
Am Fam Physician. 1998;58(2):352-354
to the editor: In 1785, Richter1 described hernias in which only part of the bowel wall was strangulated. Since only a small part of the circumference of the bowel is involved in such cases, gangrene can occur without intestinal obstruction. At our hospital, we recently saw what could be the first case of perforated Richter's hernia, with generalized peritonitis, in a patient who was 11 weeks and three days pregnant.
This 29-year-old woman, gravida 5, para 0, abortus 4, presented to the emergency department with diffuse abdominal pain of five days' duration. She had a previous right inguinal hernia that had been repaired six years earlier. In addition to being pregnant, she had a slightly tender and reddened right groin mass that she ascribed to the worsening of a recurrent hernia, which had troubled her over the past year. She had experienced bloating, nausea, vomiting and constipation over the past two days. Her clinical findings were compatible with an acute surgical abdomen.
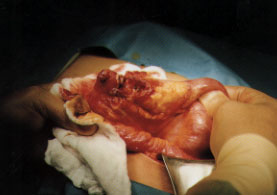
A single upright abdominal film revealed free peritoneal air. On celiotomy, a knuckle of distal ileum was released from its incarceration in a recurrent inguinal hernia. A small perforation was noted (see figure) 3 cm proximal to the incarcerated piece. The involved bowel was resected and the hernia was repaired from the inside. Her pregnancy and allergy to penicillin limited our choice of postoperative antibiotics, but with delayed surgical closure of her abdominal incision combined with judicious antibiotic use, she underwent an uncomplicated recovery. However, she was not able to carry her pregnancy to term. She miscarried at 15 weeks.
In a matched, comparative study of Richter's hernias and non-Richter's type incarcerated hernias, Kadirov and colleagues2 noted that patients with Richter's hernias had greater preoperative delay, rate of bowel resection, length of hospital stay and postoperative morbidity and mortality rates. They concluded that early operative intervention is the mainstay of successful management and that awareness of the misleading clinical presentation of Richter's hernias is of utmost importance. Our own patient presented with bowel perforation and generalized peritonitis.
Whether the peritonitis and surgical intervention were factors in our patient's eventual miscarriage is unknown. Nevertheless, it is possible that early repair of the inguinal hernia recurrence might have prevented the complication.