Original Article: Epistaxis: Outpatient Management
Issue Date: August 15, 2018
See additional reader comments at: https://www.aafp.org/afp/2018/0815/p240.html
To the Editor: The authors nicely described the traditional method for anterior-posterior nasal packing in patients with epistaxis. An alternative technique may improve posterior nosebleed management. The placement of expandable sponge or balloon packing has largely supplanted horizontally-layered gauze due to ease of use. The Rapid Rhino inflatable device has advantages over sponges because of its flexibility and smooth carboxymethyl cellulose hemostatic mesh envelope. Sponges, however, are rigid when dry and nasal abnormalities (e.g., septal deviation) may preclude passage into the nasal cavity or abrade nasal mucosa creating secondary bleeding sites.
The authors described a Foley urinary catheter as one option for the posterior pack, although they discuss more fully and illustrate the gauze technique. The catheter may be placed as the posterior pack much more easily and with less discomfort for the patient. Active posterior hemorrhage commonly provokes patient gagging, which complicates positioning of the gauze above the soft palate at the posterior nasal choana. In contrast, one visualizes the Foley balloon in the oropharynx, inflates it, and then retracts it into position.
The use of oxymetazoline (Afrin) avoids potential cardiovascular effects of phenylephrine and concentrated epinephrine. Oxymetazoline may be mixed at bedside in its own spray bottle with an equal amount of 4% liquid topical lidocaine. The combination may be sprayed into the nose or applied on unrolled cotton balls. Held horizontally, the bottle provides a generous stream rather than mist. Topical anesthetic/decongestant may be supplemented, as available, with intravenous ondansetron (Zofran) and an analgesic to improve patient comfort.
The Foley is passed, inflated, and retracted into the nasopharynx while the assistant maintains firm forward traction. The Rapid Rhino is wetted, inserted, and inflated. An unfolded four-inch gauze pad is wrapped around the Foley shaft to create a doughnut-shaped bolster and tape-wrapped around its circumference. This protects the nostril from pressure necrosis. An umbilical clamp is slid snuggly against the bolster to keep forward tension on the Foley shaft. Surgical ties placed around the Foley shaft prevent balloon deflation; the rest of the catheter shaft is trimmed (see accompanying figure). This reliable posterior packing method takes only a few minutes, and in my experience works better than commercial double-balloon products.
FIGURE
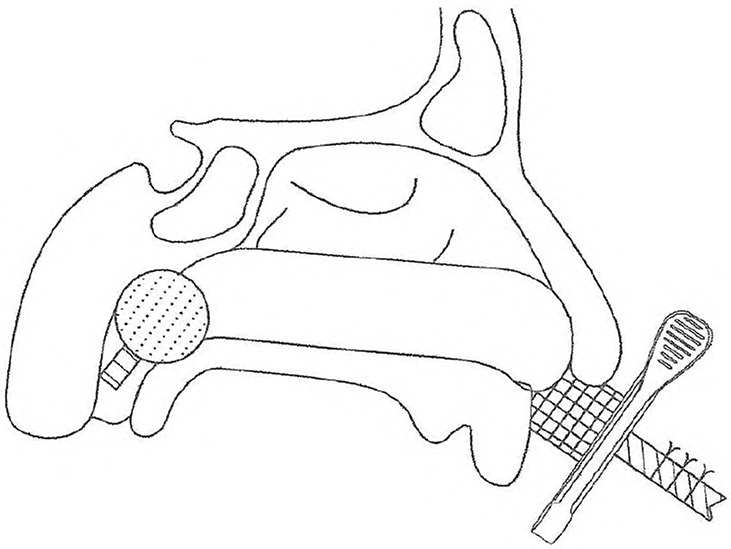
Posterior Foley/anterior Rapid Rhino nasal pack with protective nostril bolster.
