Slipped capital femoral epiphysis is the most common hip disorder in adolescents, and it has a prevalence of 10.8 cases per 100,000 children. It usually occurs in children eight to 15 years of age, and it is one of the most commonly missed diagnoses in children. Slipped capital femoral epiphysis is classified as stable or unstable based on the stability of the physis. The condition is associated with obesity and growth surges, and it is occasionally associated with endocrine disorders such as hypothyroidism, growth hormone supplementation, hypogonadism, and panhypopituitarism. Patients usually present with limping and poorly localized pain in the hip, groin, thigh, or knee. Diagnosis is confirmed by bilateral hip radiography, which needs to include anteroposterior and frog-leg lateral views in patients with stable slipped capital femoral epiphysis, and anteroposterior and cross-table lateral views in patients with the unstable form. The goals of treatment are to prevent slip progression and avoid complications such as avascular necrosis and chondrolysis. Stable slipped capital femoral epiphysis is usually treated using in situ screw fixation. Treatment of unstable slipped capital femoral epiphysis usually involves in situ fixation, but there is controversy about the timing of surgery, value of reduction, and whether traction should be used.
Slipped capital femoral epiphysis (SCFE) is the most common hip disorder in adolescents, usually occurring between eight and 15 years of age.1,2 The condition is defined as the posterior and inferior slippage of the proximal femoral epiphysis on the metaphysis (femoral neck), which occurs through the epiphyseal plate (growth plate).1,2 Figure 1 illustrates developing hip anatomy. Because of various factors, physicians often miss its diagnosis when patients initially present with vague symptoms.3,4 The prognosis of SCFE is related to how quickly the condition is diagnosed and treated.3,5 Delays in diagnosis can lead to disabling conditions and early-onset degenerative hip arthritis that eventually require hip reconstruction.6,7 SCFE should be considered in children who present with limping and pain in the hip, groin, thigh, or knee1,3,6–8; these patients should be evaluated with appropriate radiography.
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendation | Evidence rating | References |
|---|---|---|
| Family physicians should consider SCFE when a child presents with limping and groin, hip, thigh, or knee pain. | C | 1, 3, 6–8 |
| Physical examination of patients with SCFE usually shows decreased internal rotation of the hip and obligatory external rotation. | C | 1, 4, 8 |
| Radiography to rule out SCFE should include anteroposterior and lateral views of the hips (frog-leg lateral views for stable SCFE; cross-table lateral views for unstable SCFE). | C | 1, 9 |
| The standard treatment of stable SCFE is in situ fixation with a single screw. | C | 1, 4, 9, 31 |
SCFE = slipped capital femoral epiphysis.
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.xml.
Figure 1.
Anatomy of the developing hip.
Classification
Classification of SCFE is based on the stability of the physis.9 If the patient is able to ambulate with or without crutches, the SCFE is considered stable.10 If the patient is unable to ambulate even with crutches, the SCFE is considered unstable.9 Stable SCFE accounts for about 90 percent of all slips.11 Classification is important because a stable SCFE generally has a better prognosis than an unstable SCFE, which has a higher rate of complications.12
Epidemiology
The prevalence of SCFE is 10.8 cases per 100,000 children.2,12 It is more common in boys than girls, as well as in blacks and Pacific Islanders, possibly because of increased body weight in these populations.12 The average age at diagnosis is 13.5 years for boys and 12.0 years for girls.12 SCFE presents bilaterally in 18 to 50 percent of patients.13–15 Some patients present sequentially (hips usually affected within 18 months of each other).10 There is a seasonal variation in the rate of SCFE in the northern United States, with increased rates in late summer and fall in patients who reside north of 40 degrees latitude.16,17 This may be caused by increased physical activity in the summer or may result from impaired vitamin D synthesis.
Etiology
The etiology of SCFE is thought to be multifactorial and may include obesity, growth surges, and, less commonly, endocrine disorders.18–21 Of children diagnosed with SCFE, 63 percent have a weight in the 90th percentile or higher.22,23 Related endocrine disorders include hypothyroidism, growth hormone supplementation, hypogonadism, and panhypopituitarism.2 An endocrine disorder should be considered in SCFE with unusual presentations, including patients who are younger than eight years, older than 15 years, or underweight.20
History and Physical Examination
Table 1 outlines the differential diagnosis of a young patient presenting with hip pain. The most common symptoms of SCFE are limping and pain that is poorly localized to the hip, groin, thigh, or knee.8 Knee or distal thigh pain is the presenting symptom in 15 percent of patients with the condition.24 History of trauma to the area is rare.9,25
Table 1. Differential Diagnosis of Hip Pain in the Young Patient
| Condition | Age (years) | Clinical features | Frequency | Diagnosis |
|---|---|---|---|---|
| Apophyseal avulsion fracture | 12 to 25 | Pain after sudden forceful movement | Often | History of trauma; radiography |
| Hip apophysitis | 12 to 25 | Activity-related hip pain | Often | History of overuse; radiography to rule out fractures |
| Transient synovitis | < 10 | Limping or hip pain | Often | Radiography; laboratory testing; ultrasonography |
| Fracture | All ages | Pain after traumatic event | Occasionally | History of trauma; radiography |
| Slipped capital femoral epiphysis | 10 to 15 | Hip, groin, thigh, or knee pain; limping | Occasionally | Bilateral hip radiography (anteroposterior and lateral) |
| Legg-Calvé-Perthes disease | 4 to 9 | Vague hip pain, decreased internal rotation of hip | Infrequently | Hip radiography or magnetic resonance imaging |
| Septic arthritis | All ages | Fever, limping, hip pain | Infrequently | Radiography; laboratory testing; joint aspiration |
note: Table is sorted by frequency of conditions.
On physical examination, the patient may be unable to bear weight with a severe slip. Limited internal rotation of the hip is the most telling sign in the diagnosis of SCFE.8 Obligatory external rotation is noted in the involved hip of patients with SCFE when the hip is passively flexed to 90 degrees1,4,8 (Figure 2). Unless the patient has bilateral SCFE, it is helpful to compare range of motion with the uninvolved hip.
Figure 2.

Obligatory external rotation of the hip.
Radiography
Radiography is needed for patients eight to 15 years of age with new-onset limping and pain in the hip, groin, thigh, or knee. It is important to inform the radiologist of the clinical context and that SCFE is suspected so that the diagnosis can be ruled out. Radiography needs to include anteroposterior and frog-leg lateral views of both hips to diagnose stable SCFE (Figure 3). In unstable SCFE, anteroposterior and cross-table lateral views of the involved side should be compared with the uninvolved side because of the decreased range of motion of the hip.1,9 The radiologic signs of SCFE are shown in Figures 426 and 5.
Figure 3.

Frog-leg lateral radiography of mild stable slipped capital femoral epiphysis.
Figure 4.
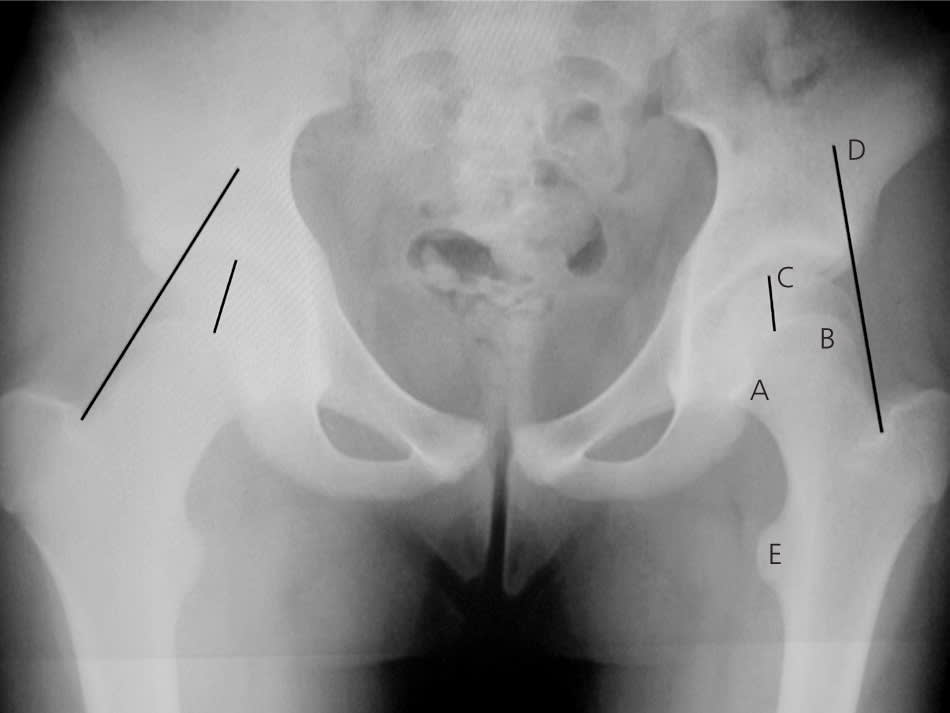
Anteroposterior radiography of left-sided slipped capital femoral epiphysis. Radiologic signs include: (A) Steel sign: on anteroposterior radiography, a double density is found at the metaphysis (caused by the posterior lip of the epiphysis being superimposed on the metaphysis); (B) widening of the growth plate (physis) compared with the uninvolved side; (C) decreased epiphyseal height compared with the uninvolved side; (D) Klein’s line: on anteroposterior radiography, a line drawn along the superior edge of the femoral neck should normally cross the epiphysis; the epiphysis will fall below this line in slipped capital femoral epiphysis; and (E) lesser trochanter prominence, which is caused by external rotation of the femur.
Information from reference 26.
Figure 5.
Diagrams of radiographic signs of slipped capital femoral epiphysis.
Radiography is used to grade the severity of the slip in SCFE. The Wilson method measures the relative displacement of the epiphysis on the metaphysis in a frog-leg lateral radiograph. A mild slip involves epiphysis displacement less than one third of the width of the metaphysis; a moderate slip involves displacement between one third and one half of the width; and a severe slip involves displacement greater than one half of the width.9 The Southwick method measures the epiphyseal shaft angle on the frog-leg lateral radiograph27 (Figure 6). The angle is calculated by subtracting the epiphyseal shaft angle on the uninvolved side from that on the side with SCFE. A mild slip is less than 30 degrees, a moderate slip is between 30 and 50 degrees, and a severe slip is greater than 50 degrees.28
Figure 6.
Southwick method for determining slipped capital femoral epiphysis (SCFE) severity using a frog-leg lateral radiograph. The first line (a) is drawn from the anterior to the posterior epiphyseal edges. Next, a line (b) is drawn perpendicular to the first line. A third line (c) is drawn down the middle of the femoral diaphysis. The angle formed by lines b and c is the lateral epiphyseal-shaft angle (LESA). The actual slip angle is the difference between the LESA of the SCFE hip and that of the uninvolved hip.
Treatment
Once the diagnosis of SCFE is made, the patient should be placed on non–weight-bearing crutches or in a wheelchair and quickly referred to an orthopedic surgeon familiar with the treatment of SCFE.1 The initial goals of treatment are to prevent slip progression and avoid complications.9,29
Prophylactic treatment of the contralateral hip in patients with SCFE is controversial, but it is not recommended in most patients. Prophylactic pinning may be indicated in patients at high risk of subsequent slips, such as patients with obesity or an endocrine disorder, or those who have a low likelihood of follow-up.11,15,30
STABLE SCFE
The standard treatment of stable SCFE is in situ fixation with a single screw1,4,9,31 (Figure 7). Case series and animal model studies have shown this to be a simple technique with low rates of recurrence and complications.4,9,31 After closure of the growth plate, progression of athletic activities may be allowed, including running and, eventually, participating in contact sports.1 Most patients with mild to moderate SCFE who are treated with in situ fixation have good to excellent long-term outcomes.11
Figure 7.

Anteroposterior radiography of bilateral stable slipped capital femoral epiphysis treated with in situ fixation with a single screw.
UNSTABLE SCFE
Unstable SCFE is a much more severe injury than stable SCFE. The rate of osteonecrosis is as high as 20 to 50 percent in patients with the unstable form.9,32 Treatment goals are similar to those of stable SCFE with in situ fixation, but there is controversy as to the specifics of treatment, including timing of surgery, value of reduction, and whether traction should be used.1,31
Complications
AVASCULAR NECROSIS
Avascular necrosis occurs in up to 60 percent of patients with unstable SCFE.31 It is a serious complication associated with severe displacement and fixation with more than one screw.8,29 Avascular necrosis often leads to advanced and early degenerative osteoarthritis.33
CHONDROLYSIS
Chondrolysis is the acute loss of articular cartilage, which causes joint stiffness and pain.9 It is usually reported as a complication of surgical treatment of SCFE, but it can occur with the use of a hip spica cast and in untreated advanced SCFE. With the improvement of surgical techniques, the incidence of chondrolysis has decreased from a rate of 5 to 7 percent to a rate of 1 to 2 percent in patients treated for SCFE.8,29
