Family physicians should always include pediatric vision screening in their routine care of children. Many vision-threatening conditions can be detected by using simple methods in the office, such as Snellen visual acuity testing, corneal light reflex examination and cover-uncover testing. Strabismus is the most common cause of amblyopia, and its detection will permit early intervention. The mainstays of therapy for amblyopia are forced use of the “weak” eye by patching the “good” eye, correction of any refractive error and subsequent surgery to align the visual axis. The earlier that amblyopia is detected, the better the visual recovery and the long-term prognosis.
Vision problems affect between 5 and 10 percent of young children.1 Up to 3 percent of the pediatric population younger than age six has strabismus, or misalignment of the visual axis.2 Of these children, as many as 40 percent subsequently develop amblyopia, or secondary vision loss related to disease of the visual pathways.3 Amblyopia is now the leading cause of monocular vision loss in people between the ages of 20 and 70.4 Fortunately, pediatric vision screening can reduce the incidence of vision loss related to amblyopia.5
While loss of vision is the most serious consequence of strabismus, children with this condition also suffer in other ways. While academic performance does not appear to be affected,6 children do experience psychologic difficulties, particularly in opposite-sex friendships during adolescence.7 Some professions require good binocular vision and therefore exclude persons with strabismus or amblyopia.8 These quality-of-life issues are important because some insurance companies treat strabismus surgery as a cosmetic procedure and refuse to authorize it.
Despite evidence that early detection and intervention can decrease the consequences of strabismus and other conditions that lead to amblyopia, studies find that primary care physicians are not consistently conducting pediatric vision screening during clinical visits.9,10 To provide effective preventive care for children, the family physician should be aware of pediatric vision screening practices, the pathophysiology of the various disorders leading to amblyopia and the management options. The American Academy of Pediatrics has published updated Pediatric Vision Screening Guidelines to promote early detection and treatment of vision-threatening conditions (Table 1).11
Physiology of the Visual Pathway
The ability to focus a visual image on the central retina develops at about two to three months of age. Ideally, all rays of light converge on the macula, the retinal area where images can be most sharply delineated. Accommodation is the process by which the ciliary body contracts, allowing the lens to assume a greater curvature and to increase refraction of light rays from near objects. Accommodation is reflexively linked to turning in of the eyes, or ocular convergence, so that a binocular image is maintained.
When moving in unison, each eye focuses the retinal image on its macula, and the cortical image in the occipital brain is reconciled into binocular “seeing.” If the retinal image is distorted in one eye because of a refractive difference between eyes (anisometropia) or a congenital cataract, or if the visual axis misaligns the image on the retina (strabismus), the cortical image is too dissimilar to permit clear binocular resolution. The brain quickly learns to suppress the poorer image from the affected eye to allow for clear vision. Since cortical visual development is dependent on continuous stimuli, neurodevelopment is impeded in the visual cortex corresponding to the suppressed eye. The result can be permanent visual impairment (amblyopia) in an otherwise normal eye (Table 2). This process is dynamic and reverses if the distortion of the retinal image is corrected; the earlier the correction, the more likely full development can be achieved.
Visual acuity improves with age. All children over age eight should be able to achieve 20/20 visual acuity using their best eyeglass correction. Younger children should be referred to an ophthalmologist if there is a difference between the right and left eyes of two or more lines on a Snellen chart evaluation.
Strabismus is the most common cause of amblyopia. Alignment of the visual axis occurs in the first three months of life. All infants should have consistent, synchronized eye movement by five to six months of age. Strabismus most often results from an altered reflex arc in the central nervous system. It can also result from cranial nerve palsies, neuromuscular disorders or craniofacial abnormalities. Amblyopia is not necessarily related to the degree of strabismus: even small deviations can result in significant vision loss.
Strabismus is categorized as medial deviation (esotropia), lateral deviation (exotropia) or vertical deviation (hypertropia). Vertical deviation is the least common type, and the higher eye is referenced as abnormal. Deviations that are always manifest are called tropias, while those that are only elicited by provocative testing are called phorias. In some cases, manifestation of the misalignment is inconsistent; this is termed intermittent strabismus.
Usually, the angle between the normal eye and the strabismic eye stays constant through all directions of gaze and is not influenced by the eye used for fixation. This is termed concomitant strabismus. When the eye divergence worsens in some gaze directions, the strabismus is non-concomitant. This is characteristic of restrictive or paralytic etiologies. In the majority of cases, strabismus develops between 18 months and six years of age.
Clinical Presentations
Esodeviations
Medial, or esodeviations, are the most common ocular deviations, accounting for more than one half of all cases of strabismus.
Infantile Strabismus. This disorder presents with profound esotropia before six months of age. It is the most frequent esodeviation in children and is often associated with a family history of strabismus. Affected children are otherwise normal, and their parents need to be reassured about this point because of the widespread misperception that developmental problems are associated with “crossed eyes.” The refraction of each eye is often normal, and the child may even alternate the fixating eye, which tends to reduce the risk of consequent amblyopia. Treatment includes the same measures used in other cases of strabismus, but surgical realignment tends to be carried out at an earlier age, usually before the child is two years old and sometimes as young as six months old.
Accommodative Esotropia. Normally, children are mildly farsighted, or hyperopic. This hyperopia can be overcome by accommodation if the refractive error is not severe. Accommodative esotropia occurs when a refractive hyperopia is in excess of what is normally present in children. Accommodation increases the refractive power of the lens, allowing for image focus on the retinal plane, but significant accommodation also results in a reflexive ocular convergence, forcing one eye medially off alignment. If one eye is habitually chosen for fixation, amblyopia will occur in the other eye. When the refractive error is extreme, even accommodation fails to produce a sharp retinal image, and both eyes may suffer some degree of amblyopia.
This condition is often hereditary, has an average onset at two to three years of age and may progress from intermittent or latent to constantly manifest deviation. Because the underlying process stems from refractive error, spectacle correction is the first treatment.
Nonaccommodative Esotropia. This type of esotropia may occur in children with normal visual acuity. It is most often associated with ocular insults such as trauma, prematurity, cataract or neurodevelopmental abnormalities.
Rare types of esodeviation include paralytic conditions affecting the sixth nerve and can be associated with Möbius syndrome (congenital oculofacial paralysis) or Duane syndrome (a hereditary condition resulting in limitation of eye movement). These esodeviations worsen depending on the direction of gaze (non-concomitant). Occasionally, a transient sixth nerve palsy may occur after a febrile illness. Nevertheless, acquired sixth nerve palsy in childhood may be an ominous sign indicating increased intracranial pressure.
Exodeviations
Lateral deviations account for about one quarter of ocular misalignments. They are often hereditary, and the majority are only manifest intermittently with fatigue, illness or distance fixation. Although these intermittent exotropias usually have a relatively favorable prognosis, they may decompensate to become constant exotropias and can lead to amblyopia. In this case, treatment is the same as for esodeviations.
Ocular or central nervous system pathology should be suspected if a child presents with a late-onset, constant exotropia. Third cranial nerve paresis, craniofacial abnormalities and surgical overcorrection of esotropia may also cause exotropia.
Vertical Deviations
Vertical strabismus accounts for less than 10 percent of ocular deviations and is often associated with a compensatory head tilt to minimize diplopia. Thus, all children who present with idiopathic torticollis should be evaluated for vertical strabismus. The majority of these deviations result from fourth cranial nerve paresis, which can occur traumatically or congenitally. A defect in the superior oblique muscle motility, called Brown syndrome, may also cause an inability to elevate the eye during medial gaze. Rare causes of vertical deviation include retro-orbital tumors, thyroid ophthalmopathy and muscle entrapment secondary to facial trauma.
Clinical Evaluation
The periodic well-child examination provides an ideal opportunity to screen for pediatric vision problems. Table 3 lists the recommended screening activities by age. Occasionally, a parent will raise concern about a child whose eyes misalign or whose head is habitually tilted. Such children seldom perceive visual trouble themselves, and the problem may elude detection unless vigilance is maintained. Any parental suspicion of a visual or alignment abnormality, or any family history of these disorders, should prompt evaluation by the family physician.
Visual Acuity
Visual screening begins with assessment of visual acuity. The testing method varies, depending on age. By five months of age, infants should regard faces or interesting objects with steady, conjugate gaze through all fields of vision. Toddlers with some speech skills can use Allen object recognition posters, which present a series of simple, idealized pictures. Recognition of each picture at 10 ft (3 m) is roughly equivalent to 20/30 vision. Children aged three and older can usually perform the “tumbling E” game, in which the child indicates the cross-bar direction of a series of progressively smaller “E's” presented with varying orientation. Figure 1 shows examples of pediatric screening charts.
FIGURE 1.
Pediatric vision screening charts commonly used for preliterate young children and for older children with mild mental retardation. (Left) Allen object recognition chart. (Right) “Tumbling E” chart.
For children in kindergarten or first grade, the Snellen letter or number charts represent the gold standard for in-office assessment of visual acuity. Children usually stand 10 ft (3 m) away from the visual chart to minimize the distraction that may occur in a busy office.
Visual acuity in each eye should be assessed by occluding the contralateral eye and measuring the uncovered eye with an age-appropriate technique. Younger children may not cooperate with the visual occlusion, but tolerance to occlusion of one eye and intolerance to occlusion of the other may suggest a significant difference in visual acuity between eyes.
Binocular Alignment
Once visual acuity is established, assessment of binocular alignment is the next step. In young infants, strabismus must be differentiated from the more common pseudostrabismus, in which the perception of medial deviation or esotropia is caused by prominent medial canthal folds and a flat nasal bridge. An infant with pseudostrabismus is shown in Figure 2.
FIGURE 2.
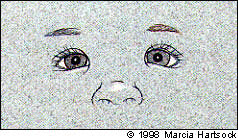
Pseudostrabismus resulting from a flat nasal bridge, wide epicanthal folds, and closely placed eyes. Note symmetric placement of the corneal light reflex (Hirschberg test).
The most common method of assessing ocular alignment is the Hirschberg corneal light reflex test. In this test, the examiner notes the position of the corneal reflection from a light held about 3 ft (1 m) from both eyes. The reflection should fall in the same location in the cornea of each eye, even when the eyes move. Displacement of the corneal light reflection in one eye suggests strabismus. Various findings encountered during corneal light reflection are illustrated in Figure 3: (A) Normal alignment—the light reflections are centered on both corneas. (B) Left esotropia—the light reflection is outwardly displaced on the left cornea. (C) Left exotropia—the light reflection is inwardly displaced on the left cornea. (D) Left hypertropia—the light reflection is downwardly displaced on the left cornea.
FIGURE 3.
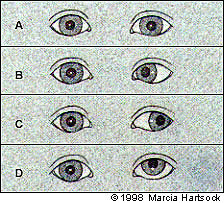
Findings during corneal light reflection. (A) Normal alignment: the light reflections are centered on both corneas. (B) Left esotropia: the light reflection is outwardly displaced on the left cornea. (C) Left exotropia: the light reflection is inwardly displaced on the left cornea. (D) Left hypertropia: the light reflection is downwardly displaced on the left cornea.
The second screening method for evaluating ocular alignment is a combination of the cover-uncover test and the alternating cover test. These examinations require more cooperation from the child but can disclose latent deviations that might otherwise be missed.
In the cover-uncover test, the child first focuses on an object about 10 ft (3 m) away, although this may be impractical in a small examining room. An interesting object such as a small toy usually holds the child's attention. The examiner covers one eye with a hand-held occluder or cupped hand, while watching the other eye for any movement of fixation. The examiner then removes the cover to see if the first eye has deviated.
If no movement is elicited on the cover-uncover test, the alternating cover test is performed. Again with the child focused on a distant object, each eye is covered in sequence, while the examiner looks for ocular deviation. If misalignment of either eye occurs during these provocative maneuvers, referral for treatment of strabismus is indicated. With practice, the entire ocular alignment screening examination can be accomplished in about 60 seconds.
Retinal Examination
The clinician should routinely perform retinoscopy, looking for intraocular pathology such as retinoblastoma. Pupillary dilation with a mild mydriatic agent like phenylephrine (Neo-Synephrine) 2.5 percent may aid in the retinal examination.
Abnormal Findings
Any abnormal findings on visual screening should prompt referral to an ophthalmologist. If the evaluation suggests strabismus, characterization of the deviation is helpful to the ophthalmologist. Monocular strabismus is suspected if one eye is consistently preferred for fixation. The strabismic eye is at high risk for amblyopia. If the eye preferred for fixation alternates during provocative testing, alternating strabismus is the likely diagnosis. Although this type of strabismus has a lower risk of amblyopia, it is still of significant concern. Figure 4 illustrates the findings encountered in monocular and intermittent esotropia during cover-uncover testing: (A) In esotropia, one eye is deviated inward. Note that the corneal light on that eye is not centrally placed. (B) When the esotropic eye is covered, neither eye moves. The uncovered eye remains fixated. (C) When the cover is removed, neither eye moves. (D) When the other eye is covered, the previously esotropic eye takes up fixation and the covered eye turns inward (becomes esotropic) under the cover. (E) If the cover is removed and no eye movement occurs, an absence of a strong preference is suggested. Both eyes have approximately equal vision. The diagnosis is alternating strabismus, associated with a lower risk of amblyopia. (F) If the cover is removed and both eyes move back to their original positions (the originally esotropic eye is again esotropic), one eye has a fixation preference. This indicates a monocular strabismus. The esotropic eye is at high risk for amblyopia. Note: The same maneuvers can be used to determine the presence of exotropia (outward deviation), hypertropia and hypotropia (upward and downward deviation, respectively) and cyclotropia (rotary displacement).
FIGURE 4.
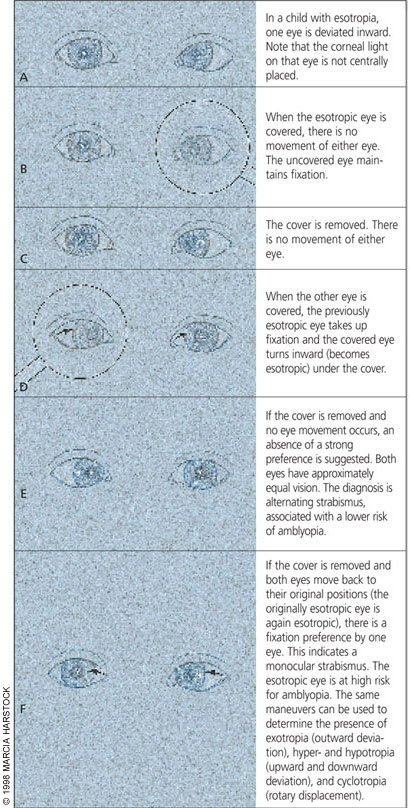
Monocular and intermittent strabismus as demonstrated by cover-uncover testing.
The alternating cover test elicits latent deviations (phorias) that may only be evident when one eye is quickly moved from fixation to occlusion. Phorias also have a lower risk for amblyopia but can progress to manifest tropias, which then require referral. Children will not outgrow strabismus. The common phorias detected by cover-uncover testing are illustrated in Figure 5: (A) Both eyes appear to be aligned and centrally fixating. Exophoria is detected by the following procedure: (B) One eye is covered. That eye will deviate outward. (C) When the cover is removed, the eye will return to a central position. In the figure, the patient has a left exophoria. The same procedure is then performed on the other eye. Esophoria is detected by the following procedure: (D) One eye is covered. That eye will deviate inward. (E) When the cover is removed, that eye will return to a central position. In the figure, the patient has a left esophoria. The same procedure is then performed on the other eye. Hyperphoria is detected by the following procedure: (F) One eye is covered. That eye will deviate upward. (G) When the cover is removed, the eye will return to a central position. In the figure, the patient has a left hyperphoria. The same procedure is then performed on the other eye.
FIGURE 5.
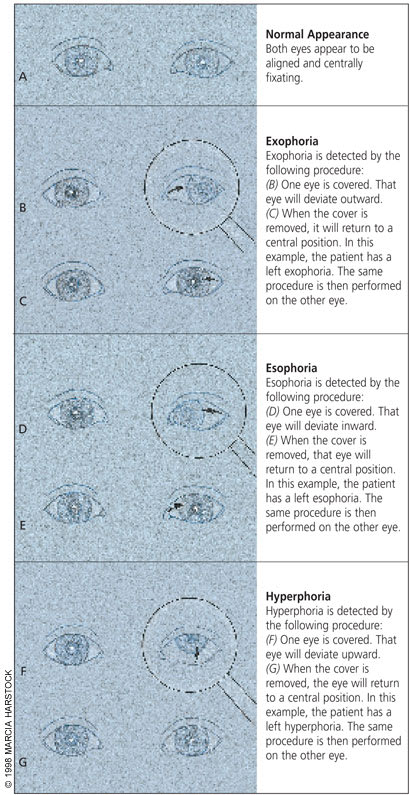
Detecting phorias by cover-uncover testing.
Management
The three principles of therapy for strabismus and resultant amblyopia are correction of the visual image clarity on the retina, alignment of bilateral vision and augmented development of the amblyopic visual cortex by intermittent occlusion of the preferred eye. The order in which these three principles are implemented depends in part on the clinical presentation, the degree of amblyopia and the age of the child. Certainly, any evident obstruction to a clear retinal image, such as congenital cataract or profound strabismus, requires treatment as soon as it is recognized. Refractive errors, however, are seldom diagnosed until early childhood or primary school age. Refractive correction is indicated as soon as an error is diagnosed. Figure 6 shows the result of correction in a child with accommodative esotropia related to hyperopia.
FIGURE 6.
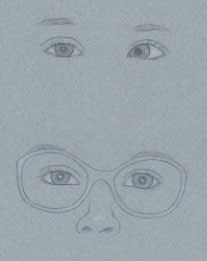
Optical correction of accommodative esotropia in a child with hyperopia. (Above) Without correction. (Below) With correction of hyperopia.
Treatment of amblyopia is the most time-critical aspect of therapy, and the assistance of a skilled ophthalmologist should be enlisted at an early stage. If strabismus is the cause of the amblyopia, surgical realignment of the visual axis is actually less urgent than treatment of amblyopia. Parents need to understand this because of popular expectations that surgery should be the first line of therapy for strabismus. In fact, in the absence of overt or potential amblyopia, surgical realignment may not be necessary.
Amblyopia is treated by forcing use of the suppressed eye with a patch over the preferred eye. If the child is intolerant of the patch, cycloplegic drops may be used to decrease the visual acuity of the preferred eye. A schedule whereby the patch is removed for one to two waking hours each day reduces the risk of a deprivation amblyopia in the good eye. Once the visual goal is achieved, part-time patching is needed to prevent relapse and is often continued for many months to years. The shorter the time that amblyopia is present and the later the age at which it began, the better the prognosis.
If surgical correction of strabismus is indicated, the main principle is altering the action of one or more extraocular muscles by repositioning them on the ocular globe. Sometimes it is necessary to operate on both eyes to balance the correction. The procedure is relatively short and the postoperative recovery is usually uneventful. The most frequent complication is that alignment has not been achieved and additional surgery is needed.
Final Comment
Pediatric vision screening is a critical part of the early well-child examination. The detection of vision-threatening ocular conditions early in the child's development provides a tremendous opportunity to prevent significant disability. The role of family physicians is pivotal because of the frequency of their contact with young children during periodic health evaluations. Using simple screening measures, family physicians can discover visual abnormalities at an age when ophthalmologic intervention has the greatest chance of success.
