or piercing; rapid progression | Earlobe usually involved | Must treat aggressively; parenteral antibiotics may be required |
| Cholesteatoma | Sense of fullness | A pearly mass may be visible through the tympanic membrane; often infected with visible squamous material | May be asymptomatic early, but generally associated with hearing loss and otorrhea |
| Granulomatosis with polyangiitis (Wegener granulomatosis) | Arthralgia, hearing loss, myalgias, oral ulcers, otorrhea, and rhinorrhea | Often with chronic otitis media or serous otitis | Consider testing for antineutrophil cytoplasmic autoantibodies |
| Malignant otitis externa | Retroauricular pain; often associated with diabetes mellitus and immunocompromised state; consider in persons with no improvement in otitis externa | Granulation tissue may be present in the external auditory canal Lower cranial neuropathies (VII, X, XI, XII) | Easy to miss with subtle findings; technetium bone scan can be used to determine the extent of disease |
| Mastoiditis | Recent otitis media that is typically chronic but may be acute | Tender edematous mastoids | Uncommon, but prevalence is increased in children with decreased access to health care |
| Ramsay Hunt syndrome (herpes zoster oticus) | Pain can be present before lesions develop; may be associated with hearing loss, vertigo, or tinnitus | Vesicular rash on auricle or ear canal with possible palsy of cranial nerve VII | Can also involve cranial nerves V, IX, and X; pain can occur without eruption |
| Relapsing polychondritis | Recurrent swelling of the auricle; hearing loss | Earlobe is typically not involved because it has no cartilage | Noninfectious; other cartilaginous sites (trachea, nose, bronchi) can be affected |
| Trauma | Blunt trauma, frostbite, burns | Evidence of the trauma | Most common is laceration of the auricle |
| Tumors or infected cysts | Pain usually well localized to auricle or ear canal | Similar presentation to chronic otitis media or externa but nonresponsive to therapy | May be confused with chronic inflammation; if nonresponsive to therapy, timely otolaryngology referral is advised |
| Viral myringitis | Similar presentation to acute otitis media | Tympanic membrane red but not bulging; hemorrhagic bullae of tympanic membrane and ear canals are typical | Bullous myringitis is not pathognomonic of viral meningitis, but commonly presents in that fashion |
Adapted with permission from Ely JW, Hansen MR, Clark EC. Diagnosis of ear pain. Am Fam Physician. 2008;77(5):623, 625, with additional information from reference 7.
TABLE 2. Etiology of Secondary Otalgia
| Etiology | History | Physical examination | Additional information |
|---|---|---|---|
| Subacute etiologies | |||
| Bell palsy | Retroauricular pain that is less severe than with Ramsay Hunt syndrome | Facial weakness that involves the forehead with otherwise unremarkable examination | Pain may occur in only 50% of patients |
| Carotidynia | May have dysphagia or throat or neck tenderness radiating to the ear | Tender carotid artery | More common in women and often self-limited |
| Cervical adenopathy | Recent upper respiratory tract infection | Tender cervical lymph nodes | Consider biopsy or imaging for lymph nodes > 1.5 cm and lasting longer than two months |
| Cervical spine arthritis | Pain with neck movement | Reduced range of motion; tense paraspinal muscles | Referred pain from C2 and C3 cervical nerve roots |
| Cricoarytenoid arthritis | Pain is worse with talking, swallowing, or coughing | Inflammatory arthritis | Likely caused by rheumatoid arthritis or systemic lupus erythematosus |
| Dental causes (caries, abscess, pulpitis) | Dental symptoms | Caries; abscess; gingivitis; facial swelling | Caries and abscess are the most common causes |
| Gastroesophageal reflux | Acid reflux | Unremarkable | Pain from irritation of cranial nerves IX and X |
| Head and neck tumors | Increased risk: smoking, alcohol use, age ≥ 50 years, radiation exposure, weight loss | Possible painless neck mass, or no unusual findings; consider fiberoptic nasolaryngoscopy | Consider early referral; imaging should be coordinated with the otolaryngologist; pain is worse with swallowing, especially acidic or spicy foods |
| Idiopathic | Variable | Unremarkable | Often diagnosed as neuropathic pain, TMJ syndrome, or eustachian tube dysfunction |
| Myofascial pain | Cervical pain may be aggravated by chewing or neck movement | Likely to have trigger point in the neck or mastoid tip at attachment of sternocleidomastoid muscle | Consider TMJ, cervical spine, or dental disorders |
| Neuralgias (trigeminal, glossopharyngeal, geniculate, sphenopalatine) | Pain usually lasts seconds and is episodic, possibly with a trigger | May have trigger point, but typically the examination is unremarkable | Trigeminal is most common |
| Oral aphthous ulcers | Localized pain in mouth but may refer to ear | Shallow ulcers inside mouth, usually gray | Recurrent etiology not well understood |
| Pharyngitis or tonsillitis | Sore throat | Pharyngeal erythema; tonsillar exudate | Ear may not be directly involved |
| Psychogenic | History of depression or anxiety | Variable affect | May be previously diagnosed as idiopathic |
| Salivary gland disorders | Pain in preauricular area | Prominent parotid glands | Recent mumps outbreaks in United States; more commonly purulent parotitis associated with dehydration or stone obstruction |
| Sinusitis | Recent upper respiratory infection | Nasal congestion, purulent nasal discharge, anosmia | Otalgia from sinusitis is unusual |
| Thyroiditis (rarely causes isolated otalgia) | May have tender thyroid | Enlarged or tender thyroid | Pain is referred from the vagus nerve |
| TMJ syndrome | Pain/clicking with opening jaw | Tender TMJ; crepitus on motion of mandible | Leading cause of secondary otalgia in adults; risk factors include clenching and biting lips/mouth, gum chewing |
| Acute etiologies requiring immediate identification | |||
| Myocardial infarction | Risk factors for coronary artery disease | Unstable vital signs | If suspected, start immediate acute coronary syndrome workup |
| Temporal arteritis | Age ≥ 50 years; jaw claudication; diplopia | May be tender along temporal artery; may see prominent artery | Erythrocyte sedimentation rate ≥ 50 mm per hour Biopsy and immediate treatment to prevent blindness Consider early referral |
| Thoracic aneurysms | Older men; hypertension; risk factors for coronary artery disease | May have unstable vital signs | Computed tomography or magnetic resonance angiography |
| Other rare causes (subdural hematoma, lung cancer, central line placement, carotid artery aneurysm, Pott puffy tumor) | Variable | Variable | Pott puffy tumor is typically a complication of prolonged sinusitis with no treatment8 |
TMJ = temporomandibular joint.
Adapted with permission from Ely JW, Hansen MR, Clark EC. Diagnosis of ear pain. Am Fam Physician. 2008;77(5):624, 626, with additional information from reference 8.
The examination also includes traction on the auricle and palpation of the tragus to differentiate disease processes affecting the external ear and ear canal (most commonly otitis externa).10 Finding vesicles in the ear canal or on the external ear may indicate herpes zoster oticus (Ramsay Hunt syndrome). If the auricular examination is unremarkable, a complete head and neck examination should also be performed, paying special attention to the TMJ and the nasal and oral cavities. TMJ syndrome commonly presents with discomfort or crepitus on palpation of the TMJ. A variety of dental causes of otalgia can be identified by evaluating the oral cavity with palpation and percussion of the gum line and teeth, specifically the molars.11 Evaluation of the oropharynx may also result in findings diagnostic of pharyngitis and other oropharyngeal disorders that can radiate pain to the ear.
Patients with abnormal vital signs who present initially with otalgia may have a serious infection, such as meningitis or sepsis, or serious traumatic injury, such as epidural hematoma. Patients with ear pain and abnormal mental status must be evaluated for traumatic injury, epidural infection, and osteomyelitis.8
Evaluation
The diagnosis of primary otalgia rarely requires more than a history and physical examination (Figure 2).5 Likewise, most cases of secondary otalgia can be diagnosed with a history and physical examination. Concerning historical features include progressive or unrelenting symptoms, unintentional weight loss, exertional pain, behavioral risk factors (e.g., tobacco exposure, heavy alcohol consumption), medical history (e.g., immunocompromised state, coronary artery disease, cancer, diabetes mellitus), and new-onset symptoms in patients 50 years or older. When the physical examination is unremarkable (especially if there are concerning historical features), nasolaryngoscopy, tympanometry, audiometry, and laboratory evaluation with a complete blood count and erythrocyte sedimentation rate can be helpful. Magnetic resonance imaging, computed tomography, and, if there is a history of cancer, positron emission tomography may be performed to provide further information.2,5,12–14 Advanced imaging for evaluation of otalgia may be most efficiently ordered in consultation with an otolaryngologist.
FIGURE 2.
Algorithm for the evaluation of ear pain.
NSAID = nonsteroidal anti-inflammatory drug; TMJ = temporomandibular joint.
Adapted with permission from Ely JW, Hansen MR, Clark EC. Diagnosis of ear pain. Am Fam Physician. 2008;77(5):622.
Primary Otalgia
Primary otalgia can be further delineated into pain originating from the external ear, ear canal, or middle ear (Table 1).5,7 External ear pain can be due to several factors, including trauma, sunburn, acute folliculitis, contact dermatitis, shingles, and other skin conditions. When trauma is suspected, the temporal and parietal regions of the skull should be assessed and appropriate imaging ordered. Disorders of the external auditory canal that may cause pain include cerumen impaction, foreign bodies, and, most commonly, infection of the canal.
Otitis externa (commonly known as swimmer's ear) is caused by bacterial infections (90%) and fungal infections (10%).5,15 Ear pain originating in the middle ear is typically due to acute otitis media, but can also be from bullous myringitis, barotrauma, and eustachian tube dysfunction.16 Otitis media is most commonly caused by Streptococcus pneumoniae, Moraxella catarrhalis, or Haemophilus influenzae.9 Eustachian tube dysfunction is also a common cause of primary otalgia, affecting an estimated 3% of patients presenting with otalgia.4 A consensus definition of eustachian tube dysfunction is signs and symptoms of pressure dysregulation in the middle ear diagnosed with otoscopic evidence of tympanic membrane retraction and/or tympanogram indicating negative middle ear pressure.17 Bullous myringitis is uncommon, but occurs when serous or hemorrhagic blisters form in the ear canal or on the lateral tympanic membrane (usually caused by a bacterial or viral infection); symptoms generally include sudden onset of severe ear pain and hearing loss.16 Pain often decreases after bullae rupture and drain.
Uncommon causes of primary otalgia include infectious, neoplastic, and inflammatory etiologies. Mastoiditis, an infection in the air cells of the skull behind the ear, is a rare complication from acute otitis media. This diagnosis is based on physical examination findings of tenderness, erythema, edema, and warmth in the mastoid region.18 Malignant otitis externa is a rare condition found in patients with diabetes or who are immunocompromised. It is characterized by severe unrelenting pain and a subtle finding of inferior external auditory canal granulation tissue at the bony cartilaginous junction. Pseudomonas infection involving the skull base (osteitis) can result in lower cranial neuropathies.19 Herpes zoster oticus is caused by reactivation of latent herpes zoster infection from the geniculate ganglion (cranial nerve VII or facial nerve), but also can involve cranial nerves V, IX, and X. Symptoms include ear pain and facial paralysis while the patient has vesicles in the external auditory canal.5
Cholesteatomas may produce a sense of fullness rather than severe pain but may also be asymptomatic. An epidermal cyst develops in the superior, usually posterior, aspect of the tympanic membranes. The cyst can cause conductive hearing loss secondary to local destruction of middle ear structures and may present with otorrhea consisting of desquamating epithelium.5 Relapsing polychondritis is a rare systemic disease involving the cartilage of many organs, but most commonly the ears. It is characterized by a relapsing, bilateral, erythematous or violaceous appearance on the external ear, sparing the ear lobes.2
Secondary Otalgia
The complex embryologic development of the ear results in neural connections to several cranial and cervical nerves. These nerves provide sensory innervation to regions of the head, neck, chest, and abdomen, which can result in referred pain to the ear 14 (Figure 1 and Table 25,8 ). Referred pain from the trigeminal nerve (cranial nerve V) is the most common source of secondary otalgia stemming from TMJ syndrome, dental infections, trigeminal neuralgia, sinusitis, and mandibular osteomyelitis or tumor.4 Herpes zoster can affect cranial nerve VII to a lesser degree than in Ramsay Hunt syndrome, which can also cause ear pain associated with Bell palsy and an unremarkable ear examination.4 Cranial nerve IX can refer pain caused by tonsillitis, pharyngitis, pharyngeal tumor, or glossopharyngeal neuromas.4 The vagus nerve affects many systems as inferior as the colon and can be activated by any vagal stimulation. Otalgia has been reported as the presenting symptom of myocardial ischemia from irritation of the vagus nerve.20
Secondary otalgia can be caused by irritation of C2 and C3 cervical nerve roots, especially in patients with cervical spine degeneration. Tumor, infection, or an inflammatory process within the sensory distribution of any of these nerves may cause referred pain to the ear.4 An example of this is temporal arteritis, which presents with temporal pain in only 40% of patients. Temporal arteritis should be considered in patients 50 years or older who have normal ear examination findings and any of the following symptoms: headache, malaise, weight loss, fever, or anorexia. Permanent blindness may result if systemic steroids are not initiated promptly. In suspected cases, an elevated erythrocyte sedimentation rate (50 mm per hour or greater) warrants immediate treatment with systemic steroids and surgical consultation to confirm the diagnosis.14
Risk Factors for a Serious Diagnosis in Patients with Otalgia
There are some characteristics that make a serious diagnosis more likely in patients with otalgia. Treatment is most effective when there is minimal delay after diagnosis. Patients who are 50 years or older, have coronary artery disease, have diabetes, or are immunocompromised are at higher risk. In addition, patients who smoke, drink alcohol, or lose weight unintentionally should undergo more scrutiny. Consumption of 50 g or more of alcohol per day (approximately 3.5 or more drinks per day) increases the risk of head, neck, and esophageal cancers by two to three times compared with nondrinkers; smoking and drinking alcohol increase the risk compared with alcohol use alone.21 In addition, unilateral hearing loss warrants further investigation if an obvious cause (e.g., cerumen impaction, foreign body) is not apparent.5
This article updates a previous article on this topic by Ely, et al.4
Data Sources: A PubMed search for evaluation and diagnosis of ear pain or otogenic otalgia or primary otalgia or secondary otalgia or otalgia was performed. The search was further limited by English only, human studies, and over the past five years. In addition to this search, we used articles from the reference list of the 2008 AFP article on ear pain,5 as well as reference lists of articles selected from our PubMed search. Search dates: July 27, 2016, and April 10, 2017.
The views expressed in this article are those of the authors and do not reflect the policy or position of the U.S. Army Medical Department, Department of the Army, Department of Defense, or the U.S. government.
