
Am Fam Physician. 2019;100(3):176-178
Author disclosure: No relevant financial affiliations.
A healthy 21-year-old male soldier stationed in Qatar presented with abdominal cramping that began two weeks prior. The pain, which he rated as a 7 out of 10, was brought on by eating. Although this resulted in him eating less to avoid the pain, he did not have significant weight loss. No foods in particular made his cramping worse. It was associated with nausea and watery diarrhea, which resolved one week prior. He did not have bloody stools, melena, night sweats, weakness, fevers, or chills. He had never had abdominal surgery, did not take any medications, and had no significant personal or family history. He had three similar episodes in the previous year, which occurred before his deployment to Qatar.
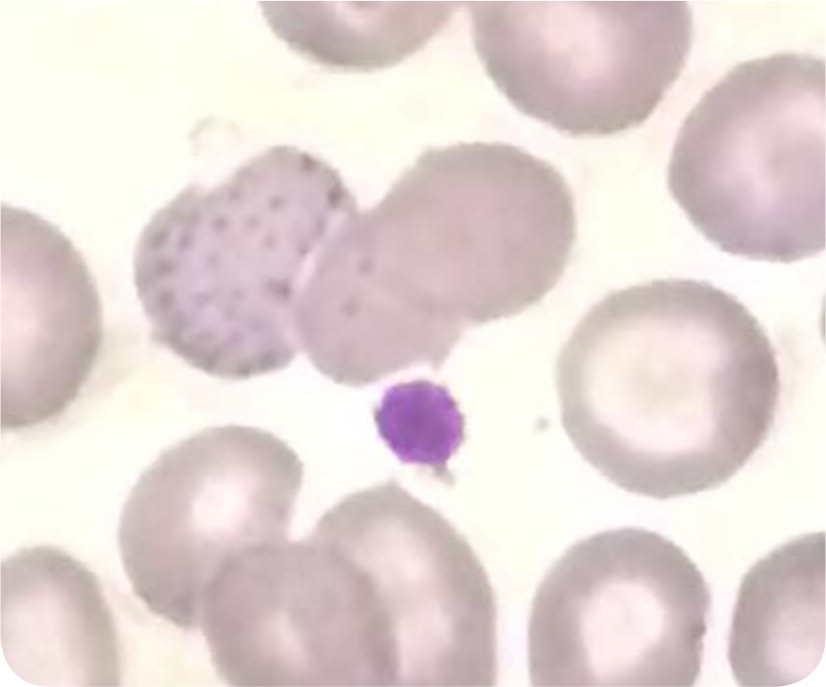
On physical examination, his vital signs were normal. His abdomen was mildly tender but the pain was nonfocal. Results of laboratory tests, including electrolyte and amylase measurements and liver function testing, were normal. Stool guaiac testing was negative. Findings on computed tomography of the abdomen and pelvis were normal. The complete blood count was significant for microcytic hypochromic anemia with hemoglobin (Hb), hematocrit, mean corpuscular volume, and mean corpuscular Hb concentration of 11.8 g per dL (118 g per L), 38.4%, 63 μm3 (63 fL), and 30.7 g per dL (307 g per L), respectively. The peripheral smear is shown in Figure 1.
Question
Discussion
The answer is A: beta-thalassemia, specifically the minor type. Beta-thalassemia is an inherited disorder that is the result of mutations of the beta-globin gene (HBB) on chromosome 11. Phenotypic variability is designated as minor, intermedia, or major. The minor type is a carrier state often discovered incidentally with a routine complete blood count. Beta-thalassemia is more common in people of Mediterranean, African, or Southeast Asian descent. It is characterized by microcytic hypochromic anemia. In addition, target cells, teardrop cells, and often coarse basophilic stippling can be seen on the peripheral blood smear. This patient's peripheral smear showed target cells and a single cell with basophilic stippling.
Diagnosis requires Hb electrophoresis or high-performance liquid chromatography demonstrating abnormal percentages of HbA, HbA2, and HbF. In this patient, Hb electrophoresis revealed a typical pattern for beta-thalassemia with a decreased HbA at 92.7% and an increased HbA2 at 5.7%.1 Other causes of elevated HbA2 include antiretroviral therapy, vitamin B12/folate deficiency, and hyperthyroidism. Genetic counseling and prenatal diagnosis may be indicated for carriers.2 As many as 60% of patients with thalassemia have chronic pain.3
Celiac disease is an immune-based reaction to dietary gluten, primarily affecting the small intestine in those with a genetic predisposition. It resolves with the elimination of dietary gluten. It can present with gastrointestinal symptoms or nongastrointestinal signs and symptoms, such as abnormal results on liver function tests, iron deficiency anemia, bone disease, and skin disorders. Celiac disease is detected by serologic testing of celiac-specific antibodies and confirmed with duodenal mucosal biopsies.4
Gastric lymphoma is the most common extranodal non-Hodgkin lymphoma. Initial symptoms are usually nonspecific but may mimic gastritis, peptic ulcer disease, pancreatic disorders, or functional disorders of the stomach. The most common symptoms include weight loss, nausea, vomiting, abdominal fullness, and indigestion. Physical examination findings are usually unremarkable, but some patients may exhibit epigastric tenderness, adenopathy, or a palpable epigastric mass. It is commonly diagnosed with a gastric biopsy performed during esophagogastroduodenoscopy, but it may also be diagnosed with endoscopic ultrasonography, computed tomography, magnetic resonance imaging, or positron emission tomography.5
Infectious mononucleosis is caused by the Epstein-Barr virus and is common among teenagers and young adults. It is characterized by fever, pharyngitis, adenopathy, and fatigue. Other, less common manifestations include splenomegaly and rash, but Epstein-Barr virus infection can affect virtually any organ system.6 Hematologic abnormalities include lymphocytosis (most common), hemolytic anemia, thrombocytopenia, aplastic anemia, thrombocytopenic purpura, and disseminated intravascular coagulation.7,8
Lead toxicity usually results from occupational exposure, but nonoccupational exposure from herbal medicines, cosmetics, and paint in older buildings has also been reported. It most commonly affects the central and peripheral nervous systems, renal function, vascular system, and gastrointestinal tract. Lead exposure can reduce circulating levels of Hb, manifesting as micro-cytic hypochromic anemia. Common peripheral smear findings include basophilic stippling of erythrocytes due to clustering of ribosomes and microcytosis.9
| Diagnosis | Characteristics |
|---|---|
| Beta-thalassemia | An inherited disorder that is a result of mutations of the beta-globin gene (HBB); the minor type is a carrier state often discovered incidentally with a routine complete blood count; genetic counseling and prenatal diagnosis may be indicated for carriers |
| Celiac disease | Immune-based reaction to dietary gluten, primarily affecting the small intestine; may lead to gastrointestinal symptoms or nongastrointestinal signs and symptoms, such as abnormal liver function tests, iron deficiency anemia, bone disease, and skin disorders |
| Gastric lymphoma | The most common extranodal non-Hodgkin lymphoma; symptoms may mimic gastritis, peptic ulcer disease, pancreatic disorders, or functional disorders of the stomach; the most common symptoms include weight loss, nausea, vomiting, abdominal fullness, and indigestion; physical examination findings are typically unremarkable |
| Infectious mononucleosis | Caused by the Epstein-Barr virus; common among teenagers and young adults; fever, pharyngitis, adenopathy, and fatigue; splenomegaly and rash are less common manifestations |
| Lead toxicity | Usually results from occupational exposures; most commonly affects the central and peripheral nervous systems, renal function, vascular system, and gastrointestinal tract |
The authors thank Lt Col Aaron W. Lambert, senior lab officer, 379th Expeditionary Medical Group, Al Udeid Air Base, Qatar, for preparation of the peripheral smear and image for this case.
The opinions and assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the U.S. Air Force Medical Department or the U.S. Air Force at large.
