
This supplement shares data from the CDC-funded American Academy of Family Physicians (AAFP) Alcohol Screening and Brief Intervention Office Champions Project and describes the impact alcohol SBI made on patient care.
Introduction
Excessive alcohol use is often unrecognized and underreported by patients. Unless questioned, patients may not disclose how much they drink and may fail to recognize the adverse effects of alcohol on their health. Screening and brief intervention (SBI) for alcohol use is a validated, evidence-based intervention to detect unhealthy drinking in the primary care setting and motivate patients to alter their behavior.1 The U.S. Preventive Services Task Force (USPSTF) “recommends screening for unhealthy alcohol use in primary care settings in adults 18 years or older, including pregnant women, and providing persons engaged in risky or hazardous drinking with brief behavioral counseling interventions to reduce unhealthy alcohol use.”2 However, incorporating alcohol SBI in the office setting can be challenging for family physicians due to time constraints, lack of training and comfort, and scarce resources.
Universal screening of patients during a health maintenance visit is an ideal opportunity to inquire about unhealthy alcohol use, but screening can be done at any time at the discretion of the physician. Screening everyone ensures equitable care, increases patient acceptance, and reduces stigma. In particular, family physicians are in a prime position to address risky alcohol use in patients who are pregnant or may become pregnant. The Centers for Disease Control and Prevention (CDC) estimated binge drinking or excessive alcohol use by 12.6% of adult women in 2018.3 Screening women of reproductive age and counseling them that no level of alcohol use is safe during pregnancy is an important step to prevent fetal alcohol spectrum disorders, which can cause learning disabilities, abnormal facial features, congenital disabilities, and poor growth in affected children.
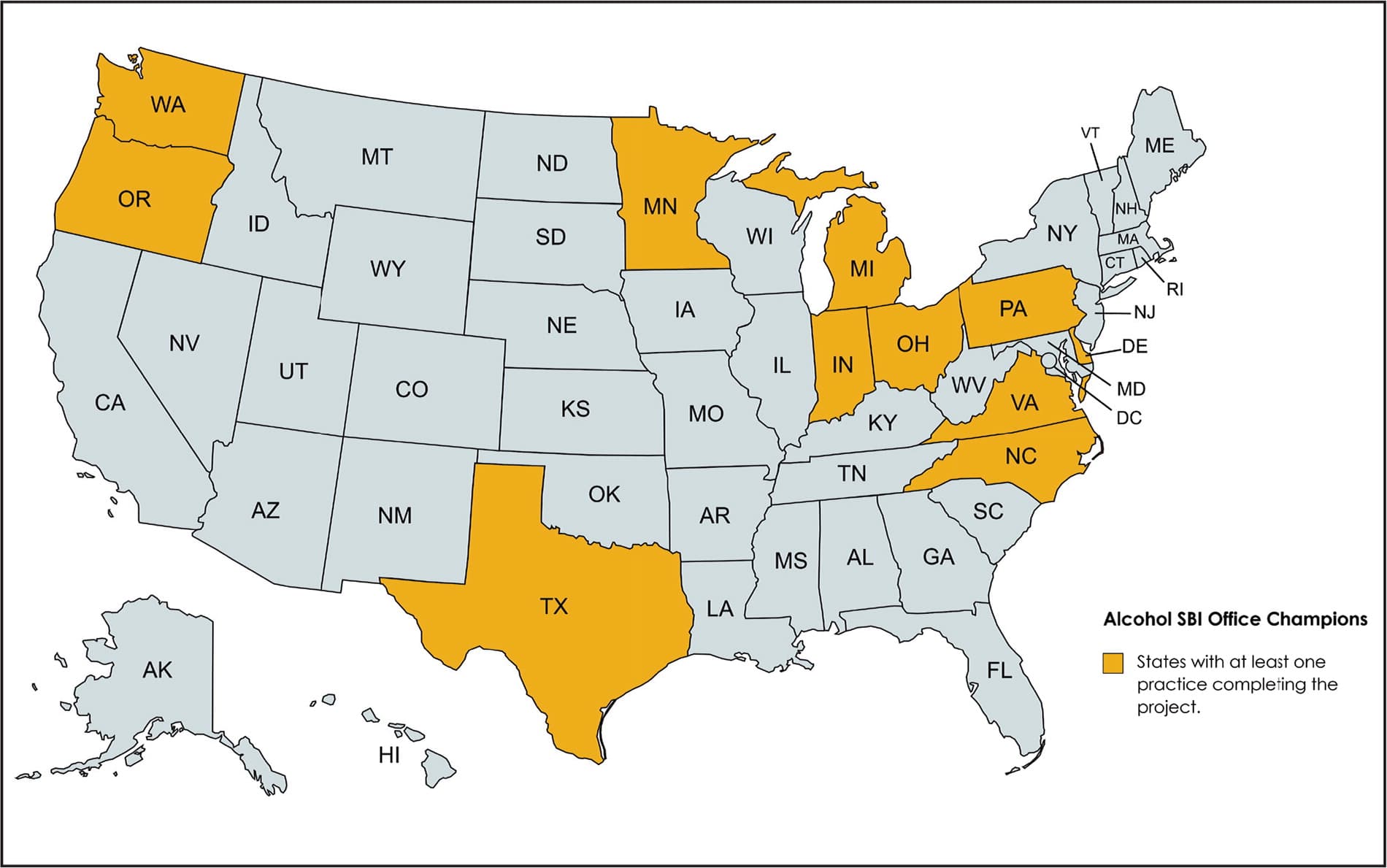
In this supplement, we will share data from the CDC-funded American Academy of Family Physicians (AAFP) Alcohol Screening and Brief Intervention Office Champions Project and describe the impact alcohol SBI made on patient care. As part of this project, 14 family medicine practices located throughout the United States (Figure 1) implemented alcohol SBI. The participating practices comprised seven family medicine groups, four multispecialty groups, two solo practices, and one safety net clinic. Two practices were in rural settings, four were in suburban settings, and eight were in urban areas. Two practices withdrew from the project due to staff turnover that included the physician and office champions. In addition, practices in four states expressed interest in joining the project after it had started.
Figure 1. Map of participating practices
Brief Summary of the Alcohol SBI Office Champions Project
In 2019, the AAFP initiated the Alcohol SBI Office Champions Project under a CDC grant. This project aimed to train family physicians on alcohol SBI to enable them to implement lessons learned in their daily practice. The project took place over the course of two years and included baseline measurement of alcohol screening by participating practices, an implementation phase, a second round of measurement, and a sustainability plan.
The Baylor Family Medicine Clinic facilitated the initial training for physician and office champions, providing tools and resources to help these individuals embark on the new journey successfully. Physician and office champions were trained on alcohol screening and the components of brief intervention with the expectation that they would disseminate this new knowledge at their practices. Training of all staff is very important for a team-based approach to be successful.
Most Frequently Used Screening Tools
Approximately nine in 10 adults who drink excessively in the United States do not meet the diagnostic criteria for severe alcohol use disorders (i.e., alcohol dependence).4 Therefore, it is important to use screening tools that will identify nondependent people who drink excessively as well. The Single-Item Alcohol Screening Questionnaire (SASQ) is short, simple to administer, and easy to remember. The Alcohol Use Disorders Identification Test-Consumption (AUDIT-C), which can also be administered in about a minute, comprises the first three questions of the full 10-question Alcohol Use Disorders Identification Test (AUDIT-10). For people who screen positive on the SASQ or the AUDIT-C, a more comprehensive follow-up with the AUDIT-10 should be performed.2
SASQ5: How many times in the past year have you had X or more drinks in a day? (X = five for men; four for women)
- How often do you have a drink containing alcohol?
- How many drinks containing alcohol do you have on a typical day you are drinking?
- How often do you have X or more drinks on one occasion? (X = five for men; four for women and for men over age 65)
Project Findings
Data on the effectiveness of the Alcohol SBI Office Champions Project were collected using chart audits. Each participating practice randomly pulled 50 charts and provided information about screening and intervention before the project started (baseline measure) and after the quality improvement (QI) activities (post-implementation measure). Altogether, 983 charts were reviewed at baseline and 933 charts were reviewed at the second measurement.
Baseline and post-implementation data were compared for screening and intervention activities (Figure 2). The screening rate increased for both men and women. For instance, only 59% of women were screened at baseline, whereas 70% of women were screened after QI activities were implemented. Likewise, the screening rate for male patients increased from 66% to 72%. The positive screening rate (i.e., percentage of people who screened positive for excessive alcohol use among those screened) increased for women but decreased for men. However, the intervention rate increased for both men and women. Of those who screened positive, only 24% of women and 21% of men received intervention at baseline, whereas the percentages increased to 43% for women and 59% for men after QI activities.
Figure 2. Screening and intervention rates
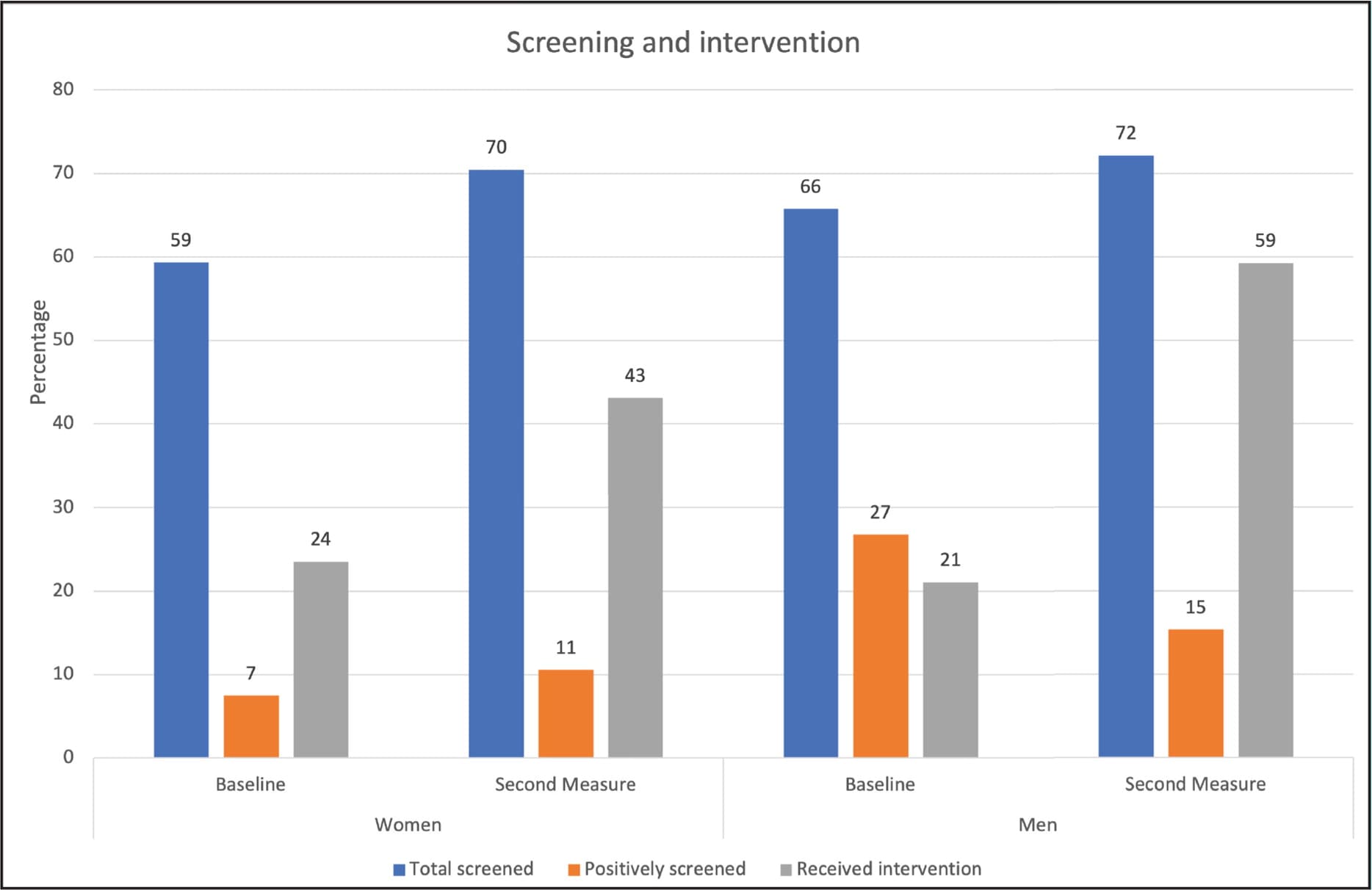
Total screened = percentage of patients screened among total chart reviews; positively screened = percentage of screened patients who had excessive alcohol use; received intervention = percentage of positively screened patients who received intervention.
Baseline and second measures showed that medical assistants (MAs) conducted the most screenings, followed by physicians and nurses. After QI activities were implemented, the percentage of physicians conducting screenings increased substantially, whereas the percentage of nurses conducting screenings decreased. There was also an increase in screening by physician assistants (PAs) at the second measurement. The increase in screening by physicians and PAs could be attributed to their deep engagement in the project as champions. In Figure 3, the inner circle represents the baseline measure and the outer circle represents the post-implementation measure.
Figure 3. Health care team members involved in alcohol screening at baseline and after QI activities
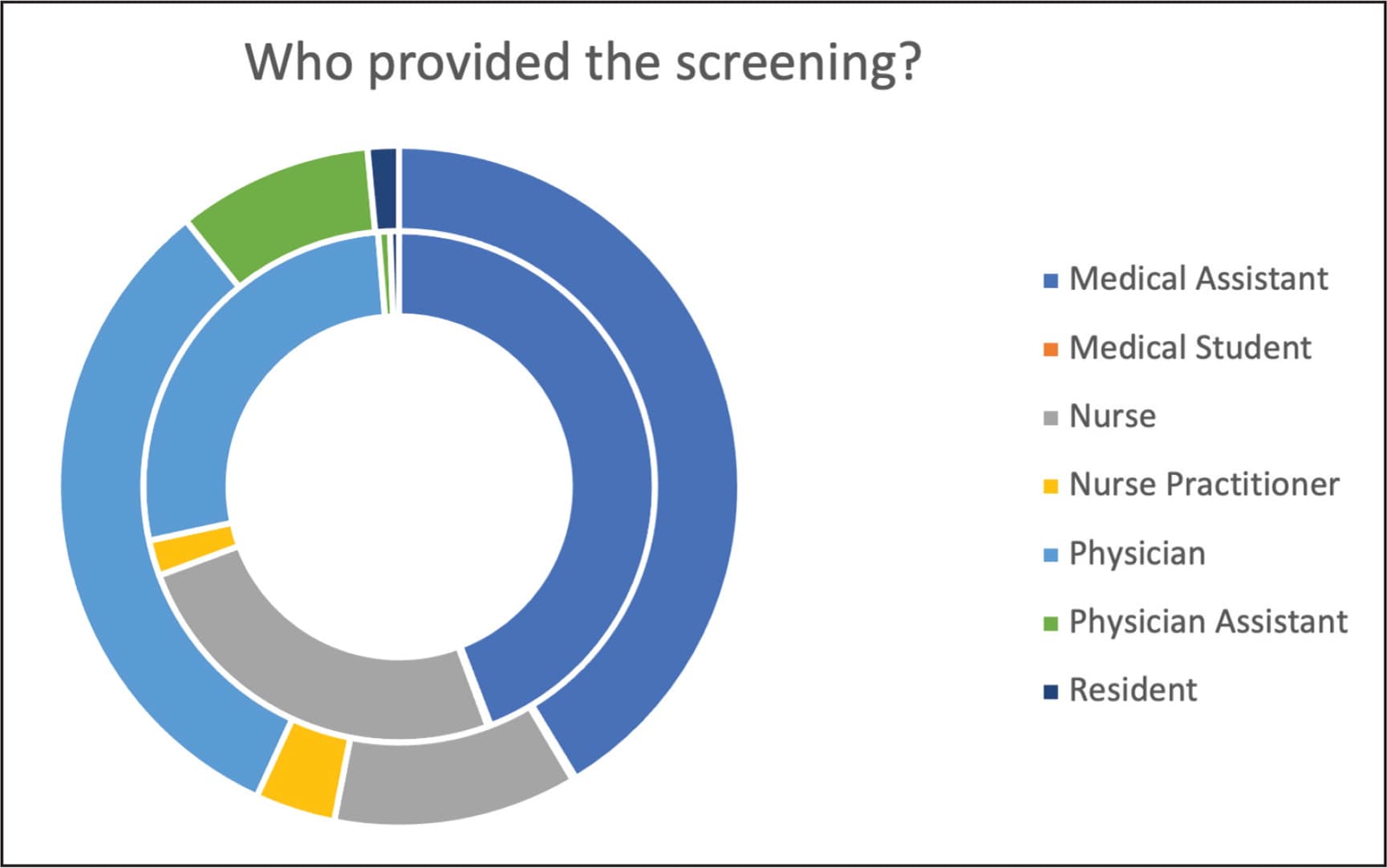
Inner circle = baseline measure; outer circle = post-implementation measure.
During both the baseline and post-implementation measurements, practices indicated that the SASQ was the health care team's preferred screening tool. After QI activities were implemented, use of the AUDIT-C increased substantially. The AUDIT-C provides more comprehensive information on a patient's excessive alcohol use, so the increased use of this screening tool suggested the use of tailored interventions. During the second measurement, we identified more diverse interventions that practices used, such as scheduling separate appointments and providing resources to patients. However, a brief intervention was the preferred choice of intervention at both data points.
Within the brief intervention, clinicians primarily advised patients to reduce or abstain from alcohol use and assessed whether they were willing to do so. Only a few clinicians assisted patients in developing a plan or arranged follow-up appointments. Some participating practices had an integrated behavioral health program to carry out behavioral intervention. In most charts, the reasons for not providing interventions were not noted. Among those reported, time constraints and refusal by the patient were the primary reasons for not providing interventions.
Overall, we found that implementing the alcohol SBI office champions model helped family physicians and their teams screen all adult patients for excessive alcohol use, target high-risk patients by exploring whether the patient was trying to become pregnant, and provide interventions accordingly.
Impact for Health Care Teams
The data obtained by the Alcohol SBI Office Champions Project showed that screening can be performed by any clinician after proper training. The number of screenings performed by physicians increased after QI activities were implemented. We believe this is due to the increased awareness of and interest in alcohol SBI generated in practices as part of the project. It was encouraging to see that some practices utilized medical students to conduct screenings because this provided a great learning opportunity for the students. The SASQ was the screening tool most frequently used by participating practices. This could be due to the small amount of time required for screening with the SASQ and its ease of use. In post-implementation measures, more nurse practitioners and PAs appeared to be screening patients. After the QI activities, the rate of brief intervention for patients who had a positive screen increased in both men and women compared to baseline.
Impact on Patient Care
Participating in the Alcohol SBI Office Champions Project gave practices an evidence-based prevention approach to address risky alcohol use and help patients make healthier choices about drinking.
One practice found that the office champions project gave them a starting point for conversations with patients about both alcohol use and contraception, such as when a 22-year-old female patient came in for her yearly well-woman exam. An MA conducted an alcohol screening, and it was positive. The patient reported that she would often binge drink at social events and parties, as would many of her friends. Although she was not interested in a referral to behavioral health, she was interested in learning more about the negative impacts of binge drinking and discussing safer alcohol use behaviors.
It was also noted that the patient was sexually active and frequently engaged in unprotected intercourse. After her physician explained the devastating impact that alcohol use can have on a developing pregnancy, the patient was interested in learning more about contraception options. Ultimately, she was scheduled for intrauterine device (IUD) placement. In this case, a screening question from the MA led to brief intervention by the physician that had significant impact on the patient. Screening and brief intervention resulted in changes in the patient's alcohol use behavior, reduced her risk of unintended pregnancy, and, through both education and contraception, reduced the risk of fetal exposure to alcohol.
In another instance, a patient came in for her annual health checkup. Because of the COVID-19 pandemic, she had not seen her physician for two years. The patient shared that she had been working remotely from home. Like many patients who resorted to alcohol for stress relief during the pandemic, she had been drinking five to six alcoholic beverages on several days of the week. Using skills acquired during training on alcohol SBI, the physician performed the validated single-question screening followed by the full AUDIT-10. Both revealed excessive alcohol use by the patient. Her physician reviewed alcohol drinking limits with her (i.e., not to exceed three drinks in one setting or seven drinks per week) and worked with her to devise a plan to cut down. In addition, arrangements were made for the patient to meet with the practice's behavioral health team for follow-up. The patient was accepting of the intervention. Reflecting on the practice's participation in the office champions project, the treating physician noted, “This project helped our health care team feel more comfortable discussing excessive drinking with our patients in the same way that we would discuss diabetes or hypertension, and it also allowed us to provide more comprehensive care.”
Participating practices also saw the value of using validated tools for alcohol SBI. For example, prior to the Alcohol SBI Office Champions Project, a physician at one practice gave generic advice to patients who drank alcohol: “Cut down and stop drinking as it is not good for health.” The physician was surprised when she saw a 68-year-old woman who screened positive for excessive alcohol use. The patient laughed and said that four drinks would not “get her anywhere,” so she usually drank six to seven cans of beer when she met with her girlfriends. The physician took this opportunity to educate the patient on recommended alcohol drinking limits and encourage her to talk to her friends about setting appropriate limits the next time they were together. Given the patient's recent diagnosis of diabetic myopathy, her physician also explained how alcohol can affect diabetes and increase fall risk. Using a validated tool allowed this practice to systematically identify patients with excessive alcohol use so the health care team could provide education and raise awareness. In addition, the physician discovered that only a few of her patients who drank alcohol had alcohol use disorder, but most had a history of excessive alcohol use. These patients often lacked awareness of alcohol use limits and were open to feedback and education.
Conclusion
It is not uncommon for physicians to meet roadblocks when it comes to implementing a practice change. Ideas for practice improvement may affect office workflow, be rejected by colleagues, or not align with other institutional priorities. Physicians must influence leadership and gain buy-in to implement changes. Sharing the advantages of a QI project and providing resources for implementation can increase acceptance by the practice. Using a team-based approach increases staff awareness and understanding leading to sustainable workflow changes. Incorporating alcohol screening and brief intervention is beneficial for patients and is worth the effort of advocating for change.
