Heel pain is a common condition in adults that may cause significant discomfort and disability. A variety of soft tissue, osseous, and systemic disorders can cause heel pain. Narrowing the differential diagnosis begins with a history and physical examination of the lower extremity to pinpoint the anatomic origin of the heel pain. The most common cause of heel pain in adults is plantar fasciitis. Patients with plantar fasciitis report increased heel pain with their first steps in the morning or when they stand up after prolonged sitting. Tenderness at the calcaneal tuberosity usually is apparent on examination and is increased with passive dorsiflexion of the toes. Tendonitis also may cause heel pain. Achilles tendonitis is associated with posterior heel pain. Bursae adjacent to the Achilles tendon insertion may become inflamed and cause pain. Calcaneal stress fractures are more likely to occur in athletes who participate in sports that require running and jumping. Patients with plantar heel pain accompanied by tingling, burning, or numbness may have tarsal tunnel syndrome. Heel pad atrophy may present with diffuse plantar heel pain, especially in patients who are older and obese. Less common causes of heel pain, which should be considered when symptoms are prolonged or unexplained, include osteomyelitis, bony abnormalities (such as calcaneal stress fracture), or tumor. Heel pain rarely is a presenting symptom in patients with systemic illnesses, but the latter may be a factor in persons with bilateral heel pain, pain in other joints, or known inflammatory arthritis conditions.
Strength of Recommendations
Heel pain in adults can be caused by various soft tissue, osseous, and systemic disorders. A thorough history and a physical examination of the lower extremity should be conducted to locate the pain, define its attributes, and narrow the differential diagnosis (Tables 11 and 2). Imaging studies may be indicated when there is suspicion of infection, stress fracture, or trauma.
TABLE 1 Cause of Heel Pain by Anatomic Location
| Pain in the midfoot |
| Lateral |
| Tendonitis of peroneus brevis |
| Tendonitis of peroneus longus |
| Medial |
| Tendonitis of the flexor digitorum longus |
| Tendonitis of the flexor hallucis longus |
| Tendonitis of the tibialis posterior |
| Pain in the posterior heel |
| Achilles tendonitis |
| Retroachilles bursitis |
| Retrocalcaneal bursitis |
| Pain in the plantar aspect of heel |
| Plantar fasciitis |
| Plantar fascia rupture |
| Heel pad atrophy |
| Tarsal tunnel syndrome |
| Neuroma |
| Bone cyst |
| Osteomyelitis |
| Fracture |
| Tumor |
Information from Brown C. A review of subcalcaneal heel pain and plantar fasciitis. Aust Fam Physician 1996;25:881.
TABLE 2 Common Causes of Heel Pain: History, Physical Examination Findings, and Treatment Options
| Clinical entity* | History | Physical examination | Conservative treatment |
|---|---|---|---|
| Plantar fasciitis | Morning pain or pain on standing after prolonged sitting | Tenderness over calcaneus Increased pain with passive dorsiflexion of toes | Analgesics, stretching, exercise, orthotics, night splint |
| Achilles tendonitis | Pain with running, jumping, or making quick turns | Pain and tenderness over insertion of Achilles tendon on calcaneus Pain may increase with dorsiflexion | Rest, analgesics, stretching, and strengthening exercises |
| Retrocalcaneal bursitis | Stiff posterior shoe edge | Pain and tenderness at posterior calcaneus | Analgesics, proper shoes with Achilles notch and padding over posterior heel |
| Tarsal tunnel syndrome | Pain or numbness in heel radiating to the sole and toes | Reproduction of symptoms with percussion of tarsal tunnel or dorsiflexion and eversion of foot | Analgesics, correcting foot posture with orthotics |
*—Listed in order of frequency of presentation.
The history should provide a description of the pain and related conditions and circumstances. The location and onset of heel pain, its variation in character and severity throughout the day, and the relieving and aggravating factors all provide important diagnostic clues. Increased levels of activity or exercise may indicate a musculoskeletal injury caused by overuse.2 If the patient describes the sensation as “burning,” “tingling,” or “numbness,” the cause may be peripheral nerve entrapment.3
Systemic disorders are uncommon causes of heel pain; however, a history of diabetes, rheumatologic disorders, or malignancy should prompt consideration of a systemic cause for heel pain, especially when there is no obvious local etiology.
The physical examination should include inspection of the patient’s foot at rest and in a weight-bearing position. A visual survey of the foot may reveal swelling, bony deformities, bruising, or skin breaks. The physician should palpate bony prominences and tendinous insertions near the heel and midfoot, noting any tenderness or palpable defects. Passive range of motion of the foot and ankle joints should be assessed for indications of restricted movement. Foot posture and arch formation should be visually examined while the patient is bearing weight; the physician is looking for abnormal pronation or other biomechanical irregularities. Observation of the foot while the patient is walking may allow the physician to identify gait abnormalities that provide further diagnostic clues. This article details specific maneuvers that may reproduce pain symptoms and help physicians identify particular causes of heel pain.
Plantar Fascia Lesions
The plantar fascia is a multilayered, fibrous aponeurosis with three portions—medial, central, and lateral. This fascia attaches to the three main weight-bearing points of the foot (i.e., calcaneus, first and fifth meta-tarsal heads) to form the longitudinal arch, which is integral to proper foot biomechanics during heel strike, foot plant, and push off. Conditions that increase tension on the plantar fascia and may cause pain include pes planus, pes cavus, decreased subtalar joint mobility, and a tight Achilles tendon.
Plantar fasciitis, the most common cause of heel pain in adults, typically results from repetitive use or excessive load on the fascia.4 Although the word “fasciitis” implies inflammation, recent research indicates that it is more likely to be a noninflammatory, degenerative process that might be more appropriately termed plantar fasciosis.5 The typical presentation is a gradual onset of plantar heel pain that is worse on taking the first steps in the morning or when standing up after prolonged sitting. Tenderness over the medial aspect of the calcaneal tuberosity usually is demonstrated, and the pain increases when the plantar fascia is stretched by passive dorsiflexion of the toes.
Acute onset of severe plantar heel pain after trauma or vigorous athletics may indicate rupture of the plantar fascia. Findings suggestive of rupture include a palpable defect at the calcaneal tuberosity accompanied by localized swelling and ecchymosis.6
If conservative treatment of plantar fasciitis fails to alleviate symptoms, radiographs are advisable to check for other causes of heel pain such as stress fractures, arthritis, or skeletal abnormalities. Radiographs may reveal a calcification of the proximal plantar fascia, which is known as a heel spur. However, these spurs often are present in asymptomatic persons, are nonspecific, and should not be construed as an explanation for heel pain.1
Tendinous Lesions
Patients who have tendonitis generally present with pain and swelling at the tendon insertion site. Passive dorsiflexion of the foot and palpation at the insertion site may increase the tenderness.2 The history may reveal difficulty in performing strenuous activities such as running, jumping, or making quick turns.2
The Achilles tendon is formed by the union of the gastrocnemius and soleus muscle tendons and inserts on the posterior aspect of the calcaneus. Achilles tendonitis is another common cause of posterior heel pain. Typically, it results from overuse of the calf muscles (e.g., running, jumping) or abnormal biomechanical stress on the foot and ankle.
The tendons of the posterior tibialis, the flexor digitorum longus, and the flexor hallucis longus pass through the medial flexor retinaculum and insert on the medial side of the midfoot (Figure 1). The peroneal tendons insert on the lateral side of the midfoot. Tendonitis involving these structures is a less common cause of heel pain but may be important when a patient localizes a medial or lateral location of heel pain.
Figure 1
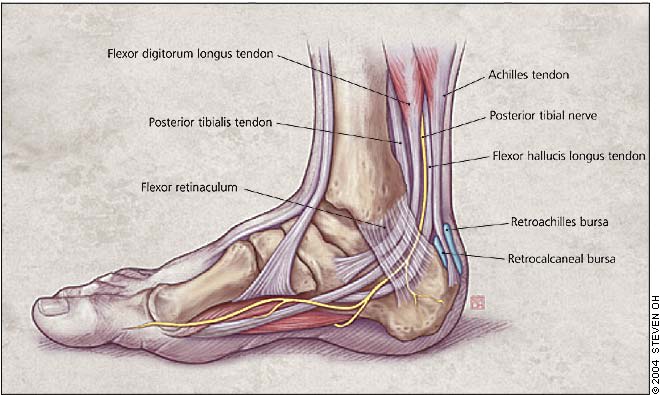
Medial view of the ankle illustrating the tendons, bursa, and nerves, which can be sources of heel pain.
Bursal Lesions
The posterior heel includes the retrocalcaneal bursa, which is located between the calcaneus and the Achilles tendon insertion site, and the retroachilles bursa, which is located between the Achilles tendon and the skin. Each bursa is a potential site of inflammation. The most common cause of posterior heel bursitis is ill-fitting footwear with a stiff posterior edge that abrades the area of the Achilles tendon insertion. Retrocalcaneal inflammation also may be associated with Achilles tendonitis and Haglund’s disease (a bony spur on the superior aspect of the posterior calcaneus)7 and, occasionally, may be caused by a systemic inflammatory arthritis such as rheumatoid arthritis. Patients with posterior heel bursitis have redness and swelling of the affected bursa, which is tender on direct palpation.
Osseous Lesions
After the metatarsals, the calcaneus is the most common location in the foot for a stress fracture.8 Calcaneal stress fractures are more likely to occur in athletes involved in sports that require running and jumping or in persons with osteopenia of the calcaneus. Patients present with diffuse heel pain and tenderness on medial and lateral compression of the calcaneus.
Refractory heel pain that persists despite conservative treatment may require further diagnostic procedures to exclude bony pathology. Radionuclide bone scans and magnetic resonance imaging (MRI) are more effective than plain-film radiographs in confirming a calcaneal stress fracture. Both methods detect stress fractures several weeks earlier than plain-film radiographs, and MRI permits visualization of abnormal soft tissue structures that may indicate other causes of heel pain.9,10
Calcaneal stress fractures are treated by cutting back on the quantity and intensity of walking and athletic activities. Non–weight-bearing status with crutches or cast immobilization may be necessary in some refractory cases.9
Simple bone cysts within the calcaneus generally are not associated with pain, although they may weaken the calcaneal structure. A pathologic fracture that extends to the wall of a bone cyst may induce heel pain.
Although rare, Ewing’s sarcoma is the most common primary bony tumor of the heel.11 Reported metastatic tumors to the calcaneus include endometrial adenocarcinoma, bronchogenic carcinoma, transitional cell bladder carcinoma, and gastric cancer.12–14 Patients who have heel pain of unclear etiology and a history of known malignancy should undergo radiographic evaluation or radionuclide bone scanning.
Peripheral Nerve Disorders
The tarsal tunnel, which is located on the medial aspect of the posterior heel, is bounded by the flexor retinaculum and the medial surfaces of the talus and calcaneus. The posterior tibial nerve courses through this tunnel and divides into its terminal branches, the medial and lateral plantar nerves (Figure 2). Heel pain accompanied by neuropathic features such as tingling, burning, or numbness may indicate tarsal tunnel syndrome, a compression neuropathy caused by entrapment of the posterior tibial nerve branches within the tunnel. Pain and numbness often radiate to the plantar heel and, in some cases, extend even to the distal sole and toes.
Figure 2
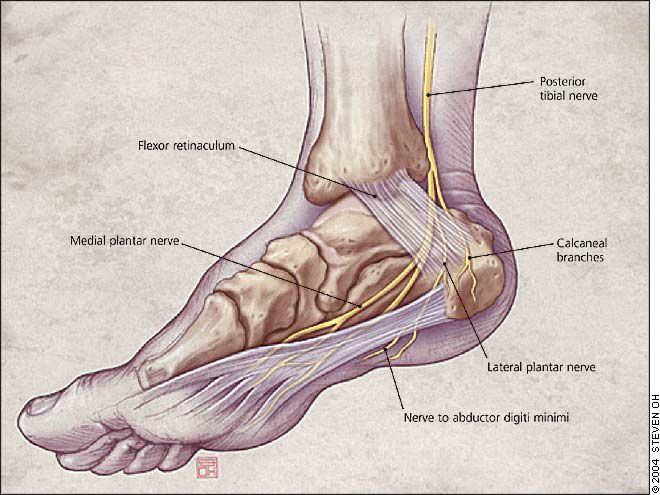
Medial view of the ankle illustrating the course of the posterior tibial nerve through the tarsal tunnel.
The clinical examination includes percussion of the nerve within the tarsal tunnel. Simultaneous dorsiflexion and eversion of the foot may reproduce symptoms as the posterior tibial nerve is stretched and compressed (Figure 3). Pes planus causes increased abduction of the forefoot and valgus deviation of the hindfoot (Figure 4), thereby increasing tension on the tibial nerve.2,15,16 Pes planus is a common cause of tarsal tunnel syndrome.
Figure 3
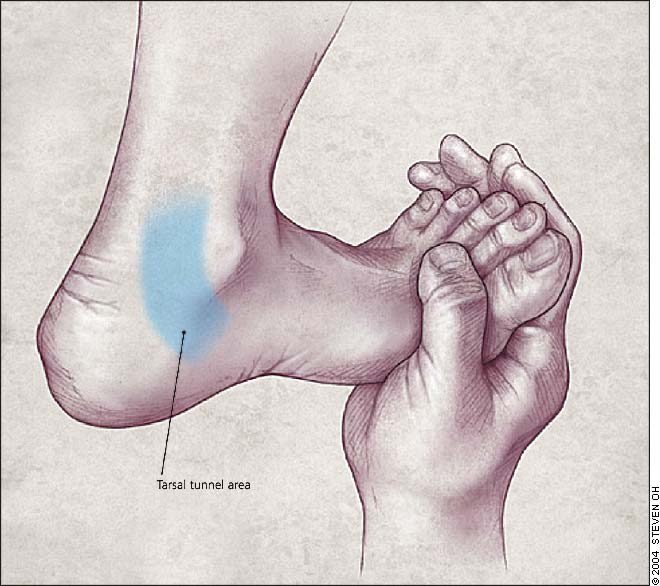
The dorsiflexion-eversion test used in the physical examination to reproduce the symptoms of tarsal tunnel syndrome.
Figure 4
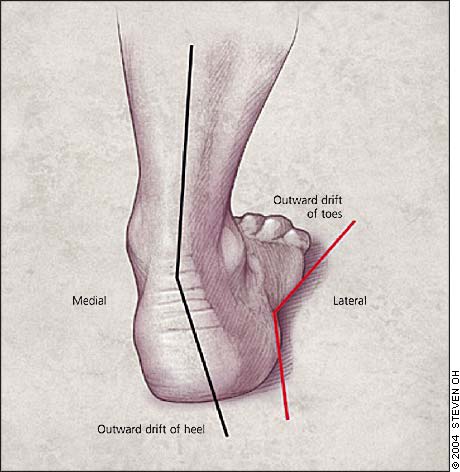
Posterior view of foot posture in patients with pes planus.
In some cases, nerve conduction velocities and electromyography may be used to confirm the diagnosis if treatment for presumptive neuropathic heel pain fails to improve symptoms.
Heel pain caused by a neuroma of the medial calcaneal nerve is uncommon and may present with symptoms quite similar to those of plantar fasciitis. Palpation of the sole over the heel and proximal midfoot may pinpoint a painful lump (known as the “lamp cord” sign because the lump feels like a lamp cord under a rug)17 that easily can be misdiagnosed as inflamed plantar fascia. If conservative treatment of plantar fasciitis fails to alleviate symptoms, the physician should evaluate for a neuroma.
Heel Pad Disorders
The heel pad is composed of columns of adipose tissue separated by fibrous septae. It is located directly beneath the calcaneus and acts as a hydraulic shock-absorbing layer. Elderly and obese patients who present with plantar heel pain may have symptoms caused by heel pad damage or atrophy. Inflammation of the heel pad also may be present in younger adults with sports-related injuries.
Although the symptoms of heel pad disorders overlap considerably with those of plantar fasciitis, heel pad pain is typically more diffuse. Heel pad pain involves most of the weight-bearing portion of the calcaneus, whereas plantar fasciitis pain is centered for the most part near the calcaneal tuberosity. In contrast to pain caused by plantar fasciitis, heel pad pain tends not to radiate anteriorly, and dorsiflexion of the toes does not increase the pain.
Infectious Etiologies
Although rarely a cause of heel pain, osteomyelitis of the calcaneus generally results from contiguous infection of surrounding soft tissue.18 During a visual examination of the foot, clues that should increase suspicion of a possible infectious cause for heel pain include puncture wounds, open skin lesions, localized warmth, erythema, or apparent cellulitis. Serious foot infections are more likely to occur in patients who have diabetes mellitus or vascular insufficiency. Radionuclide bone scanning and MRI are more sensitive and specific than plain-film radiographs in diagnosing osteomyelitis19–21 (Table 3).20,21
TABLE 3 Comparison of Imaging Modalities in Diagnosis of Osteomyelitis
Systemic Disease
Patients with known systemic arthritis conditions, bilateral heel pain, or symptoms involving joints beyond the heel should undergo a thorough review of symptoms to assess for systemic illness as a possible cause of heel pain. The seronegative spondyloarthropathies (i.e., ankylosing spondylitis, psoriatic arthritis, reactive arthritis, and inflammatory bowel disease–associated arthritis) may produce heel pain. Rheumatoid arthritis can affect the calcaneus and other adjacent structures; however, isolated heel pain as a presenting complaint would be uncommon, because hindfoot involvement typically occurs with advanced disease.22
