
Confusion around the code has contributed to low usage. This infographic explains when to use (and not use) G2211 and what changed on Jan. 1, 2025.
Update: On Jan. 1, 2026, CMS expanded the list of codes that can be reported with code G2211 to include home or residence E/M codes (CPT codes 99341, 99342, 99344, 99345, 99347, 99348, and 99350).

The Centers for Medicare & Medicaid Services (CMS) introduced HCPCS add-on code G2211 in January 2024 as a way to recognize that the longitudinal patient relationship has complexity beyond the work captured in standard office/outpatient visit evaluation and management (E/M) codes. Physicians can add G2211 to E/M codes 99202-99205 or 99211-99215 in either of the following scenarios: 1) you serve as the patient's “continuing focal point for all needed health care services” or 2) your services “are part of ongoing care related to a patient's single, serious condition or a complex condition.”1
For primary care physicians, this means you can use G2211 for your own patients, whether the visit involves an acute problem (e.g., sinus infection) or a chronic problem (e.g., diabetes) and whether the patient is established or new — as long as they are establishing care with you. The deciding factor is your continuing relationship with the patient.2
“The complexity that code G2211 captures isn't in the clinical condition … The complexity is in the cognitive load of the continued responsibility of being the focal point for all needed services for this patient. There's important cognitive effort of using the longitudinal doctor-patient relationship itself in the diagnosis and treatment plan. These factors, even for a simple condition like sinus congestion, make the entire interaction inherently complex.”3
KEY POINTS
- The Centers for Medicare & Medicaid Services introduced add-on code G2211 in January 2024 to recognize the complexity of the longitudinal patient relationship beyond that captured in standard office/outpatient visit E/M codes.
- As of Jan. 1, 2025, G2211 can also be used in conjunction with visits requiring modifier 25 in certain situations: an annual wellness visit, vaccine administration, or other Medicare preventive service.
- Due to confusion about when to use the new code, usage was low in 2024, prompting the creation of an infographic to help clinicians understand and confidently use G2211.
NEW FOR 2025
Previously, CMS did not allow G2211 in conjunction with visits requiring modifier 25; however, as of Jan. 1, 2025, Medicare will pay for G2211 alongside modifier 25 in some situations.4 When you provide an annual wellness visit, vaccine administration, or other Medicare Part B preventive service to the patient on the same day you provide an office/outpatient E/M service (attaching modifier 25 to the E/M code to indicate that it is a significant, separately identifiable service), Medicare will now allow payment for G2211.
AN INFOGRAPHIC
Because of confusion about when to use the new code, usage was low in 2024 in many practices, including mine. Based on the hypothesis that the rules for using G2211 simply had not been communicated in a way that clinicians could confidently understand, I worked with our department's billing specialist to create an infographic (below) on when to use G2211. The feedback from my colleagues has been positive, and they report feeling more confident in using the new code.
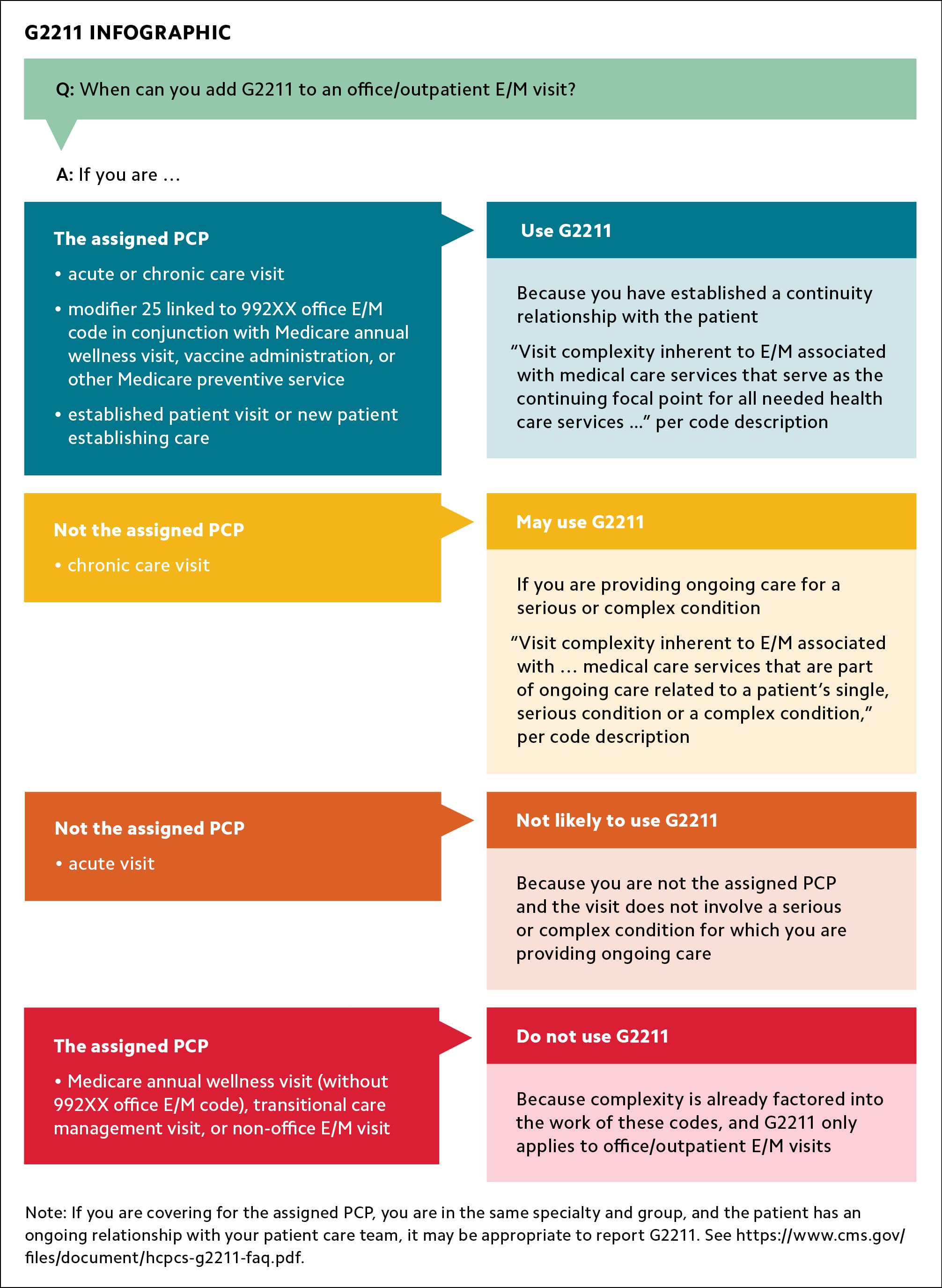
Note: If you are covering for the assigned PCP, you are in the same specialty and group, and the patient has an ongoing relationship with your patient care team, it may be appropriate to report G2211. See https://www.cms.gov/files/document/hcpcs-g2211-faq.pdf.
GETTING PAID
While Medicare covers add-on code G2211, private payer coverage varies. The American Academy of Family Physicians (AAFP) has compiled a list of confirmed national payers:
- Aetna (Medicare Advantage),
- Anthem (Medicare Advantage),
- Cigna (Medicare Advantage),
- Humana (Medicare Advantage),
- United Healthcare (Medicare Advantage).
The AAFP will update the list (available as a Word file) as new information becomes available.
