Pediculosis and scabies are caused by ectoparasites; patients usually present with itching. Head and pubic lice infestations are diagnosed by the visualization of insects or viable nits (eggs). Primary treatment is topically administered 1 percent permethrin. Malathion is one alternative for treatment failures. The importance of environmental measures to prevent infestation is a matter of controversy. Pubic lice are treated the same as head lice, but this finding should prompt evaluation for other sexually transmitted diseases. Body lice infestation should be suspected when symptoms of generalized itching occur in persons who do not change or wash their clothing or bedding regularly; lice may be found in the seams of their clothing. Topically administered permethrin may help to eradicate body lice, but personal hygiene measures are essential for successful treatment. Classic scabies in adults can be recognized by a pruritic, papular rash with excoriations; in infants, small children, and the immunocompromised, the rash may include vesicles, pustules, or nodules. Primary treatment for scabies is permethrin cream, and environmental measures are important to prevent recurrent infestation. Generalized crusted scabies is best treated with oral ivermectin.
Pediculosis and scabies are closely related skin conditions caused by arthropods. Although these conditions typically cause severe itching, they generally are benign. Pediculosis and scabies have similar treatments.
Pediculosis
The three lice species that infest humans are Pediculus humanus capitis—head louse (Figure 1, left), Phthirus pubis —crab or pubic louse (Figure 1, right), and Pediculus humanus corpus—body louse. All three insects are obligate human parasites. Contrary to popular belief, these insects do not hop, jump, or fly. Rather, they are transmitted by person-to-person contact.
Despite the introduction of new treatments, the frequency of lice infestation may be increasing. One explanation may be the development of resistance to current treatments.1,2 Fortunately, head and pubic lice do not transmit systemic disease. Hence, treatment is directed at relieving symptoms and preventing reinfestation and transmission.
CLINICAL PRESENTATION
Itching is the primary symptom of pediculosis. It is the result of an allergic reaction to louse saliva and takes two or more weeks to develop. By this time, the infestation is well established.
DIAGNOSIS
Head and pubic lice infestations are diagnosed by finding lice or viable eggs (nits) on examination. Excoriations and pyoderma also may be present.
Lice can be difficult to detect. A bright light, a magnifying lens, and separating the hair aids inspection. However, combing through the hair with a louse comb and examining the teeth of the comb for living lice detects more cases than direct visualization alone.3 The presence of a single live louse is adequate for the diagnosis of active infestation. The presence of nits only does not necessarily indicate active infestation.4 If only nits are found, they should be examined microscopically for viable embryos (Figure 2).
The diagnosis of body lice may be suggested by the presence of pruritus in homeless persons or in persons who live in situations in which bedding and clothing are not changed regularly. Examination may show generalized excoriations. In addition, body lice should be confirmed in the seams of clothing.
LIFE CYCLE OF HEAD LICE
The head louse begins as an egg laid near the scalp and “glued” firmly to a hair shaft. After three to four days, the embryo's central nervous system is fully developed. It hatches as a nymph in seven to 10 days. Nine to 12 days after hatching, the nymph develops into a sexually mature male or female.
Within 24 hours of mating, the mature female louse begins laying seven to 10 eggs a day. Repeated fertilization is not required. Head lice of both sexes have a life span of as much as 30 days. They survive only 15 to 20 hours off the host.
Nymphs and adult head lice take frequent blood meals, contributing to the symptoms of itching.
TREATMENT OF HEAD LICE
Most topical and systemic treatments are toxic to the nervous system of the louse. Because some developing embryos survive initial treatment, a second course of treatment, seven to 10 days after the first course, is recommended to kill newly hatched nymphs.
Topical Agents
In the United States, several topical agents are available for the treatment of head lice infestation. All over-the-counter agents approved by the U.S. Food and Drug Administration (FDA) belong to the pyrethrum group of insecticides (pyrethroids). Both 4 percent piperonyl butoxide–0.33 percent pyrethrins (e.g., Rid, Pronto) and 1 percent permethrin (Nix) are safe and effective. Experts consider permethrin the treatment of choice.5
The pyrethrum insecticides are pregnancy category B drugs. Their safety in breastfeeding is unknown.
A 0.5 percent malathion lotion (Ovide) is available by prescription.6 It is highly effective in the treatment of resistant head lice infestation in the United States. Because of its odor, flammability, and potential for causing respiratory depression if ingested, malathion is considered a second-line agent. Malathion should not be used in neonates and infants; its safety in nursing mothers and children under six years of age is uncertain. Malathion is a pregnancy category B drug.
Two recent evidence-based reviews found that malathion, permethrin, and pyrethrum insecticides were equally effective in treating head lice infestations.7,8 [Reference 8—Evidence level A, randomized controlled trial]
A 1 percent lindane shampoo is also used to treat resistant head lice infestations. However, lindane shampoo is used infrequently now because of concerns about neurotoxicity, resistance, and slow killing time.
Topical agents are more likely to be effective when they are applied to dry hair.9 Successful treatment requires strict adherence to directions for application. The importance of environmental measures is controversial. A recent study10 failed to show that nit removal improved treatment efficacy. Screening of household contacts and treatment of those infested or sharing the same bed as the index case may reduce reinfestation. Treatment should be repeated after seven to 10 days if live lice are present.
Oral Agents
Ivermectin (Stromectol), in an oral dose of 200 mcg per kg, effectively kills nymphs and lice, but not eggs. To kill newly hatched nymphs, a second dose should be given seven to 10 days after the first dose. Treatment with this agent occasionally is associated with mild, transient side effects such as rash or pruritus, but no serious adverse reactions have been reported.
Pediculosis is not an FDA-labeled indication for ivermectin. In the United States, the drug is not labeled for use in children weighing less than 15 kg (33 lb). Ivermectin is a pregnancy category C drug, and safety in breastfeeding is unknown.
Trimethoprim-sulfamethoxazole (Bactrim, Septra) has been used in the treatment of head lice infestation, although frequent allergic reactions and treatment failure limit its efficacy.11 Trimethoprim-sulfamethoxazole is not toxic to the louse; instead, it acts by killing essential bacterial flora in the insect's gastrointestinal tract.
Treatment Failure
Causes of treatment failure are listed in Table 1. Resistance should be suspected if live lice are still present 12 to 24 hours after treatment and no other cause for failure can be found. Resistant infestations should be treated with an agent from a different insecticide class (e.g., malathion when a pyrethrin or permethrin product was initially used). Treatment with a second agent in the same class (e.g., pyrethrin for permethrin) will result in another failure. Higher concentrations or longer application times for the same agent kill few additional resistant lice.2
Alternative Therapy
Patients who do not wish to use topical insecticides or systemic agents to treat head lice infestation may try alternative treatments. Many over-the-counter herbal shampoos and pomades are available, but they have not been tested for efficacy. Cure through physical removal alone has demonstrated a 38 percent cure rate in one study.12 Head shaving is also effective.
Lice, including nits, are difficult to kill by suffocation. Applying olive oil or petrolatum ointment and covering the head with a shower cap for four to six hours a day for three or four consecutive days may succeed. However, olive oil and petrolatum ointment are difficult to remove from the hair after treatment. Petrolatum ointment, however, is the preferred treatment for infestations of the eyelashes and eyebrows.
Environmental Measures
Although nit removal after treatment is often difficult and controversial, some think it may improve efficacy and reduce the risk of transmission before a second treatment. Use of a 50 percent vinegar and water rinse after shampooing may help slightly with nit removal.13 Thorough wet-combing with a nit comb aids in nit removal. Use of a hair conditioner makes wet-combing easier.
Bedding and recently worn clothing may be decontaminated by hot-water washing (60°C [140°F]) and heated drying, or by dry cleaning. Brushes, combs, and hair ornaments may be soaked in hot water for 10 minutes. The importance of these measures, however, is controversial. Concurrent treatment of infested personal contacts and persons sharing the same bed may prevent reinfestation. Extensive environmental measures, such as spraying pediculicides on furniture, are unnecessary. Mass school-wide screening and “no nit” policies for school reentry have not been shown to be effective.
PUBIC LICE
Pubic lice are readily transmitted sexually. Perhaps they occasionally may be transmitted through contaminated clothing or towels, although this is controversial. The presence of pubic lice should prompt an evaluation for other common sexually transmitted diseases, such as chlamydial infection and gonorrhea. Treatment is the same as for head lice. Sexual contacts also should be treated if infested.
BODY LICE
Patients with body lice infestations should wash their entire body thoroughly and then put on clean clothing. If the infestation is severe, topically administered permethrin, pyrethrin, or malathion also may help. Oral ivermectin is an alternative to topical treatment. Clothing and bedding should be decontaminated by hot-water washing (60°C) and heated drying, or by dry cleaning.
Body lice may transmit typhus and trench fever. Outbreaks of trench fever have occurred in homeless persons in the United States.14
Scabies
Scabies is caused by the parasitic mite Sarcoptes scabiei (Figure 3). Although intense pruritus, papular rash, and excoriations are characteristic, variable forms exist and may mimic other conditions.
CLINICAL PRESENTATION
In adults, classic scabies presents as a pruritic, papular rash with excoriations. The itching in scabies is caused by a delayed hypersensitivity reaction to mites, eggs, and fecal pellets. Papules and burrows generally follow a characteristic distribution, with the head and neck typically spared (Figure 4).
FIGURE 4.
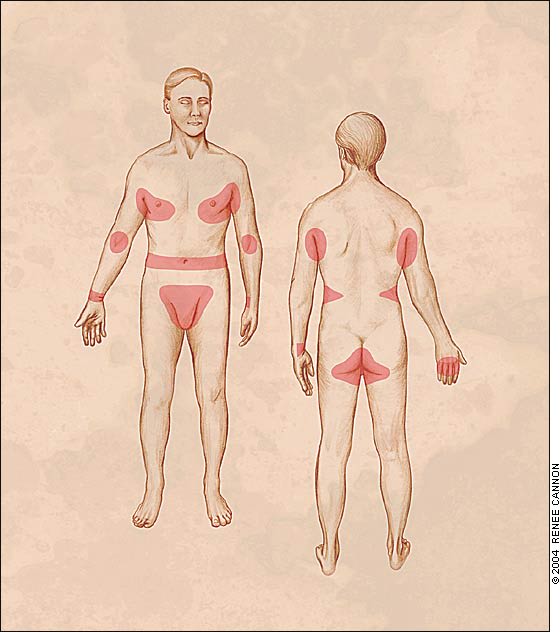
Characteristic distribution of lesions in adults with classic scabies. Burrows are more common on hands and wrists, whereas papular or nodular lesions generally are present elsewhere.
In infants and small children, the scabies rash may include vesicles, pustules, or nodules, and the head and neck may not be spared. The lesions are generally distributed but are concentrated especially on hands and feet and in body folds (Figure 5).
Scabies should be suspected when an elderly patient has an intensely pruritic condition. In the elderly, scabies lesions may be bullous. The rash often is misdiagnosed and treated with a topically administered steroid, which leads to crusting and diffuse erythema. Papules are often scant. Excoriations are frequently prominent on the buttocks and back.
FIGURE 5.

Papular scabies rash in a child's axilla. Papular lesions often are present under the breasts, around the belt line, and on the penis.
Immunocompromised patients with scabies may have crusting of lesions, and itching may be absent. The crusting may be localized or generalized. Patients with human immunodeficiency virus infection sometimes have papular or even nodular eruptions.
LIFE CYCLE OF SCABIES MITE
Like pediculosis, scabies is caused by an obligate human parasite that is transmitted by human-to-human contact. Scabies mites can survive up to four days off the host. During that time, reinfestation is possible. The female mite burrows under the skin and, before dying, lays 10 to 25 eggs. Three days later, the eggs hatch. The larvae move to the skin surface and mature into adults after 14 to 17 days.
DIAGNOSIS
The combination of a history of pruritus (especially at night), a classic rash, and itching in household or sexual contacts is adequate for the diagnosis of scabies. Mites seen on microscopic examination of skin scrapings confirm the diagnosis.
Skin scrapings obtained from the leading edge of the burrow and under the fingernails are most likely to produce a mite. Slicing through the stratum corneum with a no. 15 scalpel blade and examining the burrow under magnification also may visualize mites. For the diagnosis of scabies, skin scrapings have high specificity but low sensitivity. Punch biopsy of a burrow is often unsuccessful in identifying mites or eggs. If treatment fails to improve symptoms after two to three weeks, skin scrapings are essential for diagnosis.
TREATMENT OF CLASSIC SCABIES
Topical Agents
In adults and children over five years of age, 5 percent permethrin cream (Elimite) is standard therapy for scabies. This agent is highly effective, minimally absorbed, and minimally toxic. Adverse effects include itching and stinging on application. After the patient bathes or showers, 5 percent permethrin cream is applied to the entire body from the neck down. The cream is washed off after eight to 14 hours. Unless new lesions develop within 10 days, retreatment is unnecessary.
The 5 percent permethrin cream may be used in infants more than two months of age. In children less than five years of age, the cream must be applied to the head and neck, as well as the body.
Permethrin is a pregnancy category B drug and has been used without apparent ill effects in pregnant women. Its safety in breastfeeding is unknown. When a nursing mother has to be treated with permethrin, it would be appropriate for her to bottle-feed her infant and discard pumped breast milk until residual cream has been washed off thoroughly.
Previously, 1 percent lindane lotion was the standard treatment for classic scabies. Although lindane is generally effective, treatment resistance has occurred.15 The chief advantage of lindane is its low cost (Table 2). The primary disadvantage is the potential for neurotoxicity, if misused, which may be increased in patients with major breaks in their skin (e.g., those with crusted scabies) or in infants and small children. Lindane lotion is applied like permethrin cream, but it is washed off after six hours and reapplied one week later.
A 10 percent crotamiton cream (Eurax) can be applied to scabies nodules in children. The cream should be left on the nodules for 24 hours, washed off, and then reapplied for an additional 24 hours.16
In newborns and pregnant or lactating women with classic scabies, 5 or 10 percent precipitated sulfur in petrolatum is probably effective.17 However, there are no controlled trials of efficacy or safety. This agent is inexpensive and can be made by a compounding pharmacy. It should be applied to the entire body (including the head and neck in newborns) for 24 hours and then reapplied every 24 hours for the next two days. A bath should be taken before each application and 24 hours after the last application. All clothing and bed linens should be changed when treatment is completed. Environmental control is essential for successful treatment.
When a scabicide is prescribed, the patient (or a parent or other caregiver) should be informed that itching may persist for up to four weeks after successful treatment. It may take that long for the skin to slough residual mite debris and for the allergic reaction to subside. Itching may be managed with antihistamines and, if necessary, the addition of a topical steroid. However, steroids should not be prescribed before the completion of primary therapy.
Environmental Measures
Once scabies has been diagnosed, the physician should explain its basic epidemiology. Otherwise, medication alone might be relied on to eradicate the infestation. If environmental control measures are not instituted, treatment failure will occur, because mites are able to survive and reinfest the patient. Thus, it is critical to decontaminate all linens, towels, and clothing used in the previous four days by hot-water washing (60°C) and heated drying. Items that cannot be washed in hot water should be dry cleaned or sealed in a plastic bag for five days. Even if household and sexual contacts have no symptoms, they should follow the same cleaning procedures. Treatment must be simultaneous for all.
GENERALIZED CRUSTED SCABIES
Two issues must be considered in the topical treatment of generalized crusted (Norwegian) scabies. First, crusting diminishes the penetration of medication into burrows. Second, crusting may alter systemic absorption of scabicides because of changes in normal skin integrity.
Topical Agents
Although effectiveness is reduced, 5 percent permethrin cream may be used safely in patients with crusted scabies. Keratolytics aid treatment by improving the penetration of permethrin into burrows.
Ivermectin
Oral ivermectin is a new and promising treatment for crusted scabies. Because of its effectiveness and convenience, ivermectin is becoming the agent of choice in crusted scabies treatment, community eradication programs, and general scabies therapy. Studies have demonstrated its safety and efficacy.18,19 In one study,20 a single dose of this agent (200 mcg per kg) eradicated scabies in 70 percent of patients; optimal dosage and timing of the second dose vary.21
Ivermectin is not labeled for the treatment of scabies. Although infants elsewhere in the world reportedly are treated with ivermectin, the FDA has not labeled this drug for use in children weighing less than 15 kg (33 lb). Ivermectin is a pregnancy category C drug. It is excreted in low concentrations in breast milk. In third-world countries, it has been used to treat onchocerciasis in pregnant and nursing women, with no teratogenic effects observed.20
In pregnant or lactating women and in newborns, 5 or 10 percent precipitated sulfur in petrolatum is a safe, effective treatment for generalized crusted scabies. Treatment is as described for classic scabies.
