Transformations to Reduce Documentation Burden
Learn about organizational changes a practice can make to modify its workflow and operations. Transformations to improve documentation burden range from expanding nonphysician clinicians’ scope of work to adopting an entirely new practice model.
Team-based documentation
Team documentation can ease burden by training medical assistants to assist with the visit and patient note.
Direct primary care (DPC)
Moving from fee-for-service to direct primary care eliminates documentation and most other administrative burdens.
Team documentation can ease burden by having medical assistants (MAs) assist the physician with the visit and patient note. Transforming to a team model requires two main changes to the traditional practice model:
Train your MA to be your scribe and clinical assistant.
The physician teams with their MA to document and act as clinical assistant during the visit. The MA starts the note while the patient is being roomed. After you enter the room, the MA stays and acts as your scribe throughout the visit. The MA becomes your clinical assistant, preparing the patient for the visit and for their after-visit care.
Increase your MA-to-physician ratio.
Family medicine practices typically have each physician partnered with one MA. Team documentation places more responsibility on the MA during each visit, and some practices have responded by adding more MAs. While one MA is working in the room with the physician, a second MA can be rooming the next patient. This team model has been shown to raise productivity, outweighing the additional staffing costs.
Impact
A study that examined the University of Colorado’s Primary Care Redesign team-based model showed the following impact:
- >50% reduction in burnout (from 56% to 22%)
- improved quality metrics
- increased MA-to-clinician ratio (from 1:2 to 2.5:1)
- increased patient access (volume increased by 1.5 patients per 4 hours)
- increased productivity that kept the model cost-neutral
Challenges
Challenges of team documentation transformation include adding staff to increase the MA-to-clinician ratio and training MAs. The organization’s ability to hire and train more MA staff will determine the risk of transformation.
During rooming
The MA handles data gathering, recording the patient’s complaints and asking for additional detail. Protocols and templates can be developed based on specific patient complaints and chronic conditions to direct the MA’s questioning. The assistant also reviews and makes necessary updates to:
- chief complaints (note can be based on chief complaint templates)
- chronic conditions (note can be based on chronic condition templates)
- patient’s medical history
- patient’s surgical history
- social history
- family history
- health maintenance
- pending orders or procedures (e.g., immunizations)
- medication list reconciliation and upcoming refills
Exam room assistance
The MA presents the case to the physician, who reviews the patient's chart. Both enter the exam room together, and the physician greets the patient for the first time.
- The MA remains in the exam room serving as a scribe for the physician.
- The physician reviews accuracy and completeness of the information the MA gathered.
- The physician asks the patient more questions and performs the physical exam, if indicated.
- The MA documents any additional data (e.g., pertinent findings) and enters it into the EHR.
- The physician formulates a diagnosis and care plan with the patient and MA.
- The MA records all diagnoses for the visit and any orders needing the physician's approval.
- The MA may also maintain the problem list.
- The MA records the plan and fills in the details for the after-visit summary.
- The physician exits the exam room to review and file the orders for the encounter.
The physician moves on to the next patient.
MA wraps up visit
The MA remains with the patient and reinforces the physician's instructions by:
- providing prescriptions and referral information
- delivering patient education
- answering questions
- arranging appropriate follow-up
- printing and reviewing an updated medication list and visit summary
Family physicians who report burnout often describe it as being on a “hamster wheel”— always running, rushed, and never caught up. Time caring for patients and time with their families is compromised, and their professional satisfaction has eroded.
Under the fee-for-service (FFS) reimbursement model, physicians cover large patient panels (1,500–2,500 individuals), conduct severely time-restricted visits (~15 minutes) and spend ~40% of their time documenting their work to get paid. For these and other reasons, FFS-based, insurance-driven primary care has been labeled a primary cause of family physician burnout, in contrast to an innovative alternative model to FFS: direct primary care (DPC).
Results
Below are quantitative results and interview findings for 10 clinicians before and after adopting DPC and Hint Health’s DPC membership management solution, HintOS. The results present anecdotal evidence of these clinicians’ experiences based on their reported levels of practice satisfaction, burden, and burnout.
Burnout and burden
Which of the items below describes you best?
- I enjoy my work. I have no symptoms of burnout.
- I am under stress, but I don’t feel burned out.
- I am definitely burning out.
- I think about work frustrations a lot. It won’t go away.
- I feel completely burned out. I may need to seek help.
Practice satisfaction
Clinicians saw a dramatic increase in overall practice satisfaction, with the average score more than doubling from 4.1 to 8.9 on a scale of 1 to 10. When asked what would raise their satisfaction score with their current practice to 10, they often reported they still wanted to grow their patient panels or offer more services. A few reported that feeling outside of the system, although refreshing, was at times frustrating when trying to get information that would assist their patients.
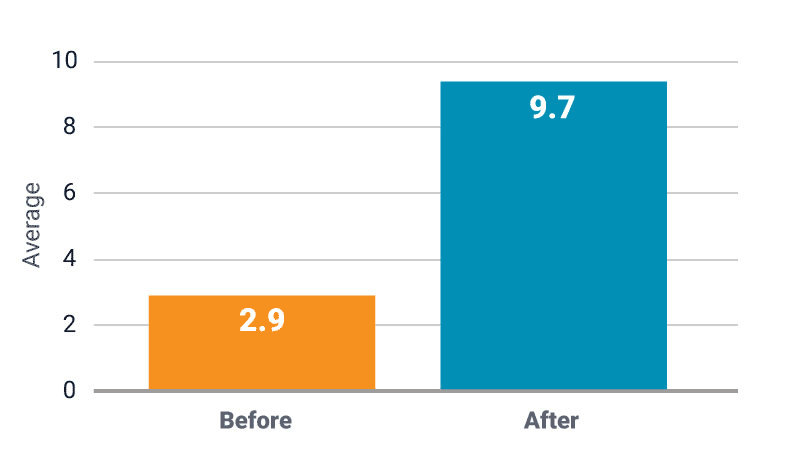
At the heart of clinicians’ responses was their strong dissatisfaction with the practice burdens associated with FFS. They reported low satisfaction under the FFS model—an average of 2.9 on a scale of 1 to 10—with several reporting that they felt they were on a “hamster wheel” and were never able to catch up or get paid adequately. After adopting DPC, they reported a 9.7 satisfaction rating, stating that they no longer worried about or even had to work specifically on getting paid simply for providing care.
Clinicians said that HintOS removed all of the administrative burden that could be associated with the prospective payment membership model because it managed the payments and reminders without clinicians having to insert themselves into the payment process. The only reason they really even needed to go into HintOS, they said, was to see “how well it was going.”
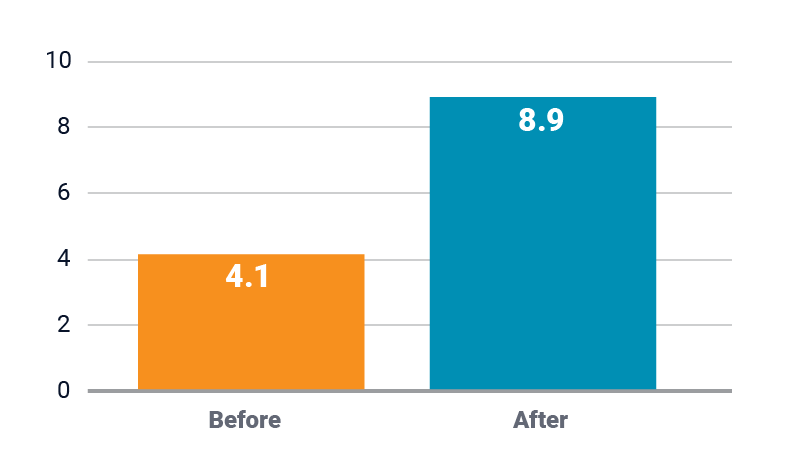
How satisfied are you with your overall practice?
How satisfied are you with FFS and dealing with insurance?
Patient panel size
Regarding patient panel size under FFS, our participants had only three definitive data points (1400, 1500, and 3000 patients), with an average just under 2000 patients. Estimates of typical primary care patient panel size under FFS range from 1500–2500 patients. With an n of 10, the participants reported their DPC patient panel sizes ranged from 150–800, with an average of 453. Most reported their ideal patient panel size would be 500–800 patients. Some wanted to keep their panel size on the smaller end to maintain a good work-life balance.

Patient panel size
Patient visit length and time with patients
Participants reported a threefold increase in typical visit length, going from an average of just under 15 minutes to an average of about 45 minutes. They reported that they thought an ideal FFS visit length should be 30 minutes. Typically under DPC, they would schedule patients for 30–45 minutes for routine visits and 60+ minutes for new patients because they considered these the ideal visit lengths to take care of patients. Their schedule often allowed them to extend these visits as needed.
How would you rate your time with your patients?
- Inadequate
- Constrained
- Adequate
- Ample
In a follow-up to the question about visit length, participants described their time with their patients as moving from between “inadequate” and “constrained” under FFS to unanimously reporting that under DPC, their time with their patients was “ample.”
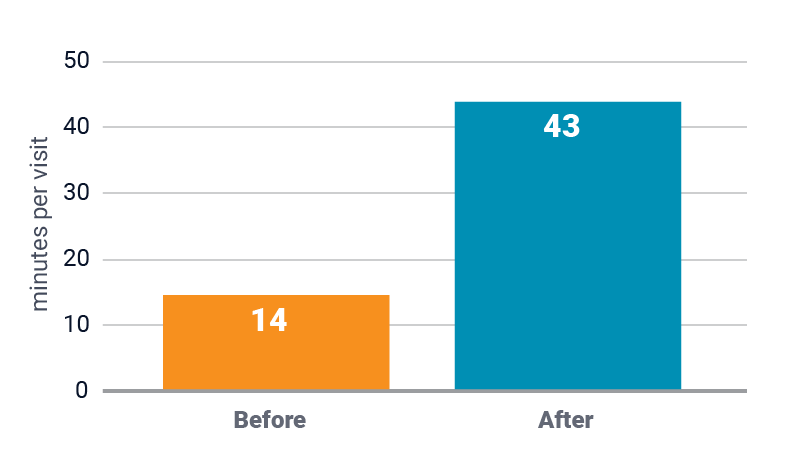
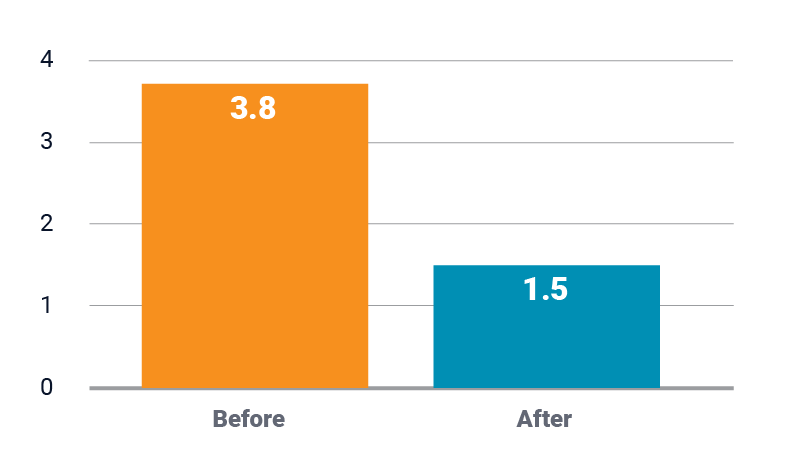
What is your typical visit length?
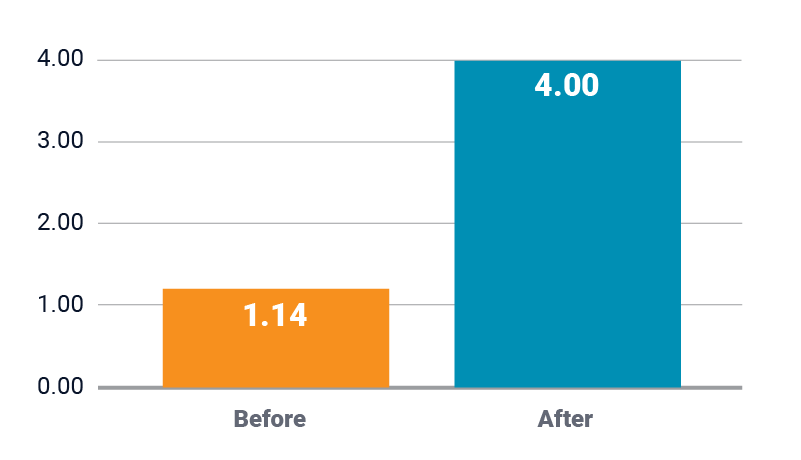
How would you rate your time with patients?
1=Inadequate 2=Constrained 3=Adequate 4=Ample
Suki Lab: AI Assistant for Documentation
Suki is a digital assistant for physicians that combines AI and voice-enabled technology. Suki understands natural language and completes tasks such as note creation and retrieving information from the EHR.
It is possible to use Suki as a standalone solution whereby Suki generates notes in PDF format that can then be saved in your EHR. Although the benefits may not be the same as those seen in the phase one pilot, members reported significant improvements using this nonintegrated workflow. The Suki lab launched in 2019 and has achieved several milestones.