Annular lesions can present in a variety of diseases. Knowledge of the physical appearance and history of presentation of these skin findings can help in the diagnosis. A pruritic, annular, erythematous patch that grows centrifugally should prompt evaluation for tinea corporis. Tinea corporis may be diagnosed through potassium hydroxide examination of scrapings. Recognizing erythema migrans is important in making the diagnosis of Lyme disease so that antibiotics can be initiated promptly. Plaque psoriasis generally presents with sharply demarcated, erythematous silver plaques. Erythema multiforme, which is due to a hypersensitivity reaction, presents with annular, raised lesions with central clearing. Lichen planus characteristically appears as planar, purple, polygonal, pruritic papules and plaques. Nummular eczema presents as a rash composed of coin-shaped papulovesicular erythematous lesions. Treatment is aimed at reducing skin dryness. Pityriasis rosea presents with multiple erythematous lesions with raised, scaly borders, and is generally self-limited. Urticaria results from the release of histamines and appears as well-circumscribed, erythematous lesions with raised borders and blanched centers. Annular lesions occur less commonly in persons with fixed drug eruptions, leprosy, immunoglobulin A vasculitis, secondary syphilis, sarcoidosis, subacute cutaneous lupus erythematosus, and granuloma annulare.
The word annular is derived from the Latin word annulus, meaning ringed. Many diseases present with cutaneous annular lesions, making distinction by physical appearance alone challenging. This review highlights the physical appearance of and historical findings associated with these lesions, which can aid in diagnosing common and uncommon diseases (Table 1). The management of conditions that cause annular lesions is also discussed.
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendation | Evidence rating | References |
|---|---|---|
| A potassium hydroxide preparation of peripheral scale is a reliable test to confirm the diagnosis of tinea corporis. | C | 1 |
| Skin hydration with emollients should be included in the basic therapy for nummular eczema. | C | 19, 20 |
| Lesions consistent with pityriasis rosea that do not resolve spontaneously in three months should be considered for biopsy. | C | 28–30 |
| In patients with acute immunoglobulin A vasculitis, the administration of systemic corticosteroids reduces joint and abdominal pain but does not reduce the risk of nephritis. | A | 38–40 |
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.
TABLE 1 Diseases That Can Cause Annular Lesions
| Common annular lesions | Uncommon annular lesions |
|---|---|
|
|
Common Diseases That May Present with Annular Lesions
Table 2 describes clinical presentations, diagnostic tests, and treatment options for skin lesions associated with common diseases.
TABLE 2 Common Diseases That May Present with Annular Lesions
| Condition | Description | Clinical presentation | Diagnosis and management |
|---|---|---|---|
| Tinea corporis | Scaly, erythematous annular plaques with raised borders that spread centrifugally | Lesions develop after close contact with infected persons, animals, or soil; warm, moist environments exacerbate lesions | Potassium hydroxide preparation may detect segmented hyphae |
| Treatment options include topical and systemic antifungals | |||
| Erythema migrans (Lyme disease) | Expanding, erythematous, annular rash with or without central clearing | Lesion appears three to 30 days after tick bite, often preceded by an influenza-like prodrome of fever, malaise, and myalgias | Diagnosis is clinical |
| Treatment options include doxycycline, amoxicillin, cefuroxime (Ceftin), and ceftriaxone (Rocephin) | |||
| Plaque psoriasis | Well-demarcated, erythematous, annular plaques with adherent silvery scales | Pruritic lesions often associated with stress, alcohol, or friction | Diagnosis is clinical |
| Treatment options include topical steroids and vitamin D analogues for mild cases; and systemic corticosteroids, phototherapy, and biologic agents for severe cases | |||
| Erythema multiforme | Multiple raised, annular, target-like lesions with central erythema | Lesions develop over a few days and usually resolve within three to five weeks without treatment; 90% of cases are associated with herpes simplex virus type 1, and 10% of cases are associated with medications or vaccinations | Diagnosis is clinical |
| Treatment options include antivirals and systemic corticosteroids for recurrent symptoms | |||
| Lichen planus | Violaceous, flat-topped papules with fine white or gray reticular, lacy lines on top of the rash | Pruritic rash that bleeds with trauma; most commonly involves the ankles and volar surfaces of the wrist; lesions can be intraoral; associated with certain drugs and hepatitis C infection | Diagnosis is clinical, but biopsy can confirm |
| Treatment options include topical corticosteroids, systemic glucocorticoids, and ultraviolet A or B phototherapy | |||
| Nummular eczema | Coin-shaped, erythematous, scaly, annular lesions | Intensely pruritic; most commonly involves the extremities | Diagnosis is clinical; potassium hydroxide preparation can rule out tinea corporis |
| Treatment includes minimizing skin dryness and reducing exposure to skin irritants; topical corticosteroids for mild symptoms; and ultraviolet B phototherapy and systemic corticosteroids for severe symptoms | |||
| Pityriasis rosea | Salmon-colored, demarcated, annular or ovoid lesions with scaly borders slanted backward | Usually asymptomatic; more common in females; follows skin cleavage lines | Diagnosis is clinical |
| Treatment options include topical corticosteroids, oral antihistamines, and ultraviolet A or B phototherapy; systemic corticosteroids may be used for severe symptoms | |||
| Urticaria | Pruritic, red, edematous plaques | Intensely pruritic; may affect any area of the body; usually lasts 90 minutes to 24 hours | Diagnosis is clinical |
| Empiric treatment options include antihistamines and corticosteroids |
TINEA CORPORIS
Tinea corporis is a dermatophyte infection that can occur on any cutaneous surface other than the hands, feet, scalp, or groin. Tinea presents as a pruritic, annular, erythematous patch or plaque that grows centrifugally (Figure 1). As the rash spreads outward, central clearing typically develops. The characteristic physical appearance may be sufficient to make the diagnosis; however, a potassium hydroxide preparation of the scaly edge of the lesion can confirm the diagnosis by demonstrating segmented hyphae on microscopic examination.1 First-line treatments include topical imidazoles (clotrimazole and miconazole) and allylamines (terbinafine [Lamisil], butenafine [Lotrimin], and naftifine [Naftin]). Oral terbinafine, griseofulvin, or itraconazole (Sporanox) may be considered for infections that cover significant areas on the body. In patients with extensive fungal infections, tests should be ordered for immunocompromising conditions, such as diabetes mellitus and human immunodeficiency virus infection.2,3 Because treatment with corticosteroids can exacerbate tinea corporis, the diagnosis should be reconsidered in patients with annular lesions that worsen when treated with these medications.1
FIGURE 1

Tinea corporis. The ovoid appearance of this lesion is caused by variable rates of extension of the scaly border.
Copyright © Thomas Jefferson University.
ERYTHEMA MIGRANS
Erythema migrans, the characteristic rash of Lyme disease, is caused by the spirochete Borrelia burgdorferi, which is transmitted by a bite from a deer tick (Ixodes scapularis or pacificus).4 There are three clinically recognized stages of Lyme disease: early localized, early disseminated, and late. The early localized stage presents three to 30 days after the tick bite and is characterized by erythema migrans.5 The rash is annular and erythematous, and may or may not have central clearing (Figure 2). The classically described bull'seye appearance occurs in only 9% of cases.6,7
FIGURE 2

Erythema migrans. Slowly expanding bull's-eye lesion with central clearing.
Copyright © Thomas Jefferson University.
The diagnosis of Lyme disease is based on the appearance of erythema migrans and recent exposure to ticks. Treatment should be initiated promptly to avoid progression of the disease and involvement of extracutaneous organ systems (cardiac, musculoskeletal, and neurologic). Doxycycline, amoxicillin, and cefuroxime (Ceftin) are equally effective for the treatment of early localized erythema migrans. Ceftriaxone (Rocephin) should be reserved for patients with neurologic or cardiac involvement.8 Additional information on the diagnosis and management of Lyme disease is available in a previous American Family Physician article.9
PLAQUE PSORIASIS
Psoriasis is a chronic inflammatory skin condition with a genetic predisposition. Plaque and pustular psoriasis are the only two forms that can present with annular lesions. The lesions of plaque psoriasis are pruritic, sharply demarcated, erythematous, and round or ovoid, with silver plaques that bleed easily with trauma 10 (Auspitz sign; Figure 3). Topical corticosteroids are sufficient for treatment of mild disease (covering less than 5% of the body surface). For more severe disease, ultraviolet A or B (UVA or UVB) phototherapy, systemic treatment with methotrexate and cyclosporine (Sandimmune), and biologic agents should be considered.11 Systemic corticosteroids are usually not recommended because of the risk of symptom flare-ups when the medications are discontinued. Additional information on the diagnosis and management of psoriasis is available in a previous American Family Physician article.12
FIGURE 3

Plaque psoriasis. Sharply demarcated, silver-scaled plaques on the knees.
Copyright © Thomas Jefferson University.
ERYTHEMA MULTIFORME
Erythema multiforme is a skin condition that is thought to be a hypersensitivity reaction to infections or drugs. The classic lesions are annular and raised, and have central erythema described as target-like (Figure 4). The lesions develop over a few days and usually resolve within three to five weeks.13 Erythema multiforme is often associated with herpes simplex virus and Mycoplasma pneumoniae infections, medications, and vaccinations; however, no cause is identified in up to 50% of cases.13–15 Treatment is aimed at managing the infection or stopping the causative medication. Oral antihistamines and topical corticosteroids can alleviate symptoms. Continuous acyclovir is the preferred treatment for recurrent symptoms caused by herpes simplex virus infection.13
FIGURE 4

Erythema multiforme. Raised, polycyclic, target-like lesions.
Copyright © Thomas Jefferson University.
LICHEN PLANUS
Lichen planus is a chronic, inflammatory, autoimmune condition that is classically described using the six P's: planar, purple, polygonal, pruritic, papules, and plaques (Figure 5). These lesions may be covered with white, lacy, reticular lines known as Wickham striae. Lesions often appear on the ankles and volar surfaces of the wrists, but they can also appear on oral mucosa. Lichen planus is associated with hepatitis C infection and certain drugs.16 The diagnosis is based on clinical assessment, but biopsy can be performed for confirmation. Treatment options include topical or systemic corticosteroids, as well as UVA and UVB phototherapy.17
FIGURE 5

Lichen planus. Violaceous, flat-topped, shiny plaques.
Copyright © Thomas Jefferson University.
NUMMULAR ECZEMA
Nummular eczema presents as a rash with coin-shaped, scaly, pruritic, erythematous lesions (Figure 6). The rash commonly develops during cold, dry months and is often associated with atopic dermatitis and asthma. It usually presents on the extensor surfaces of the hands, arms, and legs.18 Diagnosis is based on clinical presentation. Nummular eczema is often mistaken for tinea corporis, and a potassium hydroxide preparation of skin scrapings may help distinguish between the conditions. Treatment is aimed at reducing skin dryness and minimizing exposure to irritants. Topical corticosteroids may be used for mild symptoms.19 UVA and UVB phototherapy and systemic corticosteroids are reserved for severe symptoms.20
FIGURE 6

Nummular eczema. Scaly, pruritic lesions with poorly demarcated borders.
Copyright © Thomas Jefferson University.
PITYRIASIS ROSEA
Pityriasis rosea may first present as a herald patch: a single erythematous lesion with raised, scaly borders (Figure 7). Within two weeks, diffuse cutaneous involvement occurs with the eruption of multiple, round or ovoid, collarette lesions with scaly borders.2 The rash most commonly presents on the trunk and follows skin folds in a “Christmas tree” distribution.21 An influenza-like prodrome precedes the rash in 5% of patients.22 Workup should include a rapid plasma reagin test to exclude syphilis, especially if the rash is present on the palms and soles in sexually active patients. Pityriasis rosea is self-limited and usually resolves within six to eight weeks. Topical corticosteroids and oral antihistamines can be used to alleviate pruritus. There is some evidence that acyclovir and phototherapy may be effective.23–27 Lesions that last longer than three months warrant a biopsy to rule out alternative diagnoses.28–30
FIGURE 7

Pityriasis rosea. Classic herald patch demonstrating central clearing.
Copyright © Thomas Jefferson University.
URTICARIA
Urticaria is a condition that develops in response to the release of histamines, resulting in increased vascular permeability and massive edema in the superficial dermis. The edema creates well-circumscribed, ery thematous lesions with raised borders and blanched centers (Figure 8). Urticarial lesions are precipitated by three types of events: allergic, physical, or idiopathic. The diagnosis is based on clinical appearance.2 Urticaria is classified as acute if it lasts less than six weeks, or chronic if present for more than six weeks. Treatment consists of avoiding triggers; for symptomatic relief, histamine blockers may provide some benefit.31 If individual lesions last longer than 24 hours, biopsy should be considered to rule out leukocytoclastic vasculitis, which can mimic urticaria.2
FIGURE 8

Urticaria. Multiple raised, erythematous, round lesions.
Copyright © Thomas Jefferson University.
Uncommon Diseases That May Present with Annular Lesions
FIXED DRUG ERUPTION
The rash caused by a fixed drug eruption is characterized by groups of erythematous or violaceous patches or plaques (Figure 9). The rash develops 30 minutes to eight hours after ingestion of the drug. Sulfa drugs and nonsteroidal anti-inflammatory drugs are the most common causative agents. First-generation antihistamines and topical corticosteroids may provide temporary symptomatic relief. Resolution occurs within seven to 10 days of stopping the causative drug; however, postinflammatory hyperpigmentation may persist.32
FIGURE 9

Fixed drug eruption. Violaceous, annular patches with areas of hyperpigmentation.
Copyright © Thomas Jefferson University.
LEPROSY
Leprosy, also called Hansen disease, is caused by the bacteria Mycobacterium leprae. It is rare in the United States; most cases occur in patients who have lived in foreign countries. The skin lesions present as erythematous annular plaques with or without scales (Figure 10). The lesions may appear hypopigmented in dark-skinned persons. Patients may have decreased sensation to pain, temperature, and touch over the lesions. The preferred method of diagnosis is polymerase chain reaction testing or Fite-Faraco staining of a biopsy of the lesions.33 Treatment involves multidrug therapy with dapsone, rifampin, and clofazimine.34
FIGURE 10

Leprosy. Erythematous annular plaques with scales.
Image used with permission from VisualDx.
IMMUNOGLOBULIN A VASCULITIS
Immunoglobulin A (IgA) vasculitis, also called Henoch-Schönlein purpura,35 is the most common vasculitis in children. The rash presents as violaceous ecchymoses, petechiae, and palpable purpura (Figure 11). The diagnosis can be made clinically based on the presentation of skin lesions with arthritic symptoms and colicky abdominal pain. If clinical findings are inconclusive, a complete blood count, urinalysis, IgA levels, and skin and kidney biopsies should be ordered. Diagnostic biopsies will show prominent IgA deposition.36 The disease typically resolves in four to six weeks.37
FIGURE 11

Immunoglobulin A vasculitis. Violaceous, palpable purpuric lesions.
Copyright © Thomas Jefferson University.
Treatment involves pain management with nonsteroidal anti-inflammatory drugs or acetaminophen. Systemic corticosteroids can minimize the severity of joint and abdominal pain.38 However, a 2015 Cochrane review did not support the use of corticosteroids for the prevention of nephritic disease.39 A recent randomized controlled trial found no significant difference in proteinuria at 12 months after the onset of IgA vasculitis in children who received prednisolone for 14 days compared with those who received placebo.40
SECONDARY SYPHILIS
The rash of secondary syphilis is diffuse, symmetric, erythematous, and annulopapular (Figure 12). It typically involves the trunk, extremities, palms, and soles, and may be accompanied by an influenza-like prodrome. The diagnosis is made by rapid plasma reagin testing confirmed by treponemal testing. The preferred treatment is parenteral penicillin G benzathine.41 Proper treatment is essential because disease progression results in severe cardiac and neurologic complications. New cases of secondary syphilis must be reported to the Centers for Disease Control and Prevention.41
FIGURE 12

Secondary syphilis. Hyperpigmented round lesions on palms.
Image used with permission from VisualDx.
SARCOIDOSIS
The rash of sarcoidosis is characterized by erythematous, indurated plaques (Figure 13).2 The multisystem disease involves formation of noncaseating granulomas in almost every organ system, including the skin, lungs, spleen, eyes, salivary glands, and lymph nodes. It is more common in black patients 10 to 39 years of age. The recommended workup for sarcoidosis includes skin biopsy, chest radiography or high-resolution computed tomography, tuberculosis skin testing, pulmonary function testing, and ophthalmologic examination to assess for uveitis.42,43
FIGURE 13

Sarcoidosis. Erythematous, indurated plaque.
Reprinted with permission from Hsu S, Le EH, Khoshevis MR. Differential diagnosis of annular lesions. Am Fam Physician. 2001;64(2):293.
There is no cure for sarcoidosis; treatment is aimed at alleviating symptoms. First-line therapies include topical and systemic corticosteroids. Hydroxychloroquine (Plaquenil), chloroquine (Aralen), methotrexate, and thalidomide are alternatives for patients who cannot tolerate corticosteroids or whose symptoms do not respond to initial treatment.2,44 Additional information on the diagnosis and management of sarcoidosis is available in a previous American Family Physician article.45
SUBACUTE CUTANEOUS LUPUS ERYTHEMATOSUS
Subacute cutaneous lupus erythematosus most commonly develops in women 20 to 39 years of age. Skin lesions develop in sun-exposed areas of the body (Figure 14).46 Laboratory testing for autoimmune antibodies will often be positive for antinuclear and anti–Sjögren-A antibodies and negative for anti–double-stranded DNA antibodies. Treatment begins with minimizing sun exposure through the use of sunscreen. Topical corticosteroids may also be used; systemic corticosteroids, hydroxychloroquine, dapsone, thalidomide, methotrexate, and retinoids may benefit patients with more severe disease.47,48
FIGURE 14

Subacute cutaneous lupus erythematosus. Red, annular lesions with some atrophy and minimal scaling.
Reprinted with permission from Lam NC, Ghetu MV, Bieniek ML. Systemic lupus erythematosus: primary care approach to diagnosis and management. Am Fam Physician. 2016;94(4):289.
GRANULOMA ANNULARE
Granuloma annulare is characterized by firm, shiny papules that can be violaceous, erythematous, or brown or flesh-colored with central involution (Figure 15). The lesions most commonly develop on the dorsal side of the hands and feet. Granuloma annulare can be associated with type 1 diabetes, dyslipidemia, and some malignancies. Isotretinoin and dapsone may be used to treat widespread disease; however, evidence of their effectiveness is limited by a lack of clinical trials. These agents pose a significant risk of toxicity and have numerous adverse effects. Granuloma annulare lesions usually resolve spontaneously within two years.49,50
FIGURE 15
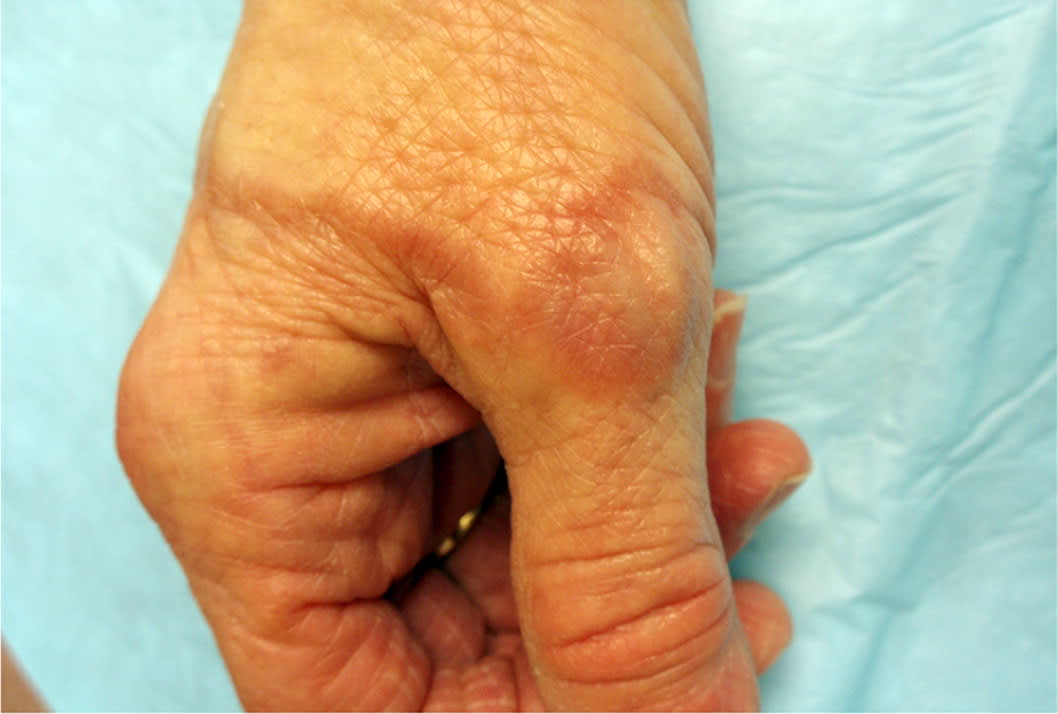
Granuloma annulare. Brownish-red lesion on the dorsal wrist with a ringed lesion extending around the hand.
Copyright © Thomas Jefferson University.
This article updates a previous article on this topic by Hsu, et al.2
Data Sources: A PubMed search was completed in Clinical Queries using the terms annular lesions, tinea corporis, Lyme, plaque psoriasis, erythema multiforme, lichen planus, nummular eczema, pityriasis rosea, herpes simplex virus type 1, and urticaria. The search included meta-analyses, systematic reviews, clinical trials, and reviews. Also searched were the Cochrane Database of Systematic Reviews, U.S. Preventive Services Task Force website, DynaMed, Essential Evidence Plus, and UpToDate. The American Academy of Family Physicians website (https://www.aafp.org/) was also searched using the term annular lesions. Search dates: May, August, and September 2017, and July 2018.
