Central retinal artery occlusions, chemical injuries, mechanical globe injuries, and retinal detachments are eye emergencies that can result in permanent vision loss if not treated urgently. Family physicians should be able to recognize the signs and symptoms of each condition and be able to perform a basic eye examination. Patients with a central retinal artery occlusion require urgent referral for stroke evaluation and should receive therapy to lower intraocular pressure and vasodilating agents to minimize retinal ischemia. Chemical injuries require immediate irrigation of the eye to neutralize the pH of the ocular surface. A globe laceration or rupture is common in patients with a recent history of trauma from a blunt or penetrating object. Physicians should administer prophylactic oral antibiotics after a globe injury to prevent endophthalmitis. The eye should be covered with a metal shield until evaluation by an ophthalmologist. Patients with symptomatic floaters and flashing lights should be referred to an ophthalmologist for a dilated funduscopic examination to evaluate for a retinal tear or detachment.
Central retinal artery occlusions (CRAOs), chemical injuries, mechanical globe injuries, and retinal detachments are ocular emergencies that have the potential to cause permanent vision loss if they are not promptly recognized and treated (Table 11–14 ). Family physicians should be familiar with the signs and symptoms associated with each condition and be able to perform a basic eye examination. American Family Physician's topic module on eye and vision disorders discusses other urgent ocular conditions (https://www.aafp.org/afp/eyedisorders).
SORT: KEY RECOMMENDATIONS FOR PRACTICE
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.
TABLE 1. Management of Eye Emergencies
| Emergency | Signs and symptoms | Initial evaluation | Ophthalmic management |
|---|---|---|---|
| Central retinal artery occlusion | Acute, painless loss of vision; amaurosis fugax; retinal whitening with foveal cherry-red spot | Assess visual acuity; perform dilated funduscopic examination Presence of a cherry-red spot in the fovea; unilateral, painless vision loss of hand motion or light perception; evaluate for stroke; echocardiography; electrocardiography; carotid artery ultrasonography; obtain erythrocyte sedimentation rate and C-reactive protein level; immediately refer to an ophthalmologist1 | Nonarteritic causes: treat with digital massage, anterior chamber paracentesis, systemic acetazolamide, pentoxifylline (Trental), intra-arterial thrombolysis Arteritic causes: treat with a high dose of systemic steroids2–4 |
| Chemical eye injury | Eye pain; decreased vision; conjunctival redness or ischemia; corneal clouding or abrasion | Assess visual acuity; examine cornea for clarity and conjunctiva for hyperemia; determine the chemical agent Immediately irrigate eye with normal saline or lactated Ringer solution with at least 2 L of fluid; immediately refer to an ophthalmologist5 | Topical antibiotics and artificial tears for mild ocular burns; topical antibiotics, artificial tears, steroids, ascorbate, citrate drops, or amniotic membrane tissue for severe burns6,7 |
| Mechanical globe injury | Decreased vision; conjunctival or corneal laceration; subconjunctival hemorrhage; ocular foreign body; hyphema or shallow anterior chamber; irregular shaped pupil or iris prolapse | Assess visual acuity, pupils, cornea, and anterior chamber Decreased visual acuity, irregular shaped pupil, iris prolapse through corneal or scleral laceration, presence of penetrating foreign body Place metal shield over eye; provide antiemetics and systemic antibiotics (levofloxacin [Levaquin], ceftazidime [Fortaz], or vancomycin); update Tdap vaccine; immediately refer to an ophthalmologist8–10 | Evaluate for orbital fractures and intraocular foreign bodies with computed tomography; schedule immediate surgical repair of laceration; monitor for endophthalmitis and sympathetic ophthalmia8 |
| Posterior vitreous detachment, retinal tear, retinal detachment | Sudden onset of flashing lights and floaters in one eye; peripheral or central visual field defect | Assess visual acuity; perform confrontational visual field testing and dilated funduscopic examination Decreased visual acuity, constricted visual fields, or patients with risk factors including myopia, age ≥ 50 years, prior detachment in the contralateral eye, prior ocular surgery, or family history may represent a retinal tear or detachment; refer to an ophthalmologist within 24 hours11,12 Unaffected visual acuity, full confrontational visual fields, or no known risk factors may represent a posterior vitreous detachment; refer to an ophthalmologist within a few days12 | Observe for posterior vitreous detachment and instruct patient to seek prompt reevaluation for increased floaters, flashing lights, or a new peripheral visual field defect Laser for small retinal tear; surgical repair with pneumatic retinopexy; scleral buckle or vitrectomy for retinal detachment11,13,14 |
Tdap = tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis.
Central Retinal Artery Occlusion
CASE SCENARIO
A 76-year-old man presents with acute, painless vision loss in his left eye during the course of 10 minutes. His visual acuity is light perception. Confrontational visual fields reveal a dense scotoma, and a penlight examination shows an afferent pupillary defect.
BACKGROUND
The annual incidence of a CRAO is approximately one in 100,000 people with a mean age in their early 60s.15 CRAO is caused by an inflammatory, embolic, or thromboembolic obstruction of the central retinal artery that supplies the macula and central retina. Most CRAOs are nonarteritic and are caused by platelet fibrin thromboemboli in the setting of atherosclerotic disease. Risk factors include hypertension, diabetes mellitus, carotid artery disease, coronary artery disease, and tobacco use.16 Arteritic CRAO accounts for less than 5% of cases and is often attributed to giant cell arteritis.16
DIAGNOSIS
Patients with a CRAO commonly present with rapid, painless vision loss and an afferent pupillary defect. Dilated funduscopic examination usually shows retinal whitening with a cherry-red spot in the fovea (Figure 1). A Hollenhorst plaque (i.e., white punctate-appearing cholesterol emboli) may be visible at the branching points of blood vessels on the optic nerve.
FIGURE 1.
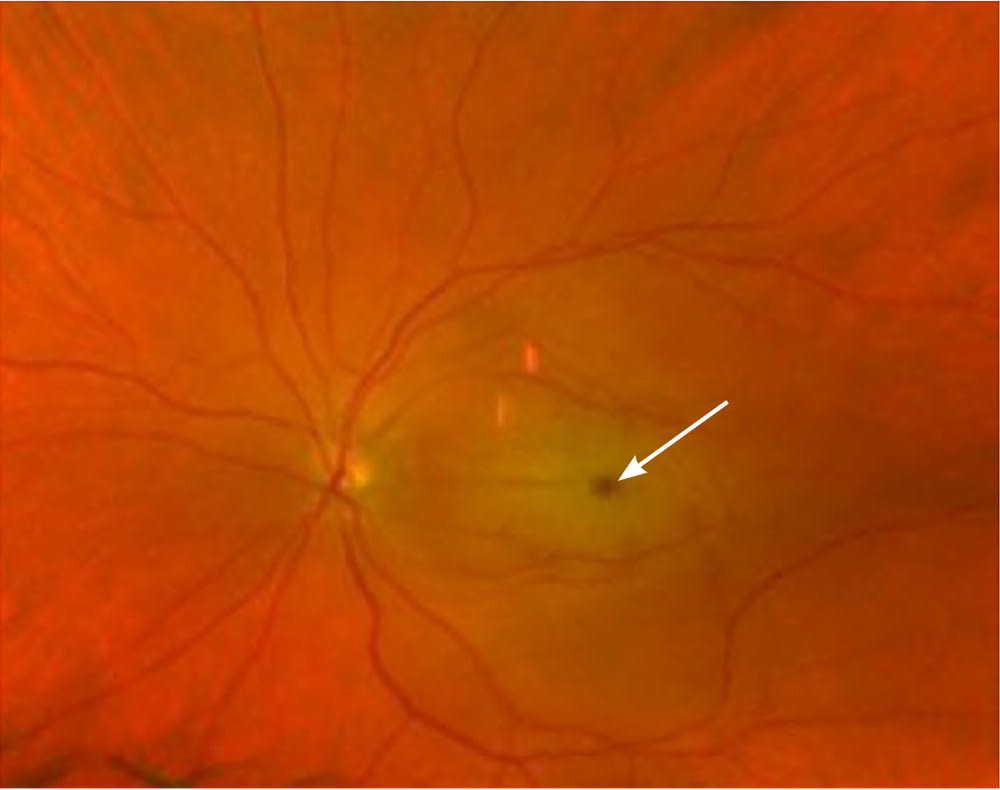
Funduscopic view of the eye demonstrating a central retinal artery occlusion with a cherry-red spot (arrow) in the fovea indicating retinal ischemia.
TREATMENT
The standard initial treatment includes ocular massage, anterior chamber paracentesis, vasodilating agents to minimize retinal ischemia, and ocular hypotensive agents including acetazolamide; however, they do not affect the natural course of the disease.2 The administration of pentoxifylline (Trental; three 600-mg tablets per day) has the potential to improve retinal blood flow.3 Intra-arterial thrombolysis has produced favorable outcomes compared with standard therapy.4
Patients diagnosed with a CRAO should be evaluated for possible stroke because of the elevated risk of a subsequent ischemic event. Echocardiography and electrocardiography can be used to determine cardiac function, and carotid artery ultrasonography to assess for stenosis.1
An erythrocyte sedimentation rate and C-reactive protein level should be obtained for patients older than 50 years with symptoms of fever, fatigue, jaw tenderness, scalp tenderness, and weight loss in whom giant cell arteritis is suspected. If the patient's levels are elevated, systemic steroids are recommended. Patients younger than 50 years should receive a hypercoagulable workup to assess for antiphospholipid antibody syndrome and other hypercoagulable diatheses.1
PROGNOSIS
There are no proven therapies that improve vision outcomes after a nonarteritic CRAO. Most patients have a final visual acuity of 20/400 or worse.17 Follow-up should include screening for cerebrovascular complications.
Chemical Injury
CASE SCENARIO
A 34-year-old man presents with eye pain, tearing, and decreased vision in his right eye two hours after spraying liquid fertilizer on plants. His visual acuity on presentation is 20/200, and a penlight examination shows swollen upper and lower eyelids, conjunctival injection, and an opaque cornea.
BACKGROUND
Chemical eye injuries occur when the ocular surface is exposed to an acid or alkali in the form of a liquid, powder, or gas. The severity of the injury is dependent on the chemical's pH concentration and the duration of contact with the ocular surface.18 Chemical burns may cause ischemic damage to conjunctival vessels and corneal limbal stem cells, resulting in conjunctival scarring and corneal opacification. Alkali burns are more common because of the prevalence of alkali in household cleaning agents and are more harmful than acid burns because alkali agents penetrate the ocular surface more quickly.19,20
DIAGNOSIS
Patients with a chemical eye injury commonly present with eye pain, redness, tearing, sensitivity to light, and decreased vision. The physician should identify the type of chemical involved and the amount that came in contact with the eye to evaluate for severity of the injury.
Examination of the external and anterior segments of the eye may reveal swelling and burns to the eyelids; a cloudy cornea or epithelial defect; conjunctival injection; or a white eye, indicating conjunctival ischemia. Initial pH testing of the ocular surface may be performed by placing a strip of litmus paper in the conjunctival fornix.
TREATMENT
Treatment for a chemical injury to the eye should be initiated immediately because of the potential for permanent damage and vision loss. Initial treatment involves liberal irrigation with lactated Ringer solution, normal saline, or water if other solutions are not available.5 The eye should be irrigated with at least 2 L of fluid using a lens irrigation system or intravenous tubing (https://www.youtube.com/watch?v=nefq2XvyZxU). The pH of the ocular surface should be remeasured five minutes after initial irrigation. The fornices are swept with a wet cotton swab to remove any retained crystallized chemical particles. Further irrigation is necessary if the pH of the ocular surface has not been neutralized (7.0 to 7.5).5
Once the ocular surface has been neutralized, the patient should be referred immediately to an ophthalmologist. For mild burns with minimal or no corneal epithelial defects (i.e., abrasions), treatment with antibiotic eye drops and preservative-free artificial tears may be effective.6 More severe burns with corneal opacities or white-appearing limbal ischemia (i.e., junction between the cornea and sclera) require topical antibiotics, steroids, ascorbate, citrate, autologous serum drops, and amniotic membrane tissue to reduce inflammation and promote epithelialization.7
PROGNOSIS
The prognosis depends on how much time elapsed between the chemical injury and eye irrigation. Immediate irrigation of the eye results in less damage to the ocular surface and better vision outcomes.5 Visual acuity following a chemical injury may achieve 20/40 or better in 100% of patients with mild corneal epithelial defects, compared with 60% of patients who have corneal opacities and limbal ischemia.6 At follow-up, the patient should be monitored for elevated intraocular pressure, corneal opacities, and eyelid abnormalities.
Mechanical Globe Injury
CASE SCENARIO
A 28-year-old man presents with acute pain in his right eye, redness, and loss of vision after using a nail gun. His visual acuity on presentation is 20/100. A penlight examination reveals an irregular pupil with a penetrating corneal foreign body.
BACKGROUND
Mechanical globe injuries occur from a full-thickness rupture or laceration through the cornea or sclera.21 Globe ruptures occur after blunt injury to the eye from a trauma such as a thrown ball, airbag injury, or assault. Globe lacerations occur after trauma from a penetrating object (e.g., knife, high-velocity projectile). The annual incidence of mechanical globe injuries is 3.8 in 100,000 people, with most of the injuries occurring in the workplace or during recreational activities.22
DIAGNOSIS
Patients with a mechanical globe injury will experience eye pain, redness, tearing, or decreased vision soon after trauma to the eye.
Anterior segment examination with a slit lamp can identify an injury to the globe; however, a penlight may also be used. Findings can include subconjunctival hemorrhage, irregular pupil, and iris prolapse through a corneal or scleral wound. If a foreign body is visible and protruding out of the globe, it should not be removed (Figure 2). Removal could cause globe collapse and hypotony. Pharmacologic pupillary dilation and intraocular pressure measurement are not recommended. A wet fluorescein dye strip can be applied near the site of a possible rupture or laceration for examination under a cobalt blue light. Dilution of the fluorescein by aqueous flow from the eye indicates an injury to the globe. Computed tomography of the orbits can evaluate for concomitant intraocular foreign bodies or orbital wall fractures.8
FIGURE 2.

External photograph (A) frontal view and (B) side view of a penetrating corneal foreign body from a nail gun injury.
TREATMENT
Interventions should be initiated to prevent an increase in intraocular pressure if a globe injury is diagnosed or suspected. The patient should be instructed to prevent Valsalva maneuvers, including coughing or straining, and avoid placing external pressure on the eye to prevent extrusion of intraocular contents. Antiemetics should be administered to prevent emesis. A metal shield should be placed over the eye, and the patient should be immediately referred to an ophthalmologist.5
Posttraumatic endophthalmitis, attributed commonly to Bacillus, Streptococcus, and the coagulase-negative Staphylococcus species, may occur in up to 8% of cases when an associated intraocular foreign body is present.23 Prophylactic systemic antibiotics are recommended to reduce the risk of endophthalmitis after a mechanical globe rupture or laceration.9,10 Levofloxacin (Levaquin; 500 mg orally every 12 hours) is an appropriate first-line medication; however, intravenous vancomycin (1 g every 12 hours) or ceftazidime (Fortaz; 1 g every eight hours) is an acceptable alternative.9,10 Antifungal therapy with voriconazole (Vfend; 200 mg orally every 12 hours) or fluconazole (Diflucan; 200 mg orally every 12 hours) may be considered if plant or organic matter is involved.9 A tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis (Tdap) vaccine booster should also be administered.
Surgical repair of the globe injury and removal of intraocular foreign bodies reduce the risk of endophthalmitis when surgery is performed within 24 hours of the injury.10 Therefore, patients with suspected globe injury should be referred immediately to an ophthalmologist.
PROGNOSIS
Favorable vision recovery following an open globe injury is associated with initial visual acuity better than 20/400. The presence of an afferent pupillary defect or posterior wound location indicates poor vision outcomes.24 Follow-up after a globe injury should include monitoring for sympathetic ophthalmia (i.e., intraocular inflammation in the contralateral eye), which, although rare, may lead to profound vision loss.
Retinal Detachment
CASE SCENARIO
A 60-year-old woman presents with several new floaters and a series of flashing lights in her right eye. She noticed a progressively enlarging black spot in her superior visual field during the past two days. Her visual acuity on presentation is 20/25 with a dense superior scotoma on confrontational visual field testing.
BACKGROUND
A retinal detachment occurs when the neurosensory layer of the retina is separated from the underlying retinal pigment epithelium. Retinal detachment is commonly preceded by a posterior vitreous detachment, which occurs when the vitreous body separates from the retina. This causes traction on the retina and potentially creates a tear that may allow the liquefied vitreous to seep through the tear and underneath the retina, causing it to detach. Detached retinas may be localized initially, but without treatment, detachments can progress to involve a larger area of the retina and cause irreversible vision loss. The mean annual incidence of retinal detachments is approximately 10 in 100,000 people.25 Risk factors include age 50 years and older, ocular trauma or surgery, myopia, family history, and a previous detachment in the contralateral eye.26
DIAGNOSIS
Patients with a retinal detachment may notice unilateral flashing lights in their peripheral vision, followed by an increase in floaters. These symptoms may be attributed to a posterior vitreous detachment; however, 14% of patients develop a retinal tear.11 Visual acuity may be unaffected with a retinal tear, but confrontational visual field testing may detect a peripheral visual field defect. If untreated, a retinal detachment may occur, causing a visual field defect in the peripheral vision that enlarges over the next few days. If the detachment is large enough to involve the macula, the patient may have a significant decline in vision.
A dilated funduscopic examination can identify a retinal detachment. A retinal tear may be difficult to detect with direct ophthalmoscopy; however, the surrounding retina will appear elevated (Figure 3). Ocular ultrasonography has a 94% sensitivity in diagnosing a retinal detachment if the retina cannot be visualized because of cataract or vitreous hemorrhage.27
FIGURE 3.

Funduscopic view of the eye demonstrating a large, elevated, inferior retinal detachment (arrow) without a detectable retinal tear.
TREATMENT
Immediate ophthalmology referral is indicated for patients with symptoms such as flashing lights, floaters, or visual field defect, or if a retinal detachment is detected on initial examination.12 Surgical treatment involves sealing the retinal tear with a laser and reapproximating the retina to the underlying choroid with an intraocular gas bubble or scleral buckle. Surgery is successful for more than 95% of patients.13,14
PROGNOSIS
The best predictor of positive vision outcomes after a retinal detachment is if the macula is attached at the time of diagnosis. Delayed repair is associated with poor vision outcomes.28 If the macula is attached, the repair of a retinal detachment results in a final visual acuity of at least 20/40 in approximately 75% of patients, compared with 40% of patients with a detached macula.29 Patients with a retinal detachment are at risk of developing a subsequent detachment in the contralateral eye; therefore, regular follow-up is recommended.30
This article updates previous articles on this topic by Gelston,31 and Pokhrel and Loftus.32
Data Sources: A search of PubMed, Essential Evidence Plus, the Cochrane database, the Agency for Healthcare Research and Quality, and the U.S. Preventive Services Task Force was conducted using the keywords retinal detachment, mechanical globe injury, posttraumatic endophthalmitis, ocular burn, and central retinal artery occlusion. The search included meta-analyses, randomized controlled trials, and systematic reviews. Search dates: September 30, 2019; October 16 and 20, 2019; and April 19, 2020.
