
A variety of forces, from hospitalists to burnout, may be chipping away at family physicians' scope of practice. Should you be concerned?

Of course no one will know with absolute certainty until 20 years after the fact, but there's growing suspicion that the scope of family practice is narrowing. Indeed, there are plenty of potential threats in today's market: hospitalists, midlevel providers, subspecialists, carve-outs, even fellow primary care physicians. But are these threats real and potentially damaging to the specialty, or are they “nothing more than noise at the end of an era,” as suggested by Larry Green, MD, director of the AAFP Center for Policy Studies in Family Practice and Primary Care? Much is unknown, yet much is at stake.
The enemy is us
Never mind for a moment the external forces that may be affecting family physicians' scope of practice. Consider instead that the greatest damage to the scope of family practice may be coming from within the specialty itself as family physicians willingly give up what was once considered sacred.
KEY POINTS:
- Due simply to fatigue and frustration, some family physicians are self-imposing limits to their scope of practice.
- Hospitals and managed care plans increasingly frustrate family physicians' attempts to practice a full scope.
- Because of their versatility and value to patients, family physicians will be able to adapt to the changes in health care.
“There are a lot of emotional issues in life. Birth is one. That's very emotional. Family physicians are getting out of that. We deal with acute illness — if it's in office hours. We no longer visit bed-ridden patients at home or dying patients at home; that's delegated to hospice and visiting nurses. We're not even pronouncing patients sometimes the way we had to in the past,” says Don Cauthen, MD, chairman of the Department of Family Medicine at Scott & White Clinic, a large multispecialty group based in Temple, Texas, and a member of the FPM Board of Editors. “We're separating ourselves, and somebody else is filling those high-emotional-impact times so that we can stay in the office and see colds.”
Of course family physicians treat much more than colds, but evidence points to the fact that family physicians' scope is changing. In 1987, for example, 41 percent of family physicians did obstetrics and 72 percent worked in the ICU; today those percentages are 30 and 55, respectively. (See “Family practice then and now.")
“I think in many if not most of those instances where you see family doctors backing away from the full range of services, if you examine it case by case, they're fatigued,” says Larry Green. “They're just plain tired of the fight and the squabble in their own environment with the other ‘co-predators’ for the health care dollar.”
Family practice then and now
All professions, all specialties, change. Family practice is no exception. In 1980, 53 percent of family physicians made house calls; 68 percent visited patients in the nursing home; and 91 percent provided care in the hospital. But for a variety of reasons, many unknown, these and other segments of family practice appear to be shrinking, according to data from the AAFP.
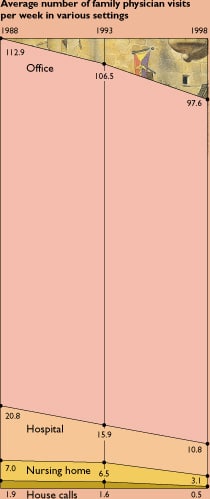
Sources: AAFP. Profile of Office-Based Practice of Active Academy Members, January 1980; Office Practice Characteristics Survey, 1988; Hospital Privileges Survey, May 1993; Practice Profile Survey, 1987 and May 1998.
Such frustration and fatigue may help explain why roughly one quarter of primary care physicians are saying their scope of care is “greater than it should be,” a finding recently published in the New England Journal of Medicine.1 But, says Lee Newcomer, MD, senior vice president for health policy at United Health Group, a Minneapolis-based managed care organization, “I was pleasantly surprised to discover that 75 percent, three out of four physicians, were comfortable with their scope of practice.” He suggests that self-imposed limits on scope of practice may in fact be a good thing, the result of physicians wanting to do superb work. “A key question many physicians ask themselves is ‘Can I do this procedure or therapy as well as anyone?’” he says. “Many physicians may be narrowing their scope of practice to remain highly competent.”
For example, when Park Nicollet Clinic decided to use hospitalists as its inpatient care model, family physicians were given the opportunity to serve in that role. What they found, says Newcomer, is that the physicians migrated to the roles that fit their strengths. “The physicians who chose to become hospitalists enjoyed complex, inpatient admissions and they enjoyed the chaos of inpatient care. They chose their special area of competency,” he says. “Physicians who chose to do outpatient work only showed increased satisfaction with their jobs — probably because they were uncomfortable taking care of inpatients.”
But Cauthen suspects there's more at play than just the desire to be competent. “I think what's happened is, because we're in a relative short supply, family physicians can maintain their income and retract the amount of work they have to do. It's becoming a lifestyle issue,” says Cauthen. “I think we're selling scope of practice for a 40-hour work week.”
Of course physicians can't say that publicly, says Cauthen, “so the language they're using is ‘I'm limiting my scope to provide better service and to be available to my patients in the clinic, and it's probably better quality that I stay in the clinic.’” While the driver is lifestyle, Cauthen says, the rhetoric is something quite different: service, access, quality. And “they're getting away with it,” he says, because the rhetoric is exactly what today's health care organizations want to hear. He worries, however, about the long-term effects: “What ramifications does that have for the discipline when, down the road, we have other primary care competitors? We will have redescribed our discipline based on the seduction of money and an easy lifestyle.”
Richard Roberts, MD, JD, president-elect of the AAFP and professor in the Department of Family Medicine at the University of Wisconsin-Madison, agrees that some family physicians are giving up too much too soon and says that a full scope and a full life should be compatible. “It shouldn't have to be painful, difficult or a lifestyle killer to deliver babies or to be in the hospital,” he says. “We can do this.”
He points to creative solutions, such as rotating hospital duties among family physicians within a group. “I think family physicians who allow themselves to walk completely away from the hospital or from pregnancy care are ultimately going to regret it. And I think the reason they will regret it is that they'll find that their knowledge base shrinks and then they become incompletely trained internists or incompletely trained pediatricians,” says Roberts. “Part of the value [family physicians] bring is the ability to care for people anywhere they are. If we step too far away from that fundamental belief, then we really have begun to undercut our value.”
Steven Green, MD, chairman of the Department of Family Practice at Sharp Rees-Stealy Medical Group in San Diego, has witnessed this struggle among many of his colleagues. “You will have some physicians who, due to burnout or overwork, will start cutting anything they can, and you almost feel like you have to remind them that they've spent a lot of time and training learning how to do these things,” he says. “If they give up hospital work or give up certain procedures, it's a one-way step. They're basically burning a bridge and it's going to be very difficult for them to get that back later.”
Despite cautions like these, many family physicians seem to be dropping their broad scope with little regret and a big sigh of relief. “That's one thing that makes the issue of fighting for scope of practice very difficult. A lot of the doctors themselves don't really seem to be interested in it as an issue,” Steve Green says. “It's very hard to fight a battle on behalf of people when some of them don't care.”
The root of all evil
Reimbursement complicates almost every aspect of medicine, so it's little surprise that the struggle to maintain a broad scope is often frustrated by the matter of money. At issue are reimbursement systems that offer no incentive — or a disincentive — to practicing a broad scope. In many cases, the family physician who practices in the hospital, does obstetrics and is procedurally active is paid the same salary or the same capitation rate as the family physician who refers all these things away.
“If you can't turn in a charge for a procedure and it takes you extra time, you start to say to yourself, ‘Why don't I just send that to dermatology,’ or whatever specialty might do it,” says Steve Green. “It's of course inefficient. The patient has two extra visits, and in the end your scope is more narrow and it's probably less satisfying, but it's hard for people to keep doing things that they're completely unincentivized to do.”
In fact, Steve Green's group is rethinking its compensation method and is eyeing an old-fashioned charge-based system, in which compensation increases with productivity. “We think we're going to get better service levels, and I think it will end up incentivizing what we really want done,” he says.
The solution for other groups may be different: distributing capitation revenues to physicians at rates that are based on their scope of practice. “With one of our IPA's contracts, we have virtually all primary care services covered under capitation — mammography to vasectomies and everything else,” explains Bill Soper, MD, MBA, a family physician in Liberty, Mo., and a member of the FPM Board of Editors. To address the issue of rewarding physicians for the actual work they do, Soper's group hired an actuarial firm to calculate what percentage of the capitation rate various services, such as vasectomies or colposcopy or fracture care, were worth. “So if a primary care physician doesn't do colposcopy or vasectomies, we actually capitate him or her less than we capitate a primary care physician who does do those things,” he says.
“Once we did this study and got through all the numbers, we found out that the differences are infinitesimal. It was like a nickel for a vasectomy. But at least we can say to people, ‘You can't complain, or you shouldn't complain, because you do vasectomies and this guy doesn't, because you're getting paid more on your capitation rate than he does.’”
What of these external threats?
Although financial incentives and disincentives and self-imposed limits on scope of practice can create a wealth of problems all their own, the greater fear for many family physicians is an external threat. “Family physicians appear to be especially nervous about what often seem to be arbitrary changes that are happening or being imposed on them by hospitals and health systems,” explains Roberts.
While this may not be the case in rural or underserved areas, in many parts of the country, hospitals and health plans have begun to impose more and more restrictions on family physicians' scope of practice, including mandatory use of hospitalists, refusal to pay for certain procedures in family physicians' offices, impossible credentialing criteria for obstetrics and so on. “I don't believe this is some sort of plot to erode our scope,” says Steve Green, “but if you have a specialist mentality, you may tend to think that it would be easier to let us ‘focus’ on our ‘regular’ office practice.”
In San Diego, where Steve Green practices, virtually no family physicians do obstetrics because “the hospitals have made credentialing for deliveries almost impossible,” he says. “It's a tremendous uphill battle.”
But it's the sort of battle that can be won — not always, but perhaps more often than is tried. Unfortunately, what tends to happen is that “family docs are so busy and not terribly experienced business people, and so the hospitals or health plans say do this and we say OK,” says Roberts. “But if you care about the patients and you believe in what you do, it means at times you're going to have to stand up on your own two hind legs and take a position and be willing to confront potential conflict.”
For example, when Prudential Health-Care of South Florida attempted last year to set up a mandatory hospitalist program, objections from physicians and specialty societies caused the health plan to overturn its decision. The same thing happened a year earlier when a Humana plan in Texas tried a similar program.
The key to winning those local battles, says Roberts, is to talk the health plan's language. “If they're driven by dollars, then you talk dollars with them,” he says. Show how family physicians can provide “better coverage and higher-quality service at a lower cost.”
In fact, Roberts has data showing the success of family physicians sharing inpatient care responsibilities, a program he is part of at the University of Wisconsin-Madison. The program's average length of stay was 20 percent shorter than that of the general medicine service, its cost of care was 25 percent less, and readmission and death rates did not differ significantly between the two programs. “There's something different about how we think about patients and how we organize ourselves in our care as family docs that serves patients and the community well,” says Roberts.
This too will pass
What sometimes gets lost in the scope-of-practice debate is the clear fact that family practice, whatever its problems, is a strong, versatile specialty with deep roots. Viewed in that light, today's threats may not seem so powerful. “My own personal opinion is that this too will pass,” says Larry Green. “It's a transitory thing, more of an epiphenomenon than anything of substance.”
The debate over “who can do colposcopy” or “who can deliver babies” is driven not by real concerns about the quality of family physicians' care, suggests Larry Green, but by economics — with a dash of ego and ideology. “The way a hurricane takes its energy from warm water, this stuff takes its energy from a relative oversupply of health care professionals, a relatively laissez-faire approach to use of technology and an undisciplined economy all converging to where a bunch of folks are trying to squeeze a living out of the health care system and maintain last year's income plus 4 percent.”
He adds, “All of this is just noise at the end of an era. When you look at what a mess the health care system is, many people would offer the analysis that it's the ending days of an old system that is destined to totally rearrange itself into a new format.”
That new format will absolutely have a place for the broadly trained family physician who provides comprehensive, continuous care to a large population of all ages, says Roberts. “Look around the world,” he says. “Every other health system that is successful is based on that.”
The scope of practice that will sustain the family practice model and benefit patients now and into the future is this, says Larry Green: “the ability to receive any problem that a person of any age and of either sex chooses to bring to the health care system and to definitively resolve it a large majority of the time and the rest of the time be able to organize it in a way so that positive progress can be made toward the solution of that problem — and doing this right the first time.
“That's the scope and the quality of what a family physician really is and is going to continue to be,” he says. “As near as I can tell, all health care systems invent this person. It seems to be grounded in human need, and I don't believe there's much evidence that it will ever go away.”
Beyond turf battles
As family physicians fight for a broad scope and to demonstrate the value of the specialty, their instinct may be to stake out their territory with stone walls and defy anyone to assail them. But “where are we going to draw all the borders?” asks Larry Green. “I think you fight those locally one at a time as necessary to sustain the scope of practice that allows a family doctor to be a robust general physician taking care of most of the problems most people have most of the time. … But there's no reason to spill blood, in my opinion, over any single CPT-IV code.”
In fact, the problems patients bring to the health care system don't always fit neatly into the buildings and reimbursement structures that have been created. “Congestive heart failure has this nasty habit of not being confined to the hospital. It's also not confined to the office. Nor is it confined to the home, nor the nursing home. And its solutions and dealing with it are not amenable to mere angioplasty or a particular drug or combination of drugs or just nutrition or just exercise or just the right family setting or just the right support system. It is all of the above,” says Larry Green.
The solution isn't to define the borders and win out over chiropractors or pediatricians or nurse practitioners. “[Patients] want us to think outside these old models and are pretty frustrated with the health care system overall,” says Larry Green. “It's a terrible mess that's not amenable to saying, ‘Let's get a rule book out and decide what the procedures are that a nurse can do and that a doctor can do, etcetera, and let's draw those lines and then we'll really have this figured out.’ It's so amazingly naive.”
Instead, family physicians will need to “rethink how we do what we do while believing in and remaining true to our core value, which is that every person needs and deserves someone who looks out for all of them. That's really the fundamental issue,” says Roberts. “What you have to do as a family doctor is remain true to what brought you to the party. Why are you there in the first place? To provide comprehensive care to a defined population of patients where you serve as their primary health adviser and guide through the health system.”
Truly focusing on the patient and meeting his or her needs will ultimately resolve the debate about scope of practice, says Larry Green. “The patient is about to become the center of the health care system, and family doctors will hug their patients dearly. They'll pull them close and be their coach, defender, their helper, their aid, their servant, their healer in a number of ways, and will protect them from harm as best they can while assuring them of access to the best that medicine can offer for the problems they have and their situation,” says Larry Green.
“This is not a trivial task. This is not a limited scope of practice. This is a function that America's best and brightest will aspire to. It's the stuff of which a meaningful life is made, from which a career blossoms, the sort of thing that someone can be grateful that they had the opportunity in their lifetime to do that and to be one of those. It's unbelievably exciting.”
