A 27-year-old man presented with constant right-sided neck, throat, and ear pain that began one day earlier after he completed an uneventful five-mile trail run. There were no alleviating or exacerbating factors for the pain. He did not have trauma or injury to the area. He reported a vague sensation of fluid moving around in his neck and a strange feeling in his throat with swallowing. He did not have dysphagia, odynophagia, fever, chills, or respiratory symptoms. He did not use drugs or alcohol.
On physical examination, he was well appearing with normal vital signs and normal oxygen saturation on room air. An ear examination was normal. The neck examination revealed minimally palpable crepitus at the right lateral aspect of the base of the neck. There was no skin warmth or erythema. Soft tissue neck radiography was performed (Figure 1 and Figure 2).
Figure 1

Figure 2

Question
Based on the patient's history, physical examination, and radiography findings, which one of the following is the most likely diagnosis?
A. Esophageal rupture.
B. Retropharyngeal abscess.
C. Spontaneous gas gangrene.
D. Spontaneous pneumomediastinum.
E. Spontaneous pneumothorax.
Figure 3.
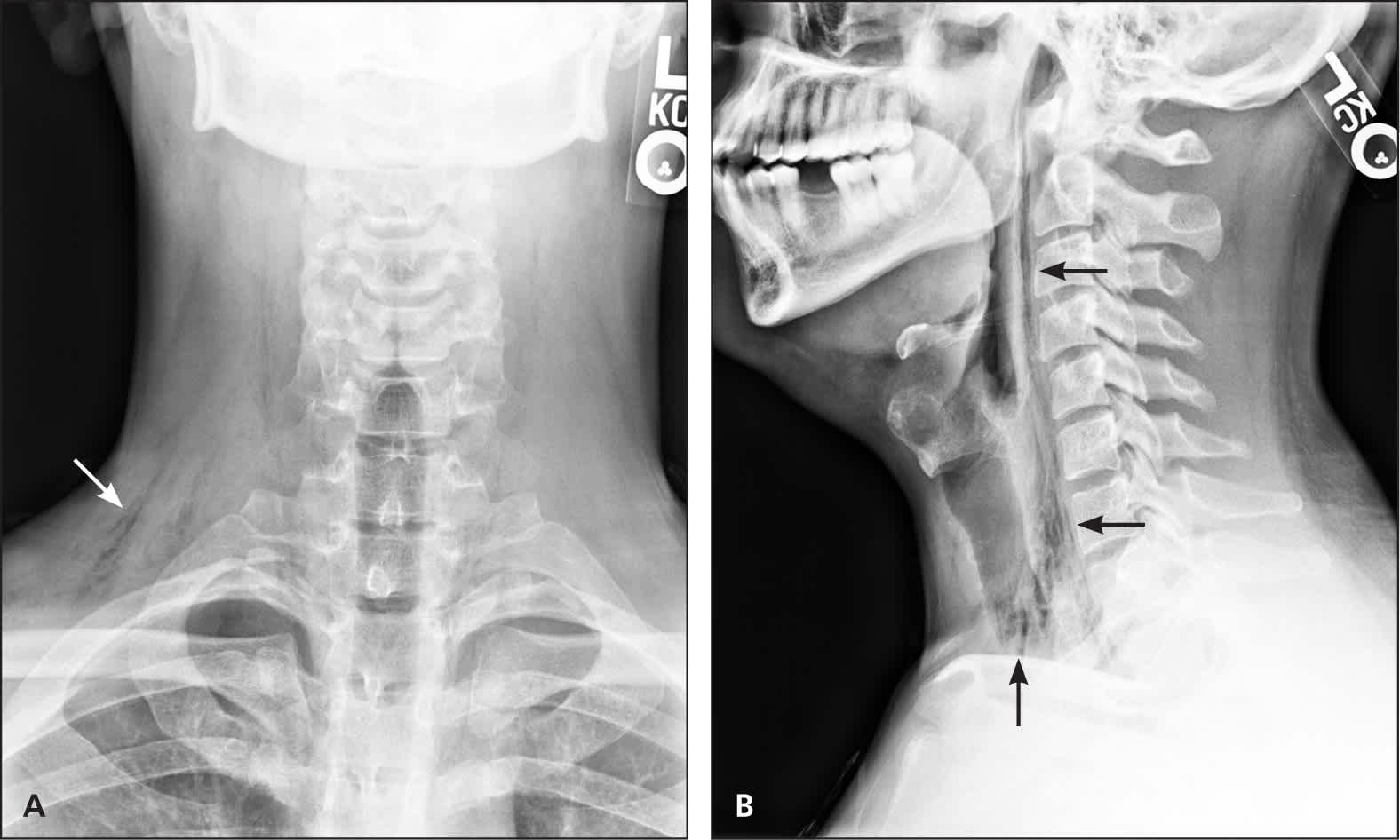
Free air or gas (arrows) in the deep tissue planes of the neck and upper thorax tracking superiorly from the mediastinal space. (A) Anteroposterior view. (B) Lateral view.
Discussion
The answer is D: spontaneous pneumomediastinum. Spontaneous pneumomediastinum is the sudden presence of free air or gas in the mediastinal space in a previously healthy patient. The deep tissue planes in the neck and upper thorax form a potential space for free air to track from the mediastinum to the cervical region (Figure 3), causing subcutaneous emphysema, as in this patient. Pneumomediastinum is rare and is often the result of thoracic trauma, surgical procedures, or pulmonary infections.1 Spontaneous pneumomediastinum is more common in children than adults. In adults, it predominantly occurs in healthy, thin young men. The underlying cause is alveolar rupture due to overdistention or increased alveolar pressure.2 There are case reports of spontaneous pneumomediastinum resulting from exertion in childbirth and during sports.3
Symptoms include the sudden onset of neck swelling, neck pain, odynophagia, chest pain, dyspnea, cough, and, less commonly, voice changes. On physical examination, subcutaneous crepitus in the neck may be noted. The diagnosis can usually be made with plain radiography of chest or neck soft tissue. Radiographs reveal subcutaneous emphysema or air in the tissue planes of the neck. Less commonly, axial computed tomography of the chest is needed to make the diagnosis. No treatment beyond rest and analgesics is recommended. Clinical findings typically resolve within seven days.
Esophageal rupture is a spontaneous tear of the esophageal wall due to increased pressure in the esophagus. Most cases are iatrogenic, usually from medical instrumentation such as endoscopy, but it can also occur with vomiting. Symptoms are severe retrosternal chest pain, dysphagia, and upper abdominal pain that is typically preceded by vomiting. Esophageal rupture can cause mediastinitis and pneumomediastinum. Gas in the neck may be seen. Diagnosis is made with a contrast esophagram or computed tomography.4
Retropharyngeal abscess is caused by a bacterial infection in the soft tissue posterior to the pharynx. It is more common in children. Symptoms include dysphagia, odynophagia, drooling, decreased oral intake, neck swelling, refusal to move the neck, muffled “hot potato” voice, and fever. Typically, children with the condition are ill appearing. Radiography of the lateral neck may reveal widening of the prevertebral space, loss of cervical lordosis because of muscle spasm, a soft tissue mass in the posterior pharynx, or rarely, air fluid levels or gas in the prevertebral space only.5
Spontaneous gas gangrene, or clostridial myonecrosis, is a life-threatening muscle infection that develops after hematogenous seeding by Clostridium septicum from the gastrointestinal tract. It can occur anywhere in the skeletal muscles of the body. Symptoms include sudden onset of severe muscle pain and fever. Predisposing factors may include gastrointestinal lesions, such as carcinoma, and immunosuppression. Physical findings include tissue crepitus with tenderness, edema, bullae, and purple skin discoloration. Sepsis is common. Gas within the soft tissue on radiography or computed tomography is suggestive of gas gangrene and helps to differentiate it from other bacterial soft tissue infections.6
Spontaneous pneumothorax is the presence of gas or free air in the pleural space of the thoracic cavity. Symptoms are sudden onset of chest pain and shortness of breath. Physical findings can be subtle and include hyperresonance and decreased breath sounds on the affected side. Chest radiographs (posteroanterior inspiratory and lateral films) may show displacement of the pleural line (the line between the lung and chest wall), but soft tissue radiographs are normal.7
Summary Table
| Condition | Characteristics |
|---|---|
| Esophageal rupture | Severe retrosternal chest pain, dysphagia, and upper abdominal pain that is typically preceded by vomiting; gas in the neck may be seen if complicated by mediastinitis or pneumomediastinum |
| Retropharyngeal abscess | Dysphagia, odynophagia, drooling, decreased oral intake, neck swelling, refusal to move the neck, muffled “hot potato” voice, and fever; more common in children; radiography of the lateral neck may reveal widening of the prevertebral space, loss of cervical lordosis, a soft tissue mass in the posterior pharynx, or, rarely, air fluid levels or gas in the prevertebral space only |
| Spontaneous gas gangrene | Sudden onset of severe muscle pain and fever; tissue crepitus and tenderness, edema, bullae, and purple skin discoloration; often accompanied by systemic symptoms of sepsis; gas within the soft tissue on radiography or computed tomography |
| Spontaneous pneumomediastinum | Sudden onset of neck swelling, neck pain, odynophagia, chest pain, dyspnea, cough, and, less commonly, voice changes; subcutaneous crepitus in the neck may be noted; radiographs reveal subcutaneous emphysema and air in the tissue planes of the neck |
| Spontaneous pneumothorax | Sudden onset of chest pain and shortness of breath; hyperresonance and decreased breath sounds on the affected side; chest radiographs show displacement of the pleural line |
