Temporomandibular joint disorders are common in adults; as many as one third of adults report having one or more symptoms, which include jaw or neck pain, headache, and clicking or grating within the joint. Most symptoms improve without treatment, but various noninvasive therapies may reduce pain for patients who have not experienced relief from self-care therapies. Physical therapy modalities (e.g., iontophoresis, phonophoresis), psychological therapies (e.g., cognitive behavior therapy), relaxation techniques, and complementary therapies (e.g., acupuncture, hypnosis) are all used for the treatment of temporomandibular joint disorders; however, no therapies have been shown to be uniformly superior for the treatment of pain or oral dysfunction. Noninvasive therapies should be attempted before pursuing invasive, permanent, or semipermanent treatments that have the potential to cause irreparable harm. Dental occlusion therapy (e.g., oral splinting) is a common treatment for temporomandibular joint disorders, but a recent systematic review found insufficient evidence for or against its use. Some patients with intractable temporomandibular joint disorders develop chronic pain syndrome and may benefit from treatment, including antidepressants or cognitive behavior therapy.
Temporomandibular joint (TMJ) disorder refers to a cluster of conditions characterized by pain in the TMJ or its surrounding tissues, functional limitations of the mandible, or clicking in the TMJ during motion.1,2 TMJ disorders are common and often self-limited in the adult population. In epidemiologic studies, up to 75 percent of adults show at least one sign of joint dysfunction on examination and as many as one third have at least one symptom.2,3 However, only 5 percent of adults with TMJ symptoms require treatment and even fewer develop chronic or debilitating symptoms.4
Etiology
The TMJ is a synovial joint that contains an articular disk, which allows for hinge and sliding movements. This complex combination of movements allows for painless and efficient chewing, swallowing, and speaking.5 The articulating surfaces of the TMJ are covered by a fibrous connective tissue; this avascular and noninnervated structure has a greater capacity to resist degenerative change and regenerate itself than the hyaline cartilage of other synovial joints.5 The synovial joint capsule and surrounding musculature are innervated, however, and are thought to be the primary source of pain in TMJ disorders.
The etiology of TMJ disorders remains unclear, but it is likely multifactorial. Capsule inflammation or damage and muscle pain or spasm may be caused by abnormal occlusion, parafunctional habits (e.g., bruxism [teeth grinding], teeth clenching, lip biting), stress, anxiety, or abnormalities of the intra-articular disk. In recent years, many of the theories about the development of TMJ disorders have been questioned. Abnormal dental occlusion appears to be equally common in persons with and without TMJ symptoms,1,6 and occlusal correction does not reliably improve the symptoms or signs of TMJ disorders.2,7 Parafunctional habits have been thought to cause TMJ microtrauma or masticatory muscle hyperactivity8; however, these habits are also common in asymptomatic patients. Although parafunctional habits may play a role in initiating or perpetuating symptoms in some patients, the cause-and-effect relationship remains uncertain.8
There is some evidence to suggest that anxiety, stress, and other emotional disturbances may exacerbate TMJ disorders, especially in patients who experience chronic pain.8 As many as 75 percent of patients with TMJ disorders have a significant psychological abnormality.8 Recognition and treatment of concomitant mental illness is important in the overall approach to management of chronic pain, including pain caused by TMJ disorders.
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendation | Evidence rating | References |
|---|---|---|
| TMJ disorders can be associated with other chronic pain syndromes or mental illness. Complicated cases may benefit from a multidisciplinary approach. | C | 8 |
| TMJ disorders are commonly self-limited and should initially be treated with noninvasive therapies. | C | 16 |
| Permanent occlusal adjustment and temporary dental splinting have not been sufficiently studied to indicate benefit or harm for patients with TMJ disorders. | B | 2, 7 |
TMJ = temporomandibular joint.
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, see page 1435 or https://www.aafp.org/afpsort.xml.
Diagnosis
CLINICAL EXAMINATION
Common symptoms of TMJ disorders include jaw pain, limited or painful jaw movement, headache, neck pain or stiffness, clicking or grating within the joint, and, occasionally, an inability to open the mouth painlessly.2,4 Most adults with these symptoms do not seek medical or dental treatment. It is not clear which symptoms are more common in which TMJ disorders; however, it is generally assumed that joint clicking or grating signifies intra-articular derangement whereas headache, neck pain, or painful jaw movement suggests a muscular problem.
Examination of the TMJ and masticatory muscles should include careful palpation of all structures. Myospasm and myofascial trigger points may be determined by palpation of the masseter or sternocleidomastoid muscles,9 which can be performed by placing a finger over the TMJ or into the ear canal while the patient opens and closes the mouth. A clicking or popping sensation that occurs during mouth opening may indicate displacement of the intra-articular disk during mandibular movement.10 Pain or swelling localized to the TMJ can indicate intra-articular inflammation. Clicking is a common symptom and is part of the diagnostic criteria for TMJ disorders; however, joint sounds do not necessarily correlate with pain severity or functional limitation. Therefore, the absence of clicking sounds is not a reliable symptom to use in determining whether the patient has responded to treatment.8 Absence of pain, improved function, and normal quality of life are more appropriate markers of treatment success.
DIFFERENTIAL DIAGNOSIS
The differential diagnosis for orofacial pain is listed in Table 1.4,11 TMJ disorders can cause referred pain, particularly undifferentiated headache.8 Some studies have shown that as many as 55 percent of patients with chronic headache who were referred to a neurologist were found to have significant signs or symptoms of TMJ disorders.12 Educating patients on self-care techniques and referral for noninvasive treatment should be considered in patients with chronic undifferentiated headache or headache that is not responding to standard treatment.
Table 1 Differential Diagnosis of Orofacial Pain
| Condition | Symptoms | Signs |
|---|---|---|
| Dental pathology | ||
| Tooth abscess | Pain with chewing over affected tooth | Visible tooth decay; fluctuance along gum line; pain with palpation over the tooth |
| Wisdom tooth eruption | Dull ache behind posterior molars | Tenderness to palpation over emerging tooth |
| Infection or inflammation | ||
| Herpes zoster and postherpetic neuralgia | Prodrome of pain followed by vesicular rash | Vesicular rash in dermatomal distribution, not crossing midline |
| Mastoiditis | Fever; otalgia | Postauricular erythema and swelling; tenderness over mastoid process |
| Otitis externa | Pruritus, pain, and tenderness of the external ear | Erythema and edema of external auditory canal |
| Otitis media | Fever; malaise; otalgia | Tympanic membrane dull, bulging, erythematous; loss of landmarks on tympanic membrane |
| Parotitis | Fever; malaise; myalgia; pain over parotid gland | Tenderness and induration over parotid gland |
| Sialadenitis | Pain and swelling of involved salivary gland | Tenderness, induration, and/or erythema of salivary gland; usually unilateral |
| Trigeminal neuralgia | Paroxysmal, unilateral lancinating pains in trigeminal nerve distribution | Examination generally normal |
CLASSIFICATION
Research has been hindered by the lack of clear diagnostic criteria for TMJ disorders; however, two groups have developed diagnostic classification systems. The American Academy of Orofacial Pain published a diagnostic classification system in 1995.8 Also, the Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD) tool was created and validated by the International Consortium for RDC/TMD-based Research.13 These two classification systems are not identical, but are substantially similar.14 The length and in-depth nature of the RDC/TMD make this instrument impractical for daily use in the family physician's office; therefore, it will not be discussed in this article.
An abbreviated version of the diagnostic classification system developed by the American Academy of Orofacial Pain is shown in Table 2.8 TMJ disorders are separated into two main categories based on the anatomic origin of the problem: articular disorders and masticatory muscle disorders. Articular disorders include the articular surface, intra-articular disk, or articulating bones.8,11 Masticatory muscle disorders are problems within the muscles surrounding the TMJ. Accurate recognition of the origin of pain, either intra-articular or muscular, may help the physician recommend an initial therapy; however, it is not clear which noninvasive therapies work best.8
Table 2 Diagnostic Classification of TMJ Disorders
| Articular disorders of the TMJ | |
| Ankylosis | |
| Congenital or developmental disorders | |
| Aplasia, hyperplasia, or hypoplasia of the cranial bones or mandible | |
| Neoplasia of the TMJ or associated structures | |
| Disk derangement disorders | |
| Articular disk displacement with or without reduction | |
| Fracture of the condylar process | |
| Inflammatory disorders | |
| Synovitis, capsulitis, polyarthritides including the TMJ | |
| Osteoarthritis | |
| TMJ dislocation | |
| Masticatory muscle disorders | |
| Local myalgia (unclassified) | |
| Myofascial pain | |
| Myofibrotic contracture | |
| Myositis | |
| Myospasm | |
| Neoplasia | |
TMJ = temporomandibular joint.
Information from reference 8.
DIAGNOSTIC TESTING
Diagnostic testing and radiologic imaging of the TMJ have uncertain usefulness and generally should only be used for the most severe or chronic symptoms.8 Local anesthetic nerve blocking can be helpful in differentiating whether orofacial pain originates from the TMJ capsule or from associated muscular structures. Sensory innervation of the TMJ is delivered primarily through the auriculotemporal branch of the third division of the trigeminal nerve (Figure 1).5,15 Patients who do not experience pain relief from diagnostic nerve blocking should be evaluated for other causes of orofacial pain.5
Figure 1.
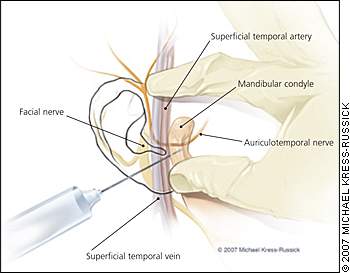
Anatomy of the temporomandibular joint and associated structures. For a diagnostic anesthesia block, use a small needle (25 to 30 gauge) to inject 0.5 cc of a short-acting anesthetic approximately 0.50 to 0.75 inches below the skin just inferior and lateral to the mandibular condyle.15 Always aspirate before injecting to ensure the needle is not in an artery or vein.
Treatment
For most patients, the signs and symptoms of TMJ disorders improve over time with or without treatment. As many as 50 percent of patients improve in one year and 85 percent improve completely in three years.16 Interventions that change the anatomy of the joint, invade the integrity of the joint space, or manipulate the jaw have the potential to cause harm and have not been shown to improve symptoms. Therefore, self-care and noninvasive treatments are good options and should be attempted before invasive or permanent therapies, such as orthodontics or surgery, are recommended.16
SELF-CARE
There is little evidence to suggest that any TMJ disorder treatment modality is superior to any other, although it is generally accepted that self-care and behavioral interventions should be encouraged for all patients, regardless of which therapies are considered.8 Providing a few simple exercises, behavioral instructions, and reassurance are important steps when treating the average patient with new or intermittent symptoms.
NONINVASIVE THERAPY
Many noninvasive therapies are commonly used for the treatment of TMJ disorders. The disciplines of medicine, dentistry, physical therapy, and psychology can all provide effective treatment. Several available therapies are listed in Table 3.8,17 Because most patients with TMJ disorders improve with or without treatment, these conservative therapies should be encouraged before invasive treatments are considered.
Table 3 Noninvasive Therapies for TMJ Disorders
| Alternative therapies | |
| Acupressure | |
| Acupuncture | |
| Hypnosis | |
| Massage | |
| Dental procedures | |
| Temporary occlusal therapy | |
| Medical interventions | |
| Intra-articular corticosteroid or anesthetic injection | |
| Myofascial trigger-point injection | |
| Pharmacologic treatment | |
| Acetaminophen | |
| Anxiolytics | |
| Benzodiazepines | |
| Muscle relaxants | |
| Nonsteroidal anti-inflammatory drugs | |
| Tricyclic antidepressants | |
| Physical therapy modalities | |
| Biofeedback | |
| Iontophoresis | |
| Phonophoresis | |
| Superficial or deep heat | |
| Therapeutic exercise | |
| Lateral jaw movement | |
| Protrusive jaw movement | |
| Resisted closing | |
| Resisted opening | |
| Tongue-up exercise | |
| Transcutaneous electrical nerve stimulation | |
| Psychological interventions | |
| Cognitive behavior therapy | |
| Relaxation techniques | |
| Stress management | |
TMJ = temporomandibular joint.
PHARMACOLOGIC INTERVENTION
Pharmacologic interventions similar to those for other musculoskeletal disorders are a treatment option. Acetaminophen and non-steroidal anti-inflammatory drugs can help with acute and chronic pain. For muscle spasm and chronic bruxism, muscle relaxants or benzodiazepines may be necessary if conservative relaxation techniques fail. Tricyclic anti-depressants may help with pain, including pain from nighttime bruxism.4,8,16 Antidepressants that are used in the treatment of chronic pain syndromes might also be beneficial in the treatment of chronic TMJ disorders. However, care should be used when prescribing selective serotonin reuptake inhibitors because there have been rare case reports of selective serotonin reuptake inhibitor-induced bruxism.18
INTRA-ARTICULAR INJECTIONS
Intra-articular injections of the TMJ with local anesthetics or corticosteroids can be used for the treatment of inflammation within the TMJ capsule.8 Intra-articular injection should only be used for severe acute exacerbations or after conservative therapies have been unsuccessful.8 Repeated intra-articular corticosteroid injections are not recommended. A recent systematic review found insufficient evidence to encourage the use of intra-articular hyaluronate for the treatment of TMJ pathology.19 Local anesthetics and botulinum toxin (Botox) can also be used in myofascial trigger-point injections for the treatment of chronic bruxism.8,16,20
DENTAL OCCLUSION THERAPY
Dental occlusal splinting and permanent occlusal adjustment have been the mainstays of TMJ disorder treatment for years, although there is no clear evidence that malocclusion of the upper and lower teeth causes TMJ pain.8 Two main types of splinting are available: occluding and nonoccluding. Occluding splints, also called stabilization splints, are specially fabricated to improve the alignment of the upper and lower teeth.20–22 Nonoccluding splints, also called simple splints, primarily open the jaw, release muscle tension, and prevent teeth clenching.20–22 Occluding splints need to be fabricated and adjusted by a trained dentist and may cost several hundred dollars in overall treatment costs.12 Nonoccluding splints are typically made of a soft vinyl and are easier and cheaper to fabricate. Inexpensive versions can usually be purchased at local pharmacies.22 Permanent occlusal adjustment can be obtained through orthodontics or by grinding down the superficial tooth enamel to improve occlusion.8
The Cochrane Collaboration recently reviewed permanent occlusal adjustment and occluding splint therapy for treatment of TMJ disorders.2,7 There was insufficient evidence to show benefit or harm with either treatment.2,7 Also, several trials comparing occluding and nonoccluding splint therapy have shown no significant differences in long-term treatment outcomes.23 Occlusal adjustment, either permanent or temporary, can still be an appropriate treatment for dental pathology, but its role in the primary treatment of TMJ disorders is uncertain.8
MANUAL REDUCTION IN ACUTE DISK DISPLACEMENT
Acute anterior displacement of the intra-articular disk is a rare condition that causes the jaw to lock in the open position. This can lead to painful inflammation in the articular capsule and can inhibit swallowing and eating. Most patients with acute locking of the jaw have a history of episodic locking, a noticeable click with chewing, or a habit of teeth clenching.10 Disk displacement should be reduced as soon as possible.
If the patient is unable to reduce the displacement by laterally moving the mandible and opening the mouth wide, manual reduction should be attempted. Manual reduction of the disk can usually be achieved by inserting the thumb into the patient's mouth, grasping under the chin, and simultaneously pushing down on the posterior teeth and pulling up on the chin. The mandibular condyle will be distracted downward, allowing the disk to move posteriorly into place.10 The patient's head should be stabilized, either by the examiner's opposite hand or a headrest or wall. A local anesthetic or intravenous benzodiazepine may be used to decrease pain and relax severe spasm before manual reduction. If the reduction is not successful, the patient should be evaluated by an oral surgeon as soon as possible.
