Persons whose experienced or expressed gender differs from their sex assigned at birth may identify as transgender. Transgender and gender-diverse persons may have gender dysphoria (i.e., distress related to this incongruence) and often face substantial health care disparities and barriers to care. Gender identity is distinct from sexual orientation, sex development, and external gender expression. Each construct is culturally variable and exists along continuums rather than as dichotomous entities. Training staff in culturally sensitive terminology and transgender topics (e.g., use of chosen name and pronouns), creating welcoming and affirming clinical environments, and assessing personal biases may facilitate improved patient interactions. Depending on their comfort level and the availability of local subspecialty support, primary care clinicians may evaluate gender dysphoria and manage applicable hormone therapy, or monitor well-being and provide primary care and referrals. The history and physical examination should be sensitive and tailored to the reason for each visit. Clinicians should identify and treat mental health conditions but avoid the assumption that such conditions are related to gender identity. Preventive services should be based on the patient's current anatomy, medication use, and behaviors. Gender-affirming hormone therapy, which involves the use of an estrogen and antiandrogen, or of testosterone, is generally safe but partially irreversible. Specialized referral-based surgical services may improve outcomes in select patients. Adolescents experiencing puberty should be evaluated for reversible puberty suppression, which may make future affirmation easier and safer. Aspects of affirming care should not be delayed until gender stability is ensured. Multidisciplinary care may be optimal but is not universally available.
In the United States, approximately 150,000 youth and 1.4 million adults identify as transgender.1,2 As sociocultural acceptance patterns evolve, clinicians will likely care for an increasing number of transgender persons.3 However, data from a large observational study suggests that 24% of transgender persons report unequal treatment in health care environments, 19% report refusal of care altogether, and 33% do not seek preventive services.4 Approximately one-half report that they have taught basic tenets of transgender care to their health care professional.4
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendation | Evidence rating | References |
|---|---|---|
| Training clinicians and staff in culturally sensitive terminology and transgender topics, as well as cultural humility and assessment of personal internal biases, may facilitate improved patient interactions. | C | 5, 12, 14, 15, 21, 24 |
| Clinicians should consider routine screening for depression, anxiety, posttraumatic stress disorder, eating disorders, substance use, intimate partner violence, self-injury, bullying, truancy, homelessness, high-risk sexual behaviors, and suicidality. However, it is important to avoid assumptions that any concerns are secondary to being transgender. | C | 5, 11, 12, 14, 15, 19, 21, 26–29 |
| Efforts to convert a person's gender identity to align with their sex assigned at birth are unethical and incompatible with current guidelines and evidence. | C | 6, 8, 11, 12, 14, 15, 17, 21, 31 |
| Not all transgender or gender-diverse persons require or seek hormone therapy. However, those who receive treatment generally report improved quality of life, self-esteem, and anxiety. | B | 5, 6, 39–44 |
| Clinicians should consider initiation of or timely referral for a gonadotropin-releasing hormone analogue to suppress puberty when the patient has reached stage 2 or 3 of sexual maturity. No hormonal intervention is warranted before the onset of puberty. | C | 5, 6, 8, 17, 21, 40, 44 |
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.
eTable A provides definitions of terms used in this article. Transgender describes persons whose experienced or expressed gender differs from their sex assigned at birth.5,6 Gender dysphoria describes distress or problems functioning that may be experienced by transgender and gender-diverse persons; this term should be used to describe distressing symptoms rather than to pathologize.7,8 Gender incongruence, a diagnosis in the International Classification of Diseases, 11th revision (ICD-11),9 describes the discrepancy between a person's experienced gender and assigned sex but does not imply dysphoria or a preference for treatment.10 The terms transgender and gender incongruence generally are not used to describe sexual orientation, sex development, or external gender expression, which are related but distinct phenomena.5,7,8,11 It may be helpful to consider the above constructs as culturally variable, nonbinary, and existing along continuums rather than as dichotomous entities.5,8,12,13 For clarity, the term transgender will be used as an umbrella term in this article to indicate gender incongruence, dysphoria, or diversity.
eTABLE A Gender-Related Terminology
| Term | Definition |
|---|---|
| Affirmed gender | When one's gender identity is validated by others as authentic |
| Agender | Person who identifies as genderless or outside the gender continuum |
| Cisgender | Not transgender; a person whose gender identity and/or expression aligns with their sex assigned at birth |
| Cross dressing | Wearing of clothes typically associated with another gender; the term transvestite can be considered pejorative and should not be used |
| Cultural humility | Concept of not projecting one's own personal experiences and preconceptions of identity onto the experiences and identities of others |
| Differences of sex development | Congenital conditions characterized by nuanced chromosomal, gonadal, or anatomic sex development (e.g., congenital adrenal hyperplasia, androgen insensitivity syndrome, Turner syndrome); not a universally accepted term; also called disorders of sex development or intersex |
| Gender | Societal perception of maleness or femaleness |
| Genderqueer | Umbrella term for a broad range of identities along or outside the gender continuum; also called gender nonbinary |
| Gender diverse* | General term describing gender behaviors, expressions, or identities that are not congruent with those culturally assigned at birth; may include transgender, nonbinary, genderqueer, gender fluid, or non-cisgender identitites and may be more dynamic and less stigmatizing than prior terminology (e.g., gender nonconforming); this term is not used as a clinical diagnosisA1 |
| Gender dysphoria | Distress or impairment resulting from incongruence between one's experienced or expressed gender and sex assigned at birth; DSM-5 criteria for adults include at least six months of distress or problems functioning due to at least two of the following:
|
| Gender expression | External display of gender identity through appearance (e.g., clothing, hairstyle), behavior, voice, or interests |
| Gender identity | Internalized sense of self as being male, female, or elsewhere along or outside the gender continuum; some persons have complex identities and may identify as agender, gender nonbinary, genderqueer, or gender fluid |
| Gender identity disorder | Diagnosis related to gender dysphoria or gender incongruence in earlier versions of the DSM and ICD |
| Gender incongruence* | General term describing a difference between gender identity and/or expression and designated sex; an ICD-11 diagnosis that does not require a mental health diagnosis |
| Sex | Maleness or femaleness as it relates to sex chromosomes, gonads, genitalia, secondary sex characteristics, and relative levels of sex hormones; these biologic determinants may not necessarily be consistent; sex assigned at birth is typically based on genital anatomy |
| Sexual orientation | Term describing an enduring physical and emotional attraction to another group; sexual orientation is distinct from gender identity and is defined by the individual |
| They/them | Neutral pronouns preferred by some transgender persons |
Transgender*
| General term used to describe persons whose gender identity or expression differs from their sex assigned at birth A transgender person designated as male at birth A transgender person designated as female at birth |
| Transfeminine | Nonbinary term used to describe a feminine spectrum of gender identity |
| Transmasculine | Nonbinary term used to describe a masculine spectrum of gender identity |
| Transphobia | Prejudicial attitudes about persons who are not cisgender |
| Transsexual | Historical term for transgender persons seeking medical or surgial therapy to affirm their gender |
DSM = Diagnostic and Statistical Manual of Mental Disorders; ICD = International Classification of Diseases.
*—The terms gender diverse, gender incongruence, and transgender do not necessarily imply gender dysphoria.
Information from:
A1. Rafferty J; Committee on Psychosocial Aspects of Child and Family Health; Committee on Adolescence; Section on Lesbian, Gay, Bisexual, and Transgender Health and Wellness. Ensuring comprehensive care and support for transgender and gender-diverse children and adolescents. Pediatrics. 2018;142(4):e20182162.
Adelson SL; American Academy of Child and Adolescent Psychiatry (AACAP) Committee on Quality Issues (CQI). Practice parameter on gay, lesbian, or bisexual sexual orientation, gender nonconformity, and gender discordance in children and adolescents. J Am Acad Child Adolesc Psychiatry. 2012;51(9):957–974.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Association; 2013.
American Psychological Association. Guidelines for psychological practice with transgender and gender nonconforming people. Am Psychol. 2015;70(9):832–864.
Coleman E, Bockting W, Botzer M, et al. Standards of care for the health of transsexual, transgender, and gender-nonconforming people, version 7. Int J Transgenderism. 2012;13(4):165–232.
de Vries AL, Klink D, Cohen-Kettenis PT. What the primary care pediatrician needs to know about gender incongruence and gender dysphoria in children and adolescents. Pediatr Clin North Am. 2016;63(6):1121–1135.
Deutsch MB. Guidelines for the primary and gender-affirming care of transgender and gender nonbinary people. 2nd ed. June 17, 2016. http://transhealth.ucsf.edu/protocols. Accessed July 5, 2018.
Hembree WC, Cohen-Kettenis PT, Gooren L, et al. Endocrine treatment of gender-dysphoric/gender-incongruent persons: an Endocrine Society clinical practice guideline [published correction appears in J Clin Endocrinol Metab. 2018;103(2):699]. J Clin Endocrinol Metab. 2017;102(11):3869–3903.
Lee PA, Nordenström A, Houk CP, et al.; Global DSD Update Consortium. Global disorders of sex development update since 2006: perceptions, approach and care [published correction appears in Horm Res Paediatr. 2016;85(3):180]. Horm Res Paediatr. 2016;85(3):158–180.
Levine DA; Committee on Adolescence. Office-based care for lesbian, gay, bisexual, transgender, and questioning youth. Pediatrics. 2013;132(1):e297–e313.
Reed GM, Drescher J, Krueger RB, et al. Disorders related to sexuality and gender identity in the ICD-11: revising the ICD-10 classification based on current scientific evidence, best clinical practices, and human rights considerations [published correction appears in World Psychiatry. 2017;16(2):220]. World Psychiatry. 2016;15(3):205–221.
Winter S, Diamond M, Green J, et al. Transgender people: health at the margins of society. Lancet. 2016;388(10042):390–400.
Optimal Clinical Environment
It is important for clinicians to establish a safe and welcoming environment for transgender patients, with an emphasis on establishing and maintaining rapport (Table 1).5,6,8,11,12,14–21 Clinicians can tell patients, “Although I have limited experience caring for gender-diverse persons, it is important to me that you feel safe in my practice, and I will work hard to give you the best care possible.”22 Waiting areas may be more welcoming if transgender-friendly materials and displayed graphics show diversity.5,12,14,15 Intake forms can be updated to include gender-neutral language and to use the two-step method (two questions to identify chosen gender identity and sex assigned at birth) to help identify transgender patients.5,16,23 Training clinicians and staff in culturally sensitive terminology and transgender topics, as well as cultural humility and assessment of personal internal biases, may facilitate improved patient interactions.5,21,24 Clinicians may also consider advocating for transgender patients in their community.12,14,15,21
TABLE 1. Transgender-Friendly Concepts for Clinicians
| Goal | Actions |
|---|---|
| Advocate for the patient in the community | Foster sources of social support, including the patient's family and/or community, if allowed by the patient |
| If you are unable to provide care for transgender patients, refer them to clinicians who are comfortable doing so | |
| Provide patients with information on transgender-friendly community resources | |
| Approach the patient with sensitivity and awareness | Avoid imposing a binary view of gender identity, sexual orientation, sex development, or gender expression |
| Be aware that interventions to change gender identity are unethical | |
| Build rapport and trust by providing nonjudgmental care | |
| Examine how aspects of one's identity (e.g., gender, sexual orientation, race, ethnicity, class, disability, spirituality) intersect in creating one's experience, and how coping strategies are influenced by marginalization experiences | |
| Treat all patients with empathy, respect, and dignity | |
| Create a transgender-friendly clinical environment | Adopt and disseminate a nondiscrimination policy |
| Ask staff to perform a personal assessment of internal biases | |
| Consider including the two-step method (two questions to identify chosen gender identity and sex assigned at birth) to collect gender identity data | |
| Ensure that intake forms and records use gender-neutral or inclusive language (e.g., partnered instead of married) | |
| Provide care that affirms the patient's gender identity | |
| Provide inclusive physical spaces (e.g., display brochures with photos of same-sex couples, designate at least one gender-neutral restroom, display LGBT-friendly flags) | |
Use gender-inclusive language, such as:
| |
| Maintain open communication with the promise of confidentiality | Do not assume patients are ready to disclose their gender identity to family members |
| Establish openness to discuss sexual and reproductive health concerns | |
| Inquire about unfamiliar terminology to prevent miscommunication | |
| Minimize threats to confidentiality (e.g., at the pharmacy, through billing practices) | |
| Provide culturally sensitive adolescent care | Be aware of state-specific minor consent and confidentiality laws |
| Ensure timely referral for puberty suppression and mental health services | |
| Obtain an age-appropriate and confidential psychosocial history |
LGBT = lesbian, gay, bisexual, transgender.
Evaluation
MEDICAL HISTORY
When assessing transgender patients for gender-affirming care, the clinician should evaluate the magnitude, duration, and stability of any gender dysphoria or incongruence.8,12 Treatment should be optimized for conditions that may confound the clinical picture (e.g., psychosis) or make gender-affirming care more difficult (e.g., uncontrolled depression, significant substance use).6,11,17 The support and safety of the patient's social environment also warrants evaluation as it pertains to gender affirmation.6,8,11 This is ideally accomplished with multidisciplinary care and may require several visits to fully evaluate.5,6,8,17 Depending on their comfort level and the availability of local subspecialty support, primary care clinicians may elect to take an active role in the patient's gender-related care by evaluating gender dysphoria and managing hormone therapy, or an adjunctive role by monitoring well-being and providing primary care and referrals (Figure 1).5,6,8,11–15,17,19,21,22
FIGURE 1.
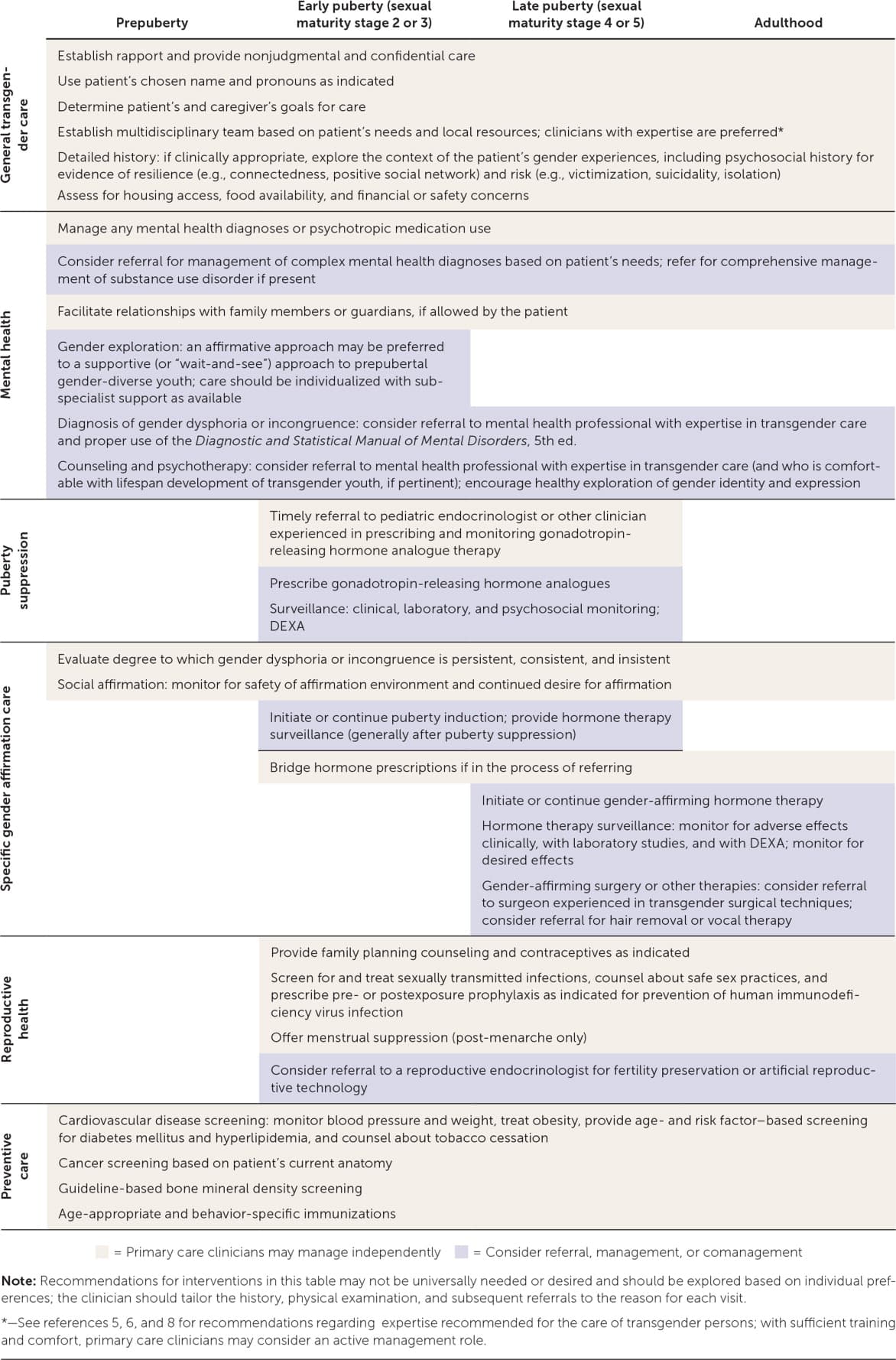
Considerations in the care of transgender and gender-diverse persons in primary care.
DEXA = dual-energy x-ray absorptiometry.
Information from references 5, 6, 8, 11 through 15, 17, 19, 21, and 22.
Clinicians should not consider themselves gatekeepers of hormone therapy; rather, they should assist patients in making reasonable and educated decisions about their health care using an informed consent model with parental consent as indicated.5,17 Based on expert opinion, the Endocrine Society recommends that clinicians who diagnose gender dysphoria or incongruence and who manage gender-affirming hormone therapy receive training in the proper use of the Diagnostic and Statistical Manual of Mental Disorders, 5th ed., and the ICD; have the ability to determine capacity for consent and to resolve psychosocial barriers to gender affirmation; be comfortable and knowledgeable in prescribing and monitoring hormone therapies; attend relevant professional meetings; and, if applicable, be familiar with lifespan development of transgender youth.6
PHYSICAL EXAMINATION
Transgender patients may experience discomfort during the physical examination because of ongoing dysphoria or negative past experiences.4,5,8 Examinations should be based on the patient's current anatomy and specific needs for the visit, and should be explained, chaperoned, and stopped as indicated by the patient's comfort level.5 Differences of sex development are typically diagnosed much earlier than gender dysphoria or gender incongruence. However, in the absence of gender-affirming hormone therapy, an initial examination may be warranted to assess for sex characteristics that are incongruent with sex assigned at birth. Such findings may warrant referral to an endocrinologist or other subspecialist.6,25
Mental Health
Transgender patients typically have high rates of mental health diagnoses.11,18 However, it is important not to assume that a patient's mental health concerns are secondary to being transgender.5,12,15 Primary care clinicians should consider routine screening for depression, anxiety, posttraumatic stress disorder, eating disorders, substance use, intimate partner violence, self-injury, bullying, truancy, homelessness, high-risk sexual behaviors, and suicidality.5,11,14,15,19,26–29 Clinicians should be equipped to handle the basic mental health needs of transgender persons (e.g., first-line treatments for depression or anxiety) and refer patients to subspecialists when warranted.5,8,15
Because of the higher prevalence of traumatic life experiences in transgender persons, care should be trauma-informed (i.e., focused on safety, empowerment, and trustworthiness) and guided by the patient's life experiences as they relate to their care and resilience.5,15,30 Efforts to convert a person's gender identity to align with their sex assigned at birth—so-called gender conversion therapy—are unethical and incompatible with current guidelines and evidence, including policy from the American Academy of Family Physicians.6,8,11,12,14,15,17,31
Health Maintenance
Preventive services are similar for transgender and cisgender (i.e., not transgender) persons. Nuanced recommendations are based on the patient's current anatomy, medication use, and behaviors.5,6,32 Screening recommendations for hyperlipidemia, diabetes mellitus, tobacco use, hypertension, and obesity are available from the U.S. Preventive Services Task Force (USPSTF).33 Clinicians should be vigilant for signs and symptoms of venous thromboembolism (VTE) and metabolic disease because hormone therapy may increase the risk of these conditions.5,6,34 Screening for osteoporosis is based on hormone use.6,35
Cancer screening recommendations are determined by the patient's current anatomy. Transgender females with breast tissue and transgender males who have not undergone complete mastectomy should receive screening mammography based on guidelines for cisgender persons.6,36 Screening for cervical and prostate cancers should be based on current guidelines and the presence of relevant anatomy.5,6
Recommendations for immunizations (e.g., human papillomavirus) and screening and treatment for sexually transmitted infections (including human immunodeficiency virus) are provided by the Centers for Disease Control and Prevention and USPSTF based on sexual practices.32,33,37,38 Pre- and postexposure prophylaxis for human immunodeficiency virus infection should be considered for patients who meet treatment criteria.32,38
Hormone Therapy
Feminizing and masculinizing hormone therapies are partially irreversible treatments to facilitate development of secondary sex characteristics of the experienced gender.6 Not all gender-diverse persons require or seek hormone treatment; however, those who receive treatment generally report improved quality of life, self-esteem, and anxiety.5,6,39–44 Patients must consent to therapy after being informed of the potentially irreversible changes in physical appearance, fertility potential, and social circumstances, as well as other potential benefits and risks.
Feminizing hormone therapy includes estrogen and antiandrogens to decrease the serum testosterone level below 50 ng per dL (1.7 nmol per L) while maintaining the serum estradiol level below 200 pg per mL (734 pmol per L).6 Therapy may reduce muscle mass, libido, and terminal hair growth, and increase breast development and fat redistribution; voice change is not expected.5,6 The risk of VTE can be mitigated by avoiding formulations containing ethinyl estradiol, supraphysiologic doses, and tobacco use.34,45–47 Additional risks include breast cancer, prolactinoma, cardiovascular or cerebrovascular disease, cholelithiasis, and hypertriglyceridemia; however, these risks are rare (yet clinically significant), indolent, or incompletely studied.5,6,36,48 Spironolactone use requires monitoring for hypotension, hyperkalemia, and changes in renal function.5,6
Masculinizing hormone therapy includes testosterone to increase serum levels to 320 to 1,000 ng per dL (11.1 to 34.7 nmol per L).6 Anticipated changes include acne, scalp hair loss, voice deepening, vaginal atrophy, clitoromegaly, weight gain, facial and body hair growth, and increased muscle mass. Patients receiving masculinizing hormone therapy are at risk of erythrocytosis, as determined by male-range reference values (e.g., hematocrit greater than 50%).5,6,45,49 Data on patient-oriented outcomes (e.g., death, thromboembolic disease, stroke, osteoporosis, liver toxicity, myocardial infarction) are sparse. Despite possible metabolic effects, few serious events have been identified in meta-analyses.6,34,35,45,46,49
Active hormone-sensitive malignancy is an absolute contraindication to gender-affirming hormone treatment.5 Patients who are older, use tobacco, or have severe chronic disease, current or previous VTE, or a history of hormone-sensitive malignancy may benefit from individualized dosing regimens and subspecialty consultation.5 The benefits and risks of treatment should be weighed against the risks of inaction, such as suicidality.5 The use of low-dose transdermal estradiol-17 β (Climara) may reduce the risk of VTE.5
Some patients without coexisting conditions may prefer a lower dose or individualized regimen.5 All patients should be offered referral to discuss fertility preservation or artificial reproductive technology.5,20 Table 25,6,17,22,50 and eTable B present surveillance guidelines and dosing recommendations for patients receiving gender-affirming hormone therapy.
TABLE 2. Monitoring of Patients Receiving Gender-Affirming Hormone Therapy
| Therapy and frequency | Surveillance |
|---|---|
| Puberty suppression (with a gonadotropin-releasing hormone analogue) | |
| Every visit | History: psychosocial assessment and treatment of high-risk findings; injection- or implant-site reaction and vasomotor symptoms; adherence to medication and mental health treatment plan, if applicable |
| 3 to 6 months | History: menstruation (if applicable) |
| Physical examination: height, weight, blood pressure, sexual maturity stage | |
| 6 to 12 months | Laboratory: serum luteinizing hormone, follicle-stimulating hormone, estradiol (in patients with ovaries) or testosterone (in patients with testes) levels by ultrasensitive assay, 25-hydroxyvitamin D level |
| 1 to 2 years | Imaging: bone mineral density testing until 25 to 30 years of age or until peak bone mass has been reached; bone age radiography of left hand if linear growth is concerning |
| Induction of puberty (with low doses of gender-affirming hormones after puberty suppression) | |
| Every visit | History: psychosocial assessment and treatment of high-risk findings; adherence to medication and mental health treatment plan, if applicable |
| 3 to 6 months | Physical examination: height, weight, blood pressure, sexual maturity stage |
| 6 to 12 months | Laboratory
|
| 1 to 2 years | Imaging: bone mineral density testing until 25 to 30 years of age or until peak bone mass has been reached |
| Feminizing hormone treatment | |
| Every visit | History: assessment for mental health conditions and treatment of high-risk findings (including suicidality); adherence to medication and mental health treatment plan, if applicable; tobacco cessation if indicated; adverse reactions to medications |
| 3 months (6 to 12 months after first year) | Laboratory: serum testosterone level (goal: < 50 ng per dL [1.7 nmol per L]) and estradiol level (goal: < 200 pg per mL [734 pmol per L]); electrolyte levels and renal function testing if spironolactone is used |
| Physical examination: blood pressure, weight, signs of feminization (per patient comfort) | |
| Periodic | Laboratory: serum prolactin level at baseline and every 1 to 2 years (alternative: only if symptomatic [e.g., visual symptoms, headaches, galactorrhea]); dyslipidemia and diabetes mellitus screening per established guidelines |
| Other testing: routine cancer screening based on current anatomy; osteoporosis screening beginning at 60 years of age (earlier if high risk or not adherent to estrogen regimen)* | |
| Masculinizing hormone treatment | |
| Every visit | History: assessment for mental health conditions and treatment of high-risk findings (including suicidality); adherence to medication and mental health treatment plan, if applicable; tobacco cessation if indicated; adverse reactions to medications |
| 3 months (6 to 12 months after first year) | Laboratory: serum testosterone level (goal: 400 to 700 ng per dL [13.9 to 24.3 nmol per L] at midpoint between injections) and hematocrit (goal: cisgender male range) |
| Physical examination: blood pressure, weight, signs of virilization (per patient comfort) | |
| Periodic | Laboratory: dyslipidemia and diabetes screening per established guidelines |
| Other testing: routine cancer screening (e.g., breast, cervical) based on current anatomy; osteoporosis screening in those who discontinue or are not adherent to testosterone regimen* | |
*—Serum luteinizing hormone and follicle-stimulating hormone levels may be monitored to optimize bone health in patients who have undergone gonadectomy and wish to reduce hormone doses.
Adapted with permission from Klein DA, Ellzy JA, Olson J. Care of a transgender adolescent. Am Fam Physician. 2015;92(2):146, with additional information from references 5, 6, 17, and 50.
eTABLE B Select Gender-Affirming Hormone Therapies for Transgender and Gender-Diverse Persons
| Therapy | Dosage | Estimated cost* | Adverse effects | Expected changes | Comments | ||
|---|---|---|---|---|---|---|---|
| Puberty suppression therapies | |||||||
| Histrelin (Supprelin LA) | 50-mg implant every 1 to 3 years based on clinical and laboratory findings | NA ($17,000), assuming 2 years of use per implant | Decreased acquisition of bone mineral density, emotional lability, injection- or implant-site reaction, transient vaginal bleeding, vasomotor symptoms, weight gain | Suppression of puberty development | Impairment of spermatogenesis and oocyte maturation occurs while receiving treatment; data on future fertility potential are limited. | ||
| Leuprolide (Lupron Depot-Ped 3-Month) | 11.25 mg intramuscularly every 3 months | NA ($33,500) | Acquisition of bone mineral density may normalize with future estrogen or testosterone treatment. | ||||
| Puberty induction therapies† | |||||||
| See 2017 Endocrine Society guidelineB1 | |||||||
| Feminizing hormone therapies‡ | |||||||
| Estrogens | |||||||
| Oral estradiol-17 β (Estrace) | 1 to 2 mg daily, titrated to maximum of 6 to 8 mg daily (divide total doses > 2 mg into two daily doses) | $50 to $150 ($1,900 to $9,000) | Migraines, emotional lability, thromboembolic disease, vasomotor symptoms, weight gain | Increased breast growth, fat redistribution, and soft, non-oily skin | Changes generally begin after 1 to 6 months of therapy, then stabilize after 1 to 3 years. | ||
| Transdermal estradiol-17 β (Climara) | 0.025- to 0.1-mg patch every 3 to 7 days (based on product), titrated to maximum of 0.2 to 0.4 mg | $400 to $650 ($1,600 to $3,000) | Rare, indolent, or incompletely studied: breast cancer, cardiovascular and cerebrovascular disease, cholelithiasis, hypertriglyceridemia, prolactinoma | Reduced muscle mass, strength, libido, sperm production, spontaneous erections, testicular volume, terminal hair growth | Avoid ethinyl estradiol because of unacceptable thromboembolic disease risk. Conjugated estrogens (e.g., Premarin) are not accurately measured in serum. Voice change is not expected; scalp hair change is unpredictable. | ||
| Adjunctive medications | |||||||
| Antiandrogen | Dose titration is based on clinical and laboratory findings. | ||||||
| Spironolactone (Aldactone) | 25 mg orally per day to 50 mg twice per day, titrated to maximum of 150 to 200 mg twice per day | $50 to $500 ($1,000 to $10,000) | Hyperkalemia, hypotension | Erectile dysfunction may be treated with a phosphodiesterase inhibitor. | |||
| Gonadotropin-releasing hormone analogue | See puberty suppression therapies above | See puberty suppression therapies above | |||||
| Masculinizing hormone therapies‡ | |||||||
| Parenteral testosterone enanthate or cypionate | 20 to 50 mg intramuscularly or subcutaneously weekly or every other week, titrated to a maximum of 100 mg per week (200 mg if given every other week) | $35 to $150 | Erythrocytosis, migraines, emotional lability, weight gain | Increased acne/oily skin, amenorrhea risk, clitoral size, facial and body hair, fat redistribution, muscle mass, strength, vaginal atrophy, voice deepening, scalp hair loss | Changes generally begin after 1 to 6 months of therapy, then stabilize after 1 to 3 years. | ||
| Transdermal testosterone 1% | 12.5 to 50 mg per day, titrated to a maximum of 100 mg per day | $700 to $3,650 | Rare, indolent, or incompletely studied: breast or uterine cancer, cardiovascular and cerebrovascular disease, hypertension, liver dysfunction | Dose titration is based on clinical and laboratory findings. | |||
| Menstruation suppression therapies/contraceptives | |||||||
| Combined oral contraceptives (continuous use of monophasic pills) | 20 to 35 mcg of ethinyl estradiol; progestin doses vary | $180 | Breakthrough bleeding, thromboembolic disease | Amenorrhea, oligomenorrhea | Progestin-only methods have minimal (if any) feminizing potential and may be ideal for transgender men who have started masculinizing therapy. | ||
| Depot medroxyprogesterone (Depo-Provera) | 150 mg intramuscularly every 3 months | $170 ($800) | Breakthrough bleeding, decreased bone mineral density, weight gain if overweight or obese | Gonadotropin-releasing hormone analogues alone may not provide adequate contraception effectiveness. | |||
| Levonorgestrel-releasing intrauterine system (Mirena) | 52-mg system | NA ($215), assuming 5 years of use | Breakthrough bleeding, patient discomfort during placement | ||||
NA = not available.
*—Estimated retail price for one year of treatment based on information obtained at http://www.goodrx.com and http://www.drugs.com (accessed November 9, 2018). Generic price listed first; brand name price in parentheses. Ranges are given to account for dosing variations. Insurance coverage varies.
†—Puberty induction therapies are started in the earlier stages of puberty, generally after puberty suppression. Regimens are available in the 2017 Endocrine Society guideline.B1 They require slow titration from lower initial doses.
‡—Some adolescents in the final stages of puberty (i.e., those not requiring puberty induction), older adults, or nonbinary persons may desire slower dose titration. Patients with a history of high-risk conditions (e.g., thromboembolic disease) may require alternative regimens.
Information from:
B1. Hembree WC, Cohen-Kettenis PT, Gooren L, et al. Endocrine treatment of gender-dysphoric/gender-incongruent persons: an Endocrine Society clinical practice guideline [published correction appears in J Clin Endocrinol Metab. 2018;103(2):699]. J Clin Endocrinol Metab. 2017;102(11):3869–3903.
Coleman E, Bockting W, Botzer M, et al. Standards of care for the health of transsexual, transgender, and gender-nonconforming people, version 7. Int J Transgenderism. 2012;13(4):165–232.
de Vries AL, Klink D, Cohen-Kettenis PT. What the primary care pediatrician needs to know about gender incongruence and gender dysphoria in children and adolescents. Pediatr Clin North Am. 2016;63(6):1121–1135.
Deutsch MB. Guidelines for the primary and gender-affirming care of transgender and gender nonbinary people. 2nd ed. June 17, 2016. http://transhealth.ucsf.edu/protocols. Accessed July 5, 2018.
Olson J, Forbes C, Belzer M. Management of the transgender adolescent. Arch Pediatr Adolesc Med. 2011;165(2):171–176.
Surgery and Other Treatments
Gender-affirming surgical treatments may not be required to minimize gender dysphoria, and care should be individualized.6 Mastectomy (i.e., chest reconstruction surgery) may be performed for transmasculine persons before 18 years of age, depending on consent, duration of applicable hormone treatment, and health status.6 Breast augmentation for transfeminine persons may be timed to maximal breast development from hormone therapy.5,6 Mastectomy or breast augmentation generally costs less than $10,000, and insurance coverage varies.51 Patients may also request referral for facial and laryngeal surgery, voice therapy, or hair removal.5,6,8
The Endocrine Society recommends that persons who seek fertility-limiting surgeries reach the legal age of majority, optimize treatment for coexisting conditions, and undergo social affirmation and hormone treatment (if applicable) continuously for 12 months.6 Adherence to hormone therapy after gonadectomy is paramount for maintaining bone mineral density.6 Despite associated costs, varying insurance coverage, potential complications, and the potential for prolonged recovery,6,8,51 gender-affirming surgeries generally have high satisfaction rates.6,42
Transgender Youth
Most, but not all, transgender adults report stability of their gender identity since childhood.17,52 However, some gender-diverse prepubertal children subsequently identify as gay, lesbian, or bisexual adolescents, or have other identities instead of transgender,8,11,17,53–55 as opposed to those in early adolescence, when gender identity may become clearer.5,8,11,17,43,44,53,55 There is no universally accepted treatment protocol for prepubertal gender-diverse children.6,12,17 Clinicians may preferentially focus on assisting the child and family members in an affirmative care strategy that individualizes healthy exploration of gender identity (as opposed to a supportive, “wait-and-see” approach); this may warrant referral to a mental health clinician comfortable with the lifespan development of transgender youth.6,12,13,21
Transgender adolescents should have access to psychological therapy for support and a safe means to explore their gender identity, adjust to socioemotional aspects of gender incongruence, and discuss realistic expectations for potential therapy.6,8,12,17 The clinician should advocate for supportive family and social environments, which have been shown to confer resilience.14,18,21,40,56,57 Unsupportive environments in which patients are bullied or victimized can have adverse effects on psychosocial functioning and well-being.21,58,59
Transgender adolescents may experience distress at the onset of secondary sex characteristics. Clinicians should consider initiation of or timely referral for a gonadotropin-releasing hormone (GnRH) to suppress puberty when the patient has reached stage 2 or 3 of sexual maturity.5,6,8,17,21,40,44 This treatment is fully reversible, may make future affirmation easier and safer, and allows time to ensure stability of gender identity.6,17 No hormonal intervention is warranted before the onset of puberty.6,8,17
Consent for treatment with GnRH analogues should include information about benefits and risks5,6,8,15,50 (eTable B). Before therapy is initiated, patients should be offered referral to discuss fertility preservation, which may require progression through endogenous puberty.5,6
Some persons prefer to align their appearance (e.g., clothing, hairstyle) or behaviors with their gender identity. The risks and benefits of social affirmation should be weighed.5,6,8,13,17,56 Transmasculine postmenarcheal youth may undergo menstrual suppression, which typically provides an additional contraceptive benefit (testosterone alone is insufficient).5 Breast binding may be used to conceal breast tissue but may cause pain, skin irritation, or skin infections.5
Multiple studies report improved psychosocial outcomes after puberty suppression and subsequent gender-affirming hormone therapy.39–42,44,60 Delayed treatment may potentiate psychiatric stress and gender-related abuse; therefore, withholding gender-affirming treatment in a wait-and-see approach is not without risk.8 Additional resources for transgender persons, family members, and clinicians are presented in eTable C.
eTABLE C Selected Resources for Care of Transgender and Gender-Diverse Persons
| For clinicians | ||
| Center of Excellence for Transgender Health | ||
| Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, 2nd ed. | ||
| National LGBT Health Education Center (provides educational programs, resources, and consultation to health care organizations to optimize care for LGBT persons) | ||
| The Endocrine Society | ||
| Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society Clinical Practice Guideline | ||
| World Professional Association for Transgender Health | ||
| Standards of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People, 7th ed. | ||
| Clinical practice guidelines: | ||
| Assistance in finding transgender-friendly health care professionals: | ||
| For patients and family members | ||
| Colage (unites people with LGBTQ parents) | ||
| Parents, Families and Friends of Lesbians and Gays (committed to advancing equality and full societal affirmation of LGBTQ persons) | ||
| Human Rights Campaign (advocates for the LGBTQ community) | ||
| National Center for Transgender Equality (social justice advocacy for transgender persons) | ||
| The Trevor Project (advocates for the LGBTQ community and hosts a call-in line for transgender youth in crisis) | ||
| Trans Lifeline (hosts a call-in line for transgender persons in crisis) | ||
| TransYouth Family Allies (online resource for parents, youth, and health care professionals) | ||
LGBTQ = lesbian, gay, bisexual, transgender, queer.
Information from Klein DA, Ellzy JA, Olson J. Care of a transgender adolescent. Am Fam Physician. 2015;92(2):142–148.
Data Sources: PubMed searches were completed using the MeSH function with the key phrases transgender, gender dysphoria, and gender incongruence. The reference lists of six cited manuscripts were searched for additional studies of interest, including three relevant reviews and guidelines by the World Professional Association for Transgender Health; the Center of Excellence for Transgender Health at the University of California, San Francisco; and the Endocrine Society. Other queries included Essential Evidence Plus and the Cochrane Database of Systematic Reviews. Search dates: November 1, 2017, to September 18, 2018.
The views expressed in this publication are those of the authors and do not reflect the official policy or position of the Departments of the Army, Navy, or Air Force; the Department of Defense; or the U.S. government.
