Osteochondrosis is a term used to describe a group of disorders that affect the growing skeleton. These disorders result from abnormal growth, injury, or overuse of the developing growth plate and surrounding ossification centers. The exact etiology of these disorders is unknown, but genetic causes, repetitive trauma, vascular abnormalities, mechanical factors, and hormonal imbalances may all play a role. Legg-Calvé-Perthes disease is a hip disorder that causes hip pain, an atraumatic limp, and knee pain. Osgood-Schlatter and Sinding-Larsen–Johannson diseases are common causes of anterior knee pain that is aggravated by jumping activities and kneeling. Sever disease causes heel pain that is exacerbated by activity and wearing cleats. It often mimics Achilles tendinitis and is treated with activity and shoe modifications, heel cups, and calf stretches. Freiberg disease and Köhler bone disease often cause foot pain and are disorders of the metatarsal head and navicular bone, respectively. Radiographs show sclerosis, flattening, and fragmentation of bone in both diseases. Elbow pain can be caused by medial epicondyle apophysitis or Panner disease. Medial epicondyle apophysitis is exacerbated by frequent throwing and is treated with throwing cessation and acetaminophen or nonsteroidal anti-inflammatory drugs. Panner disease is the most common cause of lateral-sided elbow pain in children younger than 10 years. It may or may not be associated with frequent throwing, and it resolves spontaneously. Scheuermann disease causes back pain and a humpback deformity from vertebral bone anterior wedging.
The term osteochondrosis is used to describe a group of disorders that affect patients with an immature skeleton. The etiology of joint pain in these patients is often from osteochondrosis, although traumatic, inflammatory, or infectious origins should be ruled out as well. Osteochondrosis results from abnormal development, injury, or overuse of the growth plate and surrounding ossification centers. Overall, boys are more affected and symptoms generally appear between 10 and 14 years of age.1 It is thought that boys are more commonly affected because of their greater susceptibility to childhood trauma and overuse injuries.2 Patients usually present with pain and disability. Areas of the body most often affected include the hip, knee, foot, elbow, and back (Figure 1).
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendation | Evidence rating | References |
|---|---|---|
| Osgood-Schlatter disease is a self-limited process that responds well to activity modification and nonsteroidal anti-inflammatory drugs. Physical therapy may help reduce symptoms in recalcitrant cases. | C | 10–12, 15 |
| Sever disease responds well to nonoperative treatment consisting of activity and shoe modifications, padded heel cups, and calf stretches. | C | 20–22 |
| Medial epicondyle apophysitis is best treated with prevention. Parents, coaches, and players should adhere to the guidelines set forth by the Little League Association of America to maintain the health of young, throwing athletes. | C | 31, 32, 34 |
| The primary indications for surgical treatment of Scheuermann disease are to alleviate pain and to improve cosmesis. However, the deformity is of little functional consequence and does not progress severely after skeletal maturity. | C | 39, 45–47 |
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, diseaseoriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.xml.
Figure 1. Common Locations of Osteochondrosis in Patients with Immature Skeletons
Areas of the body most often affected by osteochondrosis.
A distinction between osteochondrosis and osteochondritis dissecans lesions should be made, which can be a common source of confusion for physicians. Osteochondritis dissecans is an inflammatory condition of bone and overlying articular cartilage that affects the joints of patients with immature and mature skeletons alike. Either condition may present with activity-related pain, but osteochondritis dissecans may also cause joint catching and locking. Lesions from osteochondritis dissecans may or may not resolve with nonoperative treatment, whereas osteochondrosis eventually resolves when the growth plates have closed and skeletal maturity has been reached.
Hip Pain
LEGG-CALVÉ-PERTHES DISEASE
Legg-Calvé-Perthes disease is a hip disorder that results from a partial interruption of the blood supply to the immature femoral head. The exact cause of the vascular interruption is unknown. It occurs in children between four and eight years of age. Boys are four to five times more likely to be affected than girls.3,4 There is an increased incidence in patients with low birth weight, abnormal birth presentation, family history, higher birth order, and lower socioeconomic status.5,6 Patients present with hip pain, an atraumatic limp, and referred pain in the knee. Limited hip abduction, internal rotation, and leg-length discrepancies are commonly found on physical examination. Anteroposterior and frog-leg lateral radiographs will demonstrate varying degrees of fragmentation, flattening, and sclerosis of the proximal femur growth center with joint space widening. Other conditions, including septic arthritis and osteomyelitis of the proximal femur, should be ruled out in equivocal cases.
If patients are treated early, they have a lower risk of developing arthritis at a young age, and range of motion can be preserved. Poor prognostic factors include age older than six years at onset of disease, greater extent of femoral head deformity, hip joint incongruity, and decreased hip range of motion.7,8 A prospective, nonrandomized trial found no difference in outcomes when physical therapy and bracing were used in children younger than six years.9 Surgical treatment consists of reconstructive procedures to improve hip joint congruity.
Knee Pain
OSGOOD-SCHLATTER DISEASE
Osgood-Schlatter disease, an inflammatory condition, is a common cause of anterior knee pain in children and adolescents. It is caused by repetitive traction of the patellar tendon on the tibial tubercle ossification center or apophysis, which may cause substantial inflammation and pain. Symptomatic patients are usually between 10 and 14 years of age, and up to 30 percent of patients will have bilateral involvement.10,11 Nearly 50 percent of patients are involved in regular athletic activity.12 Pain is often exacerbated by jumping activities and direct pressure, such as kneeling. Patients have moderate to severe tenderness, swelling, and prominence over the tibial tubercle. The diagnosis is often made clinically, although plain radiographs should be obtained to rule out fractures, tumors, or osteomyelitis if the presenting signs and symptoms are atypical. Radiographs of patients with Osgood-Schlatter disease may show anterior soft tissue swelling and fragmentation of the tibial tubercle. Magnetic resonance imaging and ultrasonography are not routinely necessary.13
Osgood-Schlatter disease is a self-limited process that responds well to activity modification and acetaminophen or nonsteroidal anti-inflammatory drugs (NSAIDs). Stretching and physical therapy to improve flexibility of lower-extremity muscles can help reduce symptoms. Some case series have shown that operative treatment can alleviate symptoms in patients with mature skeletons who continue to have disabling symptoms.14,15
SINDING-LARSEN–JOHANSSON DISEASE
Sinding-Larsen–Johansson disease is another common cause of anterior knee pain in children and adolescents. It is similar to Osgood-Schlatter disease, except that Sinding-Larsen–Johansson disease occurs at the inferior pole of the patella. Affected patients are between 10 and 13 years of age and are often involved in athletic activities.16 Symptoms are aggravated by jumping or direct pressure over the inferior pole of the patella. Point tenderness is localized to the inferior pole of the patella. Although it is diagnosed clinically, radiographs should be obtained to rule out other pathology. Radiographs may show soft-tissue swelling and calcification of an avulsed portion of the patella.
Sinding-Larsen–Johansson disease is a self-limited process that responds to activity modification and acetaminophen or NSAIDs. Knee immobilization is only necessary in severe cases. Exercises to improve flexibility of the hamstrings, quadriceps, and heel cords can help reduce symptoms.17 Symptoms usually resolve within 10 to 12 months, and the condition is rare after skeletal maturity.18
Foot Pain
SEVER DISEASE
Sever disease, or calcaneal apophysitis, is a common cause of heel pain in young athletes. The Achilles tendon exerts tensile forces on the calcaneal apophysis with physical activity. Most patients associate their symptoms with a particular sport, with soccer being the most common.19 Symptoms are worse at the beginning of a new sports season or during a growth spurt. Weight-bearing activity and shoes, particularly soccer cleats, can aggravate the symptoms. Physical examination often reveals point tenderness at the insertion of the Achilles tendon, tight heel cords, and heel pain with medial-lateral compression.20 Plain radiographs look normal.
Nonoperative treatment includes activity and shoe modifications, padded heel cups, and calf stretches. Patients with persistent symptoms despite activity modification and a stretching program should have other conditions considered, such as Achilles tendinitis, plantar fasciitis, or a calcaneal stress fracture.21,22
FREIBERG DISEASE
Freiberg disease is a painful condition of the forefoot occurring most often in adolescent girls who participate in ballet and dance.23 The exact etiology is unknown, but it is commonly characterized by disordered ossification of the second metatarsal head. Possible causes include trauma, repetitive stress, disruption in blood supply, or improper shoe wear.24,25 Bilateral involvement occurs in less than 10 percent of patients.25 Pain is exacerbated by weight-bearing and athletic activities. Point tenderness and swelling are commonly found over the affected metatarsal head. Plain radiographs show sclerosis and varying degrees of flattening of the affected articular surface. In most patients, nonoperative treatment consisting of activity modification, metatarsal pads, and well-padded shoes facilitates regeneration of the metatarsal head and spontaneous resolution of symptoms.26
KÖHLER BONE DISEASE
Köhler bone disease is an osteochondrosis of the navicular bone in the foot. Patients often present between two and eight years of age, and boys are three to five times more likely to be affected.27 The etiology is unknown, and there is usually no history of previous trauma. Mid-foot pain and a limp are the most common presenting symptoms. There is point tenderness over the navicular bone on examination.27 There may be mild swelling and warmth over the dorsal midfoot.28 The diagnosis is mainly clinical; however, plain radiographs usually demonstrate navicular sclerosis, flattening, and fragmentation.28 It is a self-limited condition and symptoms will eventually resolve.27,29 Recent reviews have shown that a short leg cast for up to eight weeks accelerates resolution of symptoms, although long-term outcomes are favorable regardless of treatment.27,30
Elbow Pain
MEDIAL EPICONDYLE APOPHYSITIS
Medial epicondyle apophysitis affects throwing athletes, such as pitchers. Frequent throwing results in repetitive stress across the medial epicondyle growth plate.31,32 Patients present with pain localized directly over the medial epicondyle. Tenderness may be mild in early apophysitis, but can be severe if there is an avulsion fracture. The shoulder also should be examined because this condition can be a symptom of shoulder pathology. Plain radiographs may show fragmentation of the medial epicondyle.
Prevention is the best treatment for this condition and should include pitch limits, with limitation of curveballs and sliders in particular.33–35 Descriptive studies have shown that pitching curveballs and sliders exerts excessive torque across the shoulder and elbow joints, respectively.34,36 Successful treatment typically consists of ice, acetaminophen or NSAIDs, and throwing cessation.37 Surgical management is generally not necessary, but may be reserved for widely displaced avulsion fractures.
PANNER DISEASE
Panner disease is the most common cause of lateral-sided elbow pain in children younger than 10 years.38 It is characterized by abnormal ossification, necrosis, and degeneration of the distal humeral ossification center (capitellum). It may or may not be associated with athletic activity. Patients present with vague, lateral-sided elbow pain without point tenderness. Plain radiographs often show fragmentation and fissuring of the entire humeral capitellum. Panner disease is self-limited and generally resolves spontaneously with rest and conservative management, including acetaminophen or NSAIDs.
Back Pain
SCHEUERMANN DISEASE
Scheuermann disease is a common cause of back pain with a rigid kyphosis or humpback deformity. Disturbance of the vertebral end plates causes anterior vertebral body wedging that results in kyphosis during a growth spurt. The exact etiology of this growth disturbance is unknown.39–42 Age of onset is between 10 and 12 years. Pain and increasing back deformity are the most common presenting symptoms. Physical examination findings include a rigid, humpback deformity that does not correct with back extension (Figure 2). Signs of nerve compression are rare.43 Anteroposterior and lateral radiographs of the spine with the patient standing reveal at least 5 degrees of wedging in at least three adjacent vertebrae44 (Figure 3). Disk space narrowing, end plate irregularities, and scoliosis also may be seen. The deformity increases during adolescent growth spurts, but progression after skeletal maturity is not severe.45,46 Postural roundback is a similar disorder that can be differentiated from Scheuermann disease because patients with postural roundback show no abnormalities on radiographs and their deformity can be corrected with changes in posture or position.
Figure 2.
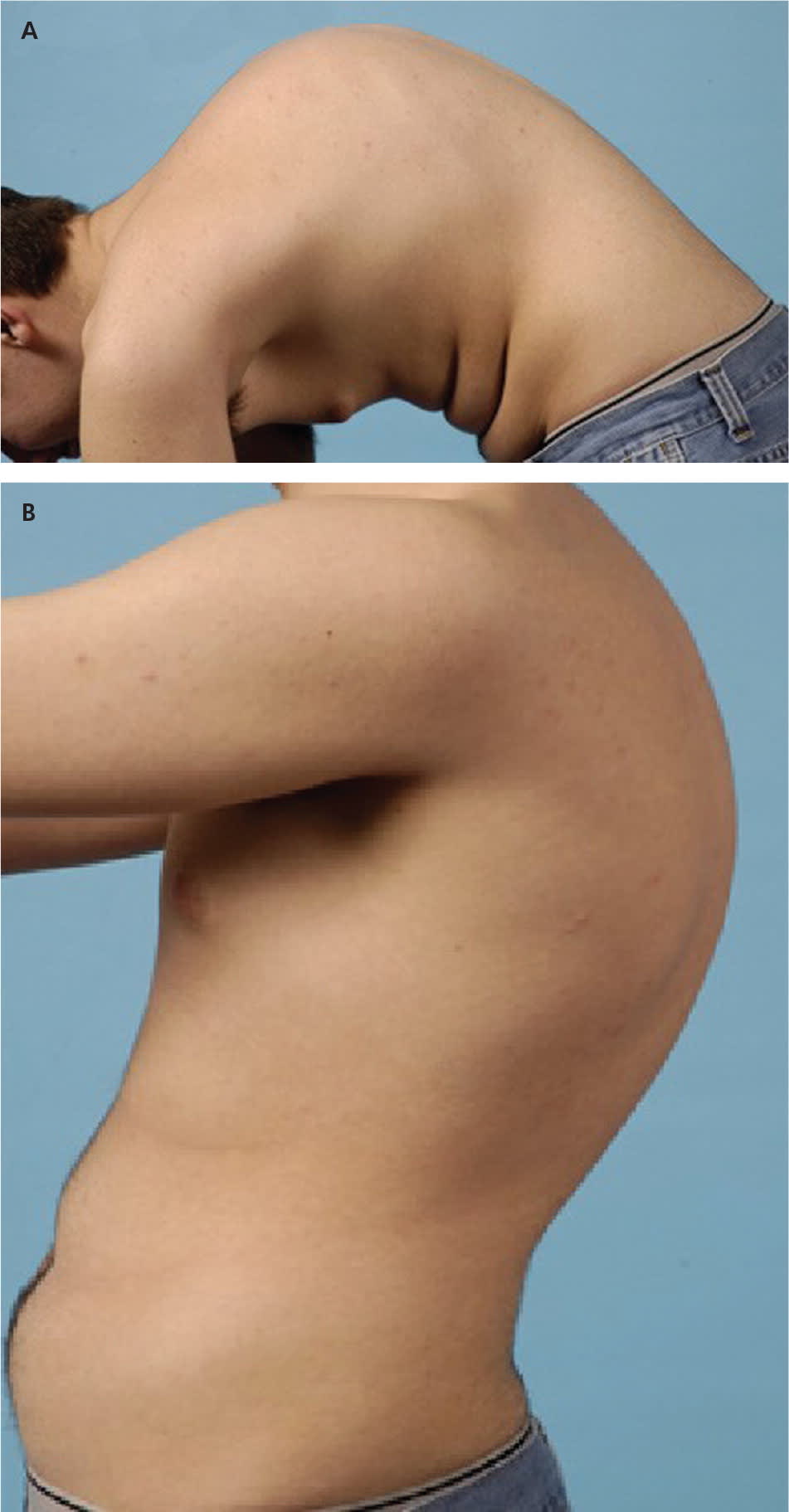
Patient with typical Scheuermann disease presentation: prominent posterior humpback deformity (A) that does not correct with hyperextension (B).
Figure 3.
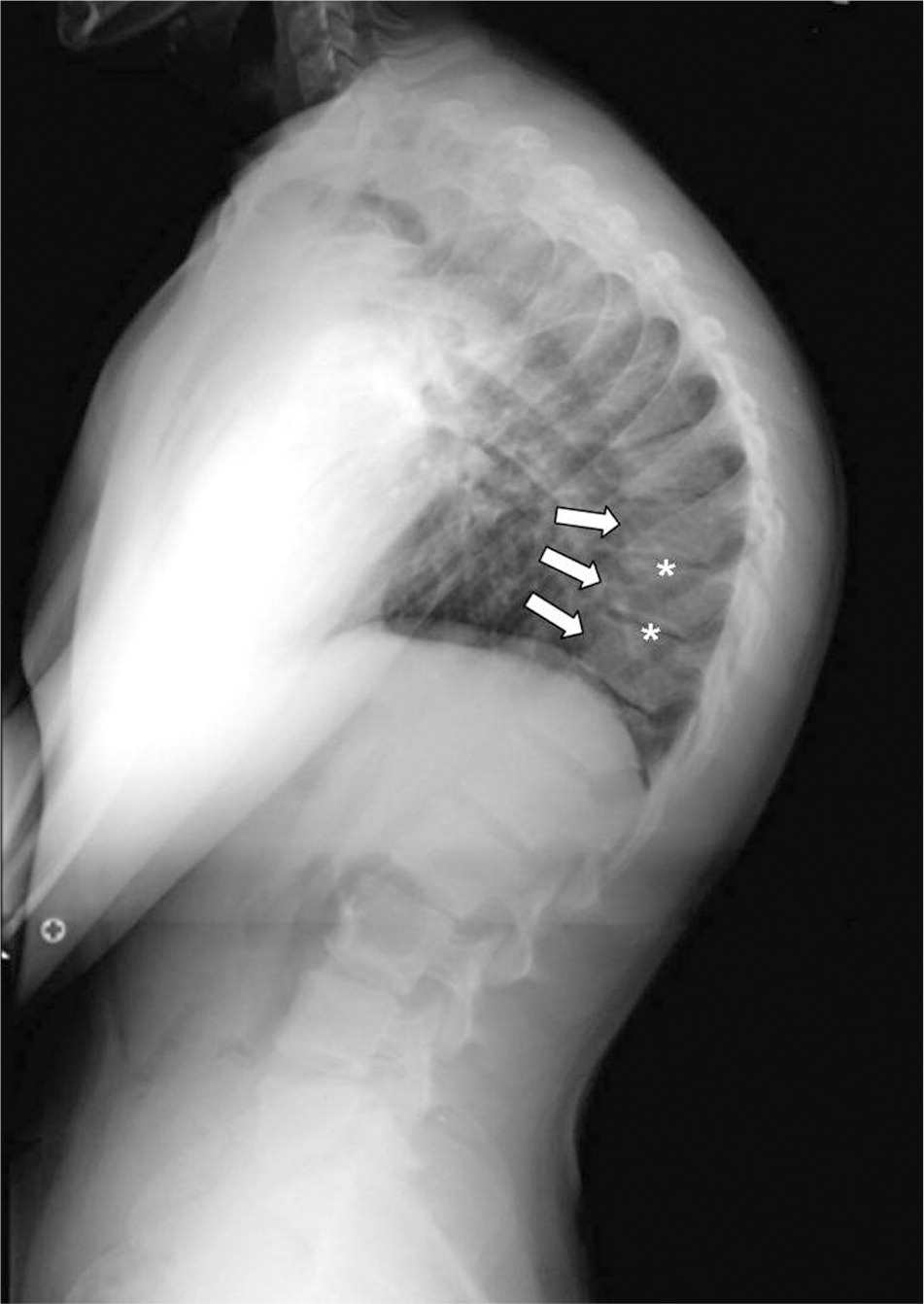
Lateral thoracolumbar radiograph of an adolescent with Scheuermann disease showing vertebral end plate abnormalities (asterisks) and anterior vertebral body wedging (arrows).
A recent evidence-based review found that most patients with Scheuermann disease do not need surgical intervention, which should be reserved only for patients with mature skeletons who have a curve greater than 75 degrees, pain, a rigid deformity, and unacceptable appearance.47 Bracing is indicated in patients who have an immature skeleton with an increasing curve.
Orthopedic Referral
Patients with osteochondrosis should be referred to an orthopedic surgeon for further evaluation if nonoperative treatment has not been effective. Patients with Osgood-Schlatter disease, Sinding-Larsen–Johannson disease, or Sever disease who have mature skeletons and disabling symptoms should be referred. Those with Freiberg disease and loose joint fragments should be referred for possible joint debridement. Patients suspected of having Köhler bone disease who have had recent trauma, illness, or elevated inflammatory markers should be referred to rule out infection or occult fracture. Referral is also indicated in those with medial epicondyle apophysitis or Panner disease who have acute trauma, pain despite several weeks of rest, or loose joint fragments. Any patient suspected of having Legg-Calvé-Perthes disease or Scheuermann disease should be referred for further evaluation.
A summary of diagnostic, treatment, and referral indications for each osteochondrosis disorder is provided in Table 1.
Table 1. Summary of Osteochondrosis Disorders
| Disorder | Clinical presentation | Radiograph findings | Initial treatment | Orthopedic referral |
|---|---|---|---|---|
| Legg-Calvé-Perthes disease | Atraumatic limp; hip and knee pain | Sclerosis, flattening, and fragmentation of proximal femur growth center | — | Any patient with suspected Legg-Calvé-Perthes disease |
| Osgood-Schlatter disease | Pain at anterior tibial tubercle with activity and kneeling | Soft tissue swelling and fragmentation of tibial tubercle | Activity modification; acetaminophen or NSAIDs | Patients with a mature skeleton who have persistent symptoms |
| Sinding-Larsen–Johansson disease | Pain at inferior patellar pole with activity and kneeling | Soft tissue swelling and calcification of inferior pole of patella | Activity modification; acetaminophen or NSAIDs | Patients with a mature skeleton who have persistent symptoms |
| Sever disease | Posterior heel pain with activity and shoe wear | Plain radiographs are usually normal | Activity and shoe modifications; heel cups; calf stretches; acetaminophen or NSAIDs | Patients with a mature skeleton who have persistent symptoms |
| Freiberg disease | Metatarsal head pain and swelling | Sclerosis, flattening, and fragmentation of metatarsal head | Activity modification; metatarsal pads; well-padded shoes | Patients with metatarsophalangeal joint arthritis and loose joint fragments |
| Köhler bone disease | Midfoot pain and limp | Sclerosis, flattening, and fragmentation of navicular bone | Cast immobilization for up to eight weeks | Patients with recent trauma, illness, or elevated inflammatory markers |
| Medial epicondyle apophysitis | Localized pain over medial epicondyle with throwing | May show fragmentation or widening of medial epicondyle | Throwing cessation; acetaminophen or NSAIDs | Patients with acute avulsions or continued symptoms despite rest |
| Best prevention is monitored throwing in young athletes | ||||
| Panner disease | Vague, lateral-sided elbow pain | Flattening and fragmentation of humerus capitellum | Rest; acetaminophen or NSAIDs | Patients with loose joint fragments |
| Scheuermann disease | Back pain and humpback deformity | Anterior wedging of three adjacent vertebrae and end plate irregularities | — | Any patient with suspected Scheuermann disease |
NSAIDs = nonsteroidal anti-inflammatory drugs.
